Epidemiology, Biology, Clinical Manifestation and Prevention of Influenza Virus Disease: A Review
Influenza means ‘flu’, caused by RNA viruses of Orthomyxoviridae family which is an infectious agent of birds and mammals. It causes mild to severe symptoms including chills, fever, sore throat, muscle pains, headache, coughing, fatigue but about 33% of the cases with influenza are asymptomatic. Since 1918, influenza virus has been one of the major causes of morbidity and mortality, especially among young children. Though the commonly circulating strain of the virus is not virulent enough to cause mortality, the ability of the virus genome to mutate at a very high rate may lead to the emergence of a highly virulent strain that may become the cause of the next pandemic. Apart from the influenza virus strain circulating in humans (H1N1 and H3N2), the avian influenza H5N1 H7 and H9 virus strains have also been reported to have caused human infections, H5N1 H7 and H9 have shown their ability to cross the species barrier from birds to humans and further replicate in humans. Influenza now spreads all over the world and it is also known as seasonal epidemics. This paper reviewed the epidemiology, biology, clinical manifestation and prevention of influenza virus.
Introduction
Influenza virus is involved in epidemic and pandemic diseases particularly respiratory system of both humans and animals. In 1918, influenza pandemically disturbed 50 million people and is still considered a great threat [1]. It belongs to family orthomyxoviridae and genus influenza virus A. Influenza virus is an envelope, negative sense, single stranded virus with segmented RNA that produces 11 proteins [2]. Waterfowls are considered to be the natural host for influenza A viruses [3]. Influenza virus adapts different ways to circumvent host immune system, either by down regulation of host immune system or by enhancing its replication process to counteract with host immune system. Virulence and pathogenicity of influenza virus greatly varies with its surface glycoproteins such as neuraminidase (NA) and hemagglutinin (HA) [4]. NAs are nine in number while haemagglutinin proteins (HA) are sixteen in number [5, 6, 7]. Other proteins of influenza A viruses include, nucleoprotein (NP), two types of matrix proteins i.e. M1 and M2, two non-structural proteins, i.e. NS1 and NS2 also called as nuclear export proteins (NEP), polymerase subunit (PA), PB1, PB1-F2 and PB2 [8]. Based on the antigenic differences in NP and M, influenza viruses can be classified into three genera: influenza virus A, influenza virus B and influenza virus C. Two others, still not well accepted genera include is a virus and thogotavirus [9]. Influenza A is mainly concerned with pandemic infections. It is reported that influenza viruses are pleomorphic in nature with mean diameter of 100– 150 nm and the shape varies from filamentous to spherical [10]. Influenza virus damages the respiratory epithelial cells that ultimately result in invasion of secondary bacterial infections. Moreover, it was reported that Haemagllutinin (HA) was involved in inhibition of LPS-induced interleukin 12 (IL12) and p70 at transcriptional level making environment suitable for secondary bacterial infections [11]. It has also been reported that influenza infections are fatal in patients having cardiac and pulmonary infection [12].
Types of Influenza
There are three different types of influenza virus – A, B, and C. The type A viruses are the most virulent human pathogens among the three influenza types and cause the most severe disease. The influenza A virus can be subdivided into different serotypes based on the antibody response to these viruses [12]. Two different proteins which are present on the surface of these viruses are called hemagglutinin (HA) and neuraminidase (NA). There are 16 different versions of HA and 9 different versions of NA [13]. Influenza B almost exclusively infects humans and is less common than influenza A [12]. The only other animals known to be susceptible to influenza B infection are the seal and the ferret [14]. This type of influenza mutates at a rate 2– 3 times slower than type A and consequently is less genetically diverse, with only one influenza B serotype [12, 15]. Influenza C virus infects humans, dogs and pigs, sometimes causing both severe illness and local epidemics [13]. However, influenza C is less common than the other types and usually only cause mild disease in children [16].
Structure of Influenza a Virion
Orthomyxovirus virions are usually close to being spherical, with diameter ranging from 100-200 nm (Figure 1). However, some laboratory strains may form extended threadlike structures, which sometimes exceed 1000 nm. The virions are relatively unstable in the en- vironment and influenza viruses are inactivated by heat, dryness, extremes of pH and detergents [17]. The outer lipid layer of influenza viruses originates from the plasma membranes of the host in which the virus was propagated [18]. Outside of the lipid envelope, there are about 500 projections/virions in the form of spikes. About 80% of these projections resemble rods which are composed of hemagglutinin. The remaining projections are in the shape of mushrooms and they are built from molecules of neuraminidase. The viral outer membrane also contains some copies of the small M2 protein that form ion channels in the virion particles. The matrix protein M1, which is the most abundant protein in virions, underlies the lipid layer and plays an important role in the attachment of the ribonucleoprotein (RNP). The RNP core is a complex structure composed mostly of the NP protein, which wraps eight different RNA segments of the influenza A genome. Additionally, RNPs contain about 50 copies per virion of RNA-dependent RNA polymerase, which in case of influenza A virus is a complex of three proteins: PB1, PB2 and PA [1].
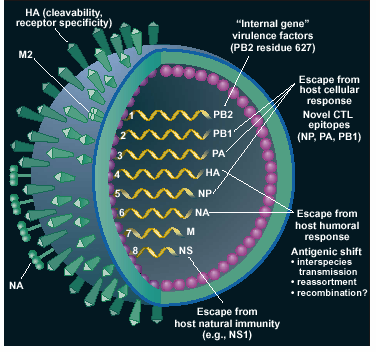
Source: Webster, 2001 Figure 1: Structure of influenza virus.
Epidemiology
As influenza is caused by a variety of species and strains of viruses, in any given year some strains can die out while others create epidemics with a potential to cause a pandemic. The incubation period of this virus is generally 1-4 days, with an average of 2 days [19]. The adults transmit influenza one day prior to onset of symptoms and up to 5 days after the symptoms begin. The children usually transmit it for 10 or more days [20]. The groups of people that are at a high risk for contracting influenza and influenza related complications include:
i. All individuals 50 years and older ii. Children 6–23 months of age iii. Women who are pregnant during influenza season iv. Residents of long term care facilities v. Children 6 months to 18 years of age and who are receiving aspirin therapy for extended period of time vi. Persons 6 months and older with any chronic illness [21]. Human H5N1 cases have been observed to increase towards the end of the year and during the early months of the subsequent year when the temperature and humidity is relatively lower and they occur in association with increases in H5N1 poultry outbreaks. A WHO review of 256 H5N1 cases found that the median age was 18 years (range 3 months-75 years), 89% of cases were more than 40 years old, the median duration from illness onset to hospitalization was 4 days, mortality was highest among cases aged 10–19 years, and the median duration from illness onset to death was 9 days (range 2–31 days) [22]. Investigations suggest that most human cases appear to have acquired H5N1 virus infection through avian-to- human transmission following direct or close contact with sick or dead poultry (e.g. slaughtering, culling, burying, preparing for food, de-feathering, etc.), well-appearing poultry (holding cock-fighting roosters, ducks or H5- vaccinated poultry) or wild birds (de-feathering dead wild swans) [23]. Risk factors for H5N1 disease identified in Vietnam and Thailand include directly touching sick or dead poultry or preparing them for consumption, having sick or dead poultry in or around the home, and being within 1 meter of sick or dead birds [24, 25]. In urban areas, where poultry raising is uncommon, a risk factor for H5N1 disease appears to be visiting a live poultry market [26]. This suggests that environmental factors could play a role in H5N1 virus transmission to humans. In up to a quarter of cases, a source of H5N1 virus exposure could not be identified [27]. Clusters of two or more epidemiologically linked H5N1 cases have been identified in several countries [28]. Approximately 25% of all H5N1 cases reported to date have occurred in clusters. Most clusters have involved two to three cases; the largest to date was eight cases (seven confirmed one probable) with seven deaths. While most cluster cases probably acquired H5N1 virus infection through common poultry exposures, limited, non-sustained human to human H5N1 virus transmission through close, prolonged, unprotected contact with a severely ill H5N1 patient has probably occurred or could not be excluded in some clusters [29, 30]. Probable, limited, human-to-human transmission in health care settings has been reported in health care workers and family members [29]. Nearly all H5N1 cluster cases have occurred among blood-related family members, suggesting a possible role of genetic susceptibility. The occurrence and frequency of clinically mild and asymptomatic H5N1 virus infection are unknown. A sero-prevalence study among 1525 Hong Kong poultry workers in 1997 found that 10% had H5N1 neutralizing antibodies [31]. Of the 11 pediatric H5N1 cases identified in 1997, seven had relatively mild disease, but four had severe or fatal illness. Limited data from case investigations and sero-surveys since 2003 suggest that clinically mild disease and asymptomatic H5N1 virus infection is uncommon. A small number of clinically mild H5N1 cases have been identified among children [30]. Sero-surveys among rural villagers in Cambodia, poultry workers in China and Nigeria, and health care workers in Vietnam and Thailand suggest that human H5N1 virus infection has been very rare to date. Therefore, the high proportion of fatal cases among reported H5N1 cases may be accurate, although further studies are needed on the spectrum of H5N1 virus infection. At admission, most H5N1 cases have presented with a history of high fever, cough, and shortness of breath, dyspnoea, and evidence of pneumonia on chest X-ray [23]. About one-third of cases have had diarrhoea. Common laboratory findings at hospitalization include leucopoenia, lymphopenia and mild to moderately decreased platelet counts [23]. Clinical complications include progression to respiratory failure, acute respiration distress syndrome (ARDS), multi-organ failure, sepsis, shock and reactive haemophagocytosis.
Clinical Manifestation of Human Influenza Infection
The disease is usually most severe in very young children (under 5 years of age) and the elderly. Many people are so ill that they are confined to bed for several days, with aches and pains throughout their bodies, which are worst in their backs and legs [32]. Symptoms of influenza may include:
i. Sudden onset of fever ii. Dry cough iii. Body aches, especially joints and throat iv. Coughing and sneezing v. Chills and rigor vi. Fatigue vii. Headache viii. Irritated watering eyes ix. Nasal congestion x. Reddened eyes, skin (especially face), mouth, throat and nose xi. Abdominal pain (in children with influenza B) [33]
Common symptoms of the flu such as fever, headaches, and fatigue come from the huge amounts of pro- inflammatory cytokines and chemokines (such as interferon or tumour necrosis factor) [32, 34] produced from influenza-infected cells. Of the symptoms listed above, the combinations of findings including fever, cough, sore throat and nasal congestion can improve diagnostic accuracy [35].
Laboratory Diagnosis of Influenza Virus
A number of tests help in the diagnosis of influenza. Specimens are preferably collected within the first 4 days of illness. Rapid influenza tests provide results within 30 min or less; viral culture provides results in 3-10 days. Routine serological testing for influenza requires paired acute and convalescent sera and does not provide results to help with clinical decision-making. Broadly the techniques are classified as direct and indirect diagnostic techniques. The Direct method involves detection of direct presence of viral particles, viral antigens, and viral genome through direct immune-flourescence, Enzyme linked immunosorbent assay, Antigen capture and staining of cells with monoclonal antibody [36, 37]. Other methods are indirect where the clinical samples may be inoculated in cell cultures, eggs, or animals for growth of the virus and its further typing. Hen’s eggs and cell lines are used for virus growth. Many continuous cell lines are being employed for influenza virus growth like MDCK, LLC-MK2 etc. [38]. The most common used cell line is MDCK. The presence of virus is detected by the cytopathic effect (CPE) like slow rounding and degeneration of cells. Further confirmation of influenza virus is done by haemagglutination test and haemagglutination-inhibition test which are used for routine diagnosis [39]. In recent years molecular techniques are being increasingly used for diagnostics. The advantage of these techniques is its sensitivity and quick turnaround time. Some molecular techniques for influenza diagnosis include reverse transcriptase polymerase chain reaction (RT-PCR), multiplex PCR, real time RT-PCR, nucleic acid based amplification (NASBA) and loop mediated isothermal amplification (LAMP) [40]. The most commonly used technique for rapid detection of influenza viruses is RT- PCR. It is extremely sensitive and rapid [41]. A reverse multiplex PCR is employed for typing and sub-typing of number of different influenza strains together. The appropriate combination of primer sets and optimizations of PCR conditions allow formation of multiplex PCR for detection of influenza A (H1N1 and H3N2) and B from clinical samples (Stockton 1998) [42]. The advent of molecular methods such as real time PCR has allowed improvement of detection methods currently used in laboratories, although not all of these methods include an internal positive control (IPC) to monitor for false negative results. A one-step reverse transcription real time PCR (RRT-PCR) with a minor groove binder (MGB) probe, for the detection of different subtypes of AIVs (against the HA and NA gene) has also been designed [43]. The PCR is performed and the corresponding graphs indicate the type, sub-types and amount of the viral strains without performing agarose gel analysis [44]. Most recent rapid, sensitive technique which is not found to be affected by other biological compounds in the clinical samples is called loop mediated isothermal amplification (LAMP) which is conducted under isothermal conditions of 60-65 ˚C by using enzyme called DNA polymerase. Thus, it is able to quantify the amount of DNA accurately without being affected by presence of other inhibitory substances [45, 46]. Thus more and more sensitive techniques must be explored for the development of efficient and effective strategies against influenza.
Procedure Influenza types Acceptable specimens Time for results Viral culture A and B NP (Naso Pharyngeal) swab, throat swab, nasal Immunofluorescence A and B NP swab, nasal wash, bronchial wash, nasal RT-PCR A and B NP swab, throat swab, nasal wash, bronchial wash, Enzyme Immuno Assay (EIA) A and B NP swab , throat swab, nasal wash, bronchial wash 2 hour Rapid detection tests (using kits) Serology A and B paired acute and convalescent serum samples 2 weeks or more A NP (Naso Pharyngeal) wash and aspirate Less than Source: Khanna et al., 2008 Table: Various techniques used for the laboratory diagnosis of the influenza virus.
Prevention and Treatment of Influenza
Influenza causes significant morbidity and mortality and is responsible for considerable medical expenditures. Antiviral therapy and vaccination are important strategies for the control of human/ avian influenza, but the efficacy of these modalities is limited by the timings of administration and shortage of supply. Healthcare workers currently must apply strict standards, contact and droplet precautions when dealing with suspected cases, and upgrade to airborne precautions when performing aerosol-generating procedures. Non- pharmacological measures such as early case isolation, household quarantine, school/workplace closure, good community hygiene and restrictions on travel are useful measures in controlling a pandemic [47, 48].
Chemotherapy
Rimantadine and amantadine are the two well known antivirals to prevent and treat influenza A. Amantadine and rimantadine are M2 inhibitors and block virus entry across the endosome and also interfere with virus release [49]. They are good prophylactic agents for influenza A and may be given as protective agents during an outbreak, especially to those at severe risk and key personnel. They may also be given at the time of vaccination for a few weeks, until the humoral response has time to develop. (There is some evidence that these drugs can help prevent more serious complications and reduce the duration of influenza A, if given early.) However, in the 2005-2006 influenza seasons, 92% of H3N2 strains examined had mutations that would confer resistance to these drugs as did 25% of the H1N1 strains tested. Similar problems were seen in 2006-2007 and so these drugs are not recommended until the percent resistance in the major circulating type drops. The resistance to amantadine and rimantadine is detected by sequencing the M2 gene which detects the point mutations responsible for imparting the resistance [50, 51, 52]. Two neuraminidase inhibitors (Zanamivir [Relenza] and Oseltamivir [Tamiflu]) have also been approved by the Food and Drug Administration (FDA) for prophylaxis as well as treatment [53, 54]. They are active against both influenza A and influenza B and can reduce the duration of uncomplicated influenza (by approximately 1day in about 70–90% of adults) if taken within two days of the onset of illness. Low-dose steroids may be considered in the treatment of refractory septic shock. Noninvasive positive pressure ventilation (NPPV) may play a limited supportive role for acute lung injury, but it is contra- indicated in critically ill patients with multi-organ failure and haemodynamic instability. Intravenous gammaglobulin should be used with caution for treatment of reactive haemophagocytosis due to its thrombogenic effects, whereas the role of etoposide needs evaluation with animal models [47, 48].
Vaccination
Influenza vaccine is often recommended for high-risk groups, such as children and the elderly. Influenza vaccines can be produced in several ways; the most common method is to grow the virus in fertilized eggs of hens [55]. A new vaccine is formulated annually with the types and strains of influenza predicted to be the major problems for that year (predictions are based on worldwide monitoring of influenza). The vaccine is multivalent (trivalent) and the current one, recommended by WHO, is to two strains of influenza A (one for H1N1 and one for H3N2) and one of influenza B. It has a short lived protective effect and is usually given in the fall so that protection is high in December/January – the usual peak months for flu in the northern hemisphere. In India, the poor population especially children living in slums and other over crowded areas should be targeted for vaccination in the start of November. About two weeks after vaccination, the antibodies that provide protection against virus infection develop in the body [56]. The types of influenza virus vaccine include;
- Inactivated virus vaccine: When the vaccine and the circulating strains are antigenically similar, inactivated vaccines prevent the illness among approximately 70–90 % of healthy adults with age less than 65 years (Demicheli et al 2000) [57]. Older persons and persons with chronic diseases might develop lower post vaccination antibody titers and can remain susceptible to influenza infection and other respiratory tract infection [58].
- Live attenuated influenza vaccine (LAIV): The virus can be grown in eggs until it loses virulence and the avirulent virus given as a live vaccine [59]. Attenuation is done by multiple changes in the various genome segments. Re-assortment is used to generate viruses which have six gene segments Emerging influenza virus: A global threat 479 from the attenuated virus and the HA and NA coding segments from the virus which is likely to be a problem in the up-coming influenza season [60, 61].
Conclusion
Influenza means ‘flu’, caused by RNA viruses of Orthomyxoviridae family which is an infectious agent of birds and mammals. It causes mild to severe symptoms including chills, fever, sore throat, muscle pains, headache, coughing, fatigue but about 33% of the cases with influenza are asymptomatic. Occasionally it leads to pneumonia in both healthy and immunosuppressive person. Influenza is transmitted through the air by coughing, sneezing or creating aerosols containing influenza. It can also be transmitted by direct contact with bird droppings or nasal secretions or through contact with contaminated surfaces. Influenza now spreads all over the world and it is also known as seasonal epidemics. Several reports depicted both emergence and pandemic potential of the virus in the perspective of earlier pandemic influenza viruses of 1918 (H1N1), 1957 (H2N2) and 1968 (H3N2) by comparison of the available genetic sequence data.
References
-
Boivin S, Cusack S, Ruigrok R, Hart DJ (2010) Influenza A Virus Polymerase: Structural Insights Into Replication And Host Adaptation Mechanisms. J Biol Chem 285(37): 28411-28417.
-
Hale B, Randall R, Ortı´n J, Jackson D (2008) The multifunctional NS1 protein of influenza A viruses. J gen Virol 89(10): 2359-2376.
-
Tumpey T, Basler C, Aguilar P, Zeng H, Solórzano A, et al. (2005) Characterization of the reconstructed 1918 Spanish influenza pandemic virus. Science 310(5745): 77-80.
-
Fouchier A, Munster V, Wallensten A, Bestebroer M, Herfst S, et al. (2005) Characterization of a novel influenza A virus hemagglutinin subtype (H16) obtained from black headed gulls. J Virol 79(5): 2814- 2822.
-
Glaser L, Stevens J, Zamarin D, Wilson I, García-Sastre A, et al. (2005) A single amino acid substitution in 1918 influenza virus hemagglutinin changes receptor binding specificity. J Virol 79(17): 11533-11536.
-
Yena H, Aldridgea J, Boona A, Ilyushinaa N, Salomona R, et al. (2009) Changes in H5N1 influenza virus hemagglutinin receptor binding domain affect systemic spread. PNAS 106(1): 286-291.
-
Ghedin E, Sengamalay N, Shumway M, Zaborsky J, Feldblyum T, et al. (2005) Large-scale sequencing of human influenza reveals the dynamic nature of viral genome evolution. Nature 437(7062): 1162-1166.
-
Potter W (1998) Chronicle of influenza pandemics In Textbook of Influenza. Black well Science. Oxford, UK.
-
Roberts, Compans (1998) Host cell dependence of viral morphology. Microbiology 95(10): 5746-5751.
-
Noone C, Lewis E, Frawely A, Newman R, Mahon B, et al. (2005) Novel mechanism of immunosuppression by influenza virus haemagglutinin: selective suppression of interleukin 12 p35 transcription in murine bone marrow-derived dendritic cells. J gen Virol 86: 1885-1890.
-
Schweiger B, Zadow I, Heckler R (2002) Antigenic drift and variability of influenza viruses. Medical Microbiology and Immunology 191(3-4): 133-138.
-
Hay AJ, Gregory V, Douglas AR, Lin YP (2001) The evolution of human influenza viruses. Philos Trans R Soc Lond B Biol Sci 356(1416): 1861-1870.
-
Matsuzaki Y, Sugawara K, Mizuta K, Tsuchiya E, Muraki Y, et al. (2002) Antigenic and genetic characterization of influenza C viruses which caused two outbreaks in Yamagata City, Japan, in 1996 and 1998. J Clin Microbiol 40(2): 422-429.
-
Osterhaus AD, Rimmelzwaan GF, Martina BE, Bestebroer TM, Fouchier RA (2000) Influenza B virus in seals. Science 288(5468): 1051-1053.
-
Nobusawa E, Sato K (2006) Comparison of the mutation rates of human influenza A and B viruses. J Virol 80(7): 3675-3678.
-
Matsuzaki Y, Katsushima N, Nagai Y, Shoji M, Itagaki T, et al. (2006) Clinical features of influenza C virus infection in children. J Infect Dis 193(9): 1229-1235.
-
Schulman JL, Palese P (1977) Virulence factors of influenza A viruses: WSN virus neuraminidase required for plaque production in MDBK cells. J Virol 24(1): 170-176.
-
Nayak DP, Hui EK, Barman S (2004) Assembly and budding of influenza virus. Virus Res 106(2): 147- 165.
-
Khanna M, Kumar P (2002) Influenza: A serious global threat. J Infect Dis Antimicro Agents 19: 25-39.
-
Elveback LR, Fox JP, Ackerman E, Langworthy A, Boyd M, et al. (1976) An influenza simulation model for immunization studies. Am J Epidemiology 103(2): 152-165.
-
Mathew TM (2006) Epidemiology of influenza A, B and C. Adv Med Veter Virol Immunol Epidemiol 6: 24.
-
World Health Organization (2007) Recommendations and laboratory procedures for detection of avian influenza A (H5N1) virus in specimens from suspected human cases.
-
World Health Organization (2008) Cumulative number of confirmed human cases of avian influenza A(H5N1) reported to WHO.
-
Areechokchai D, Jiraphongsa C, Laosiritaworn Y, Hanshaoworakul W, O’Reilly M, et al. (2006) Investigation of avian influenza (H5N1) outbreak in humans-Thailand, 2004. MMWR 55(1): 3-6.
-
Dinh PN, Long HT, Tien NT, Hien NT, Mai le TQ, et al. (2006) Risk factors for human infection with avian influenza A H5N1, Vietnam, 2004. Emerg Infect Dis 12(12): 1841-1847.
-
Yu H, Feng Z, Zhang X, Xiang N, Huai Y, et al. (2007) Human influenza A (H5N1) cases, urban areas of people’s Republic of China, 2005-2006. Emerg Infect Dis 13(7): 1061-1064.
-
Sedyaningsih ER, Isfandari S, Setiawaty V, Rifati L, Harun S, et al. (2007) Epidemiology of cases of H5N1 virus infection in Indonesia, July 2005-June 2006. J Infect Dis 196(4): 522-527.
-
Olsen SJ, Ungchusak K, Sovann L, Uyeki TM, Dowell SF, et al. (2005) Family clustering of avian influenza A (H5N1). Emerg Infect Dis 11(11): 1799-1801.
-
Ungchusak K, Auewarakul P, Dowell SF, Kitphati R, Auwanit W, et al. (2005) Probable person-to-person transmission of avian influenza A (H5N1). N Engl J Med 352(4): 333-340.
-
Kandun IN, Wibisono H, Sedyaningsih ER, Yusharmen, Hadisoedarsuno W, et al. (2006) Three Indonesian clusters of H5N1 virus infection in 2005. N Engl J Med 355: 2186-2194.
-
Bridges CB, Lim W, Hu-Primmer J, Sims L, Fukuda K, et al. (2002) Risk of influenza A (H5N1) infection among poultry workers, Hong Kong, 1997-1998. J Infect Dis 185(8): 1005-1010.
-
Eccles R (2005) Understanding the symptoms of the common cold and influenza. Lancet Infect Dis 5(11): 718-725.
-
Kerr AA, McQuillin J, Downham MA, Gardner PS (1975) Gastric flu influenza B causing abdominal symptons in children. Lancet 1(7902): 291-295.
-
Schmitz N, Kurrer M, Bachmann MF, Kopf M (2005) Interleukin- 1 is responsible for acute lung immunopathology but increases survival of respiratory influenza virus infection. J Virol 79(10): 6441-6448.
-
Call SA, Vollenweider MA, Hornung CA, Simel DL, McKinney WP (2005) Does this patient have influenza?. JAMA 293(8): 987-997.
-
Orskov I, Orskov F (1990) Serologic classification of fimbriae. Curr Top Microbiol Immunol 151: 71-90.
-
Brumback BG, Wade CD (1996) Simultaneous rapid culture for four respiratory viruses in the same cell monolayer using a differential multicolored fluorescent confirmatory stain. J Clin Microbiol 34(4): 798-801.
-
Davies FG, Casals J, Jesset DM, Ochieng P (1978) The serological relationships of Nairobi sheep disease virus. J Comp Pathol 88(4): 519-523.
-
Hirst GK (1941) Agglutination of red cells by allantoic fluid of chick embryos infected with influenza virus. Science 94(2427): 22-23.
-
Khanna M, Srivastava V (2006) Clinical laboratory diagnosis of influenza. Adv Med Veter Virol Immunol Epidemiol 6: 138.
-
Wright KE, Wilson GA, Novosad D, Dimock C, Tan D, et al. (1995) Typing and subtyping of influenza viruses in clinical samples by PCR. J Clin Microbiol 33(5): 1180-114.
-
Stockton J, Ellis JS, Saville M, Clewley JP, Zambon MC (1998) Multiplex PCR for typing and subtyping influenza and respiratory syncytial viruses. J Clin Microbiol 36(10): 2990-2995.
-
Lee CW, Suarez DL (2004) Application of real-time RT-PCR for the quantitation and competitive replication study of H5 and H7 subtype avian influenza virus. J Virol Methods 119(2): 151-158.
-
Di Trani L, Bedini B, Donatelli I, Campitelli L, Chiappini B, et al. (2006) A sensitive one-step real- time PCR for detection of avian influenza viruses using a MGB probe and an internal positive control. BMC Infect Dis 6: 87.
-
Poon LL, Leung CS, Chan KH, Lee JH, Yuen KY, et al. (2005) Detection of human influenza A viruses by loop-mediated isothermal amplification. J Clin Microbiol 43(1): 427-430.
-
Kaneko H, Kawana T, Fukushima E, Suzutani T (2007) Tolerance of loop-mediated isothermal amplification to a culture medium and biological substances. J Biochem Biophys Methods 70(3): 499-501.
-
Hui DS (2008) Influenza A/H5N1 infection: Other treatment options and issues. Respirology 1: S22- S26.
-
Tambyah PA (2008) Update on influenza vaccines. Respirology 13: S41-S43.
-
Wang C, Takeuchi K, Pinto LH, Lamb RA (1993) Ion channel activity of influenza A virus M2 protein: characterization of the amantadine block. J Virol 67(9): 5585-5594.
-
Belshe RB, Smith HM, Hall CB, Betts R, Hay AJ (1988) Genetic basis of resistance to rimantadine emerging during treatment of influenza virus infection. J Virol 62(5): 1508-1512.
-
Hayden FG, Hay AJ (1992) Emergence and transmission of influenza A viruses resistant to amantadine and rimantadine. Curr Top Microbiol Immunol 176: 119-130.
-
Abed Y, Goyette N, Boivin G (2005) Generation and characterization of recombinant influenza A (H1N1) viruses harboring amantadine resistance mutations. Antimicrob Agents Chemother 49(2): 556-559.
-
Gubareva LV, McCullers JA, Bethell RC, Webster RG (1998) Characterization of influenza A/Hong Kong/156/97 (H5N1) virus in a mouse model and protective effect of zanamivir on H5N1 infection in mice. J Infect Dis 178(6): 1592-1596.
-
Monto AS, Robinson DP, Herlocher ML, Hinson JM Jr, Elliott MJ, et al. (1999) Zanamivir in the prevention of influenza among healthy adults: a randomized controlled trial. JAMA 282(1): 31-35.
-
Osterholm MT (2005) Preparing for the next pandemic. N Engl J Med 352(18): 1839-1842.
-
Dunnil P (2006) A DNA flu vaccine in practice. Nat Biotechnol 24(2): 139.
-
Demicheli V, Jefferson T, Rivet D, Deeks J (2000) Prevention and early treatment of influenza in healthy adults. Vaccine 18(11-12): 957-1030.
-
McElhaney JE, Beattie BL, Devine R, Grynoch R, Toth EL, et al. (1990) Age related decline in interleukin 2 production in response to influenza vaccine. J Am Geriatr Soc 38(6): 652-658.
-
Hilleman MR (2002) Realities and enigmas of human viral influenza: pathogenesis, epidemiology and control. Vaccine 20(25-26): 3068-3087.
-
Jin H, Lu B, Zhou H, Ma C, Zhao J, et al. (2003) Multiple amino acid residues confer temperature sensitivity to influenza virus vaccine strains (Flu Mist) derived from cold adapted A/Ann Arbor/ 6/60. Virology 306(1): 18-24.
-
Hoffmann E, Mahmood K, Chen Z, Yang CF, Spaete J, et al. (2005) Multiple gene segments control the temperature sensitivity and attenuation phenotypes of ca B/Ann Arbor/ 1/66. J Virol 79(17): 11014- 11021.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions