Multidrug Resistant Pneumonia: A Case Study
Pneumonia is an infectious disease, in which the lungs are affected by pathological microorganisms, which are most often bacteria or viruses. As a result of advances in experimental therapeutics, many promising therapies for pneumonia are emerging. The first line agents according to WHO guidelines are penicillins. Many other drugs such as macrolides, carbepenes, tetracyclines, cephalosporines, floroquinolones and aminoglycosides are also used. Some major side effects such as Q-T interval prolongation caused by moxifloxacin and macrolides, tetracycline’s cause teeth discoloration, photosentivity, growthretardation, aminoglycosides cause ototoxicity and nephrotoxicity. It’s important to note that alteration in doses of drugs used in treatment depending upon individual condition prove helpful in reducing these complications. If a patient is resistant to one drug an alternative drug therapy is suggested or employed.
Introduction
Pneumonia is defined as inflammation of lung parenchyma of infective origin and characterized by consolidation. It is an infectious disease in which the lungs alveoli are filled with fluid which causes difficulty in breathing and oxygen levels in body decrease. The symptoms associated with pneumonia arechills, fever, cough (possibly with sputum production), difficulty in breathing, chest pain, wheezing, increase rate of breathing, fatigue. A wide range of organisms cause pneumonia. It is classified into lobar pneumonia, broncho pneumonia. The pneumonia is classified according to place of origin is Community acquired pneumonia (CAP) and Hospital Acquired Pneumonia (HAP). As a result of advances in experimental therapeutics, many promising therapies for Pneumonia are emerging. The empiric therapy for pneumonia mostly starts with amoxicillin. Diagnosis of pneumonia is done through x-ray, physical examination, atrial blood gas, and bronchoscopy. The rapid emergence of resistant bacteria is occurring worldwide and this resistance is a big threat to everyone. The antibiotic resistance crisis is due to overuse or misuse of the antibiotic. WHO make some guidelines or protocols to treat pneumonia. The initial antibiotic therapy regimens vary from country to country. According to WHO guidelines first line agents are penicillin’s (amoxicillin). If it’s not effective or the patient is resistant to them than use second option which is cephalosporin’s and aminoglycoside and so on. The last therapy for multi-resistant drug therapy is carbepenes (imipenem). Monotherapy of imipenem/clistatin for lower respiratory tract infections was safe and effective. Risk factors for multi resistant pneumonia are advance age, immune suppression, broad spectrum antibiotic exposure, increased severity of illness, methicilline
A 55yrs old patient name Mr. Nazir Ahmad was admitted to services hospital pulmonology ward 5th December 2017, with the complaint of severe breathing difficulty, fever, chest pain, cough and chills. He was a patient of hypertension too. He was also suffering from asthma but not taking any medicine for asthma. He was taking OTC medicine for cough and from last 15 days. The patient was taking cough syrup for cough and amoxicillin and antipyretic for fever. He was not taking medicine for asthma and hypertension.
History of Present Illness
He was complaining of fever, cough, breathing difficulties.
Past Medical History
- Fever from last 15 days and cough from last 1 month.
- He has asthma and hypertension.
Family History, Occupational History, Allergy
Nothing contributory
General Examination
- Height 5’5”
- Weight 68kg
• BP 100/70
• Pulse 110/min
• Temperature 990F
Diagnosis of Pneumonia
Chest X-ray Sputum Culture Test Oxygen saturation test AFB Test
Medication History
Amoxicillin, Antipyretics (Paracetamol, Disprine), Cough syrup.
The patient condition was improving day by day.
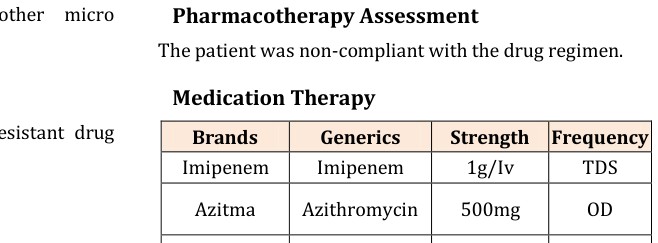
When the patient was admitted to the hospital he has accepted the prescribed drugs, including imipenem, azithromycin, panadol, and hydrocortisone and vent line. After 3 days imipenem stops and ceftriaxone started. All these agents have advantages and drawbacks. Routinely patient’s LFT and RFT are done. AFB test was conducted to confirm either its T.B or pneumonia. Patient was not compliant in the past that’s why tell him to follow to the regimen. Imipenem was the most potent drug for controlling Pneumonia symptoms, particularly the résistance induced through antibiotic. However imipenem is the most expensive drug so, is gradually withdrawn and another preparation then tried. For nasal congestion, and bronchospasm ventoline is recommended. Panadol (paracetamol) is added in the regimen for fever and patient fever was cured. Patient first strategy of therapy was not effective although his condition worsten then he was hospitalized.
Conclusion
In the present study a multi-drug resistant pneumonia patient condition addressed his regimen altered and compliance makes sure. A major difference in his condition was established. The patient condition was constantly improving. For improvement of the therapeutic strategies in such cases, further studies should be performed. To prove therapeutic strategies used in this case further studies are to be conducted, as present paper is single case study. Trial in a larger sample is required to generalize this effect.
References
-
National Institute of Health and Care Excellence (NICE) guidelines about pneumonia December 2014.
-
Grgurich PE, Hudcova J, Lei Y, Sarwar A, Craven DE (2012) Management and Prevention of Ventilator- associated Pneumonia Caused by Multidrug-resistant Pathogens. Expert Rev Resp Med 6(5): 533-555.
-
Sibila O, Rodrigo-Troyano A, Shindo Y, Aliberti S, Restrepo MI (2016) Multidrug-resistant pathogens in patients with pneumonia coming from the community 22(3): 219-226.
-
Gross AE, Schoonveld TCV, Olsen KM, Rupp ME, Bui TH, et al. (2014) Epidemiology and predictors of multidrug -resistant community acquired and Health Care associated Pneumonia. Antimicrob Agents Chemother 58(9): 5262-5268.
-
Multidrug Resistant Treatment Protocols in clinical pharmacy and therapeutics by Roger Walker and Cate whittles.
-
Salata RA, Gebhart RL, Palmer DL, Wade BH, Scheld WM, et al. (1985) Pneumonia treated with imipenem/ cilastatin. Am J Med 78(6A): 104-109.
-
Postma DF, van Werkhoven CH, van Elden LJR, Thijsen SFT, Hoepelman AIM, et al. (2015) Antibiotic treatment strategy for Community acquired pneumonia in adults. N Engl J Med 372: 1312-1323.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions