Hepatitis C Virus Pathophysiology and Diagnosis
Hepatitis C virus (HCV) is spherical enveloped RNA virus and belongs to Flaviviridae family , Parenteral exposure to the HCV is the most efficient means of transmission . Often Hepatitis C is diagnosed accidentally so, HCV diagnostic tests should be performed in all patients presenting with increased aminotransferase levels. The number of patients actually HCV RNA positive is estimated to be around 80 to 90% of all HCV-antibody positive persons the Genotype 4 is responsible for >90% of cases ,approximately 3% of the world’s population (roughly 170-200 million people) infected with hepatitis C virus with considerable regional variations.
Introduction
Hepatitis C virus (HCV) is the principal cause of death from liver disease and the leading indication for liver transplantation [1]. Hepatitis C virus (HCV) infection is a major health problem around the globe, with more than 200 million people infected worldwide [2]. Genotype 4 is responsible for >90% of cases. The distribution of this genotype (specifically subtype 4a) is thought to be due to the mass treatment programs for schistosomiasis for decades until the 1980s when oral treatment became available [3]. Complications of hepatitis C occur mostly in patients who develope cirrhosis. The risk for decompensation is estimated to be close to 5% per year in cirrhotics [4]. Once decompensation has developed the 5- year survival rate is roughly 50% [5]. Hepatocellular carcinoma (HCC) also develops solely in patients with cirrhosis (in contrast to chronic hepatitis B) [6].
Hepatitis C Pathophysiology
Viral Structure
Taxonomy and Genotypes: The hepatitis C virus (HCV) belongs to Hepacivirus genus of the Flaviviridae family with six major HCV genotypes with a large number of subtypes within each genotype [7].
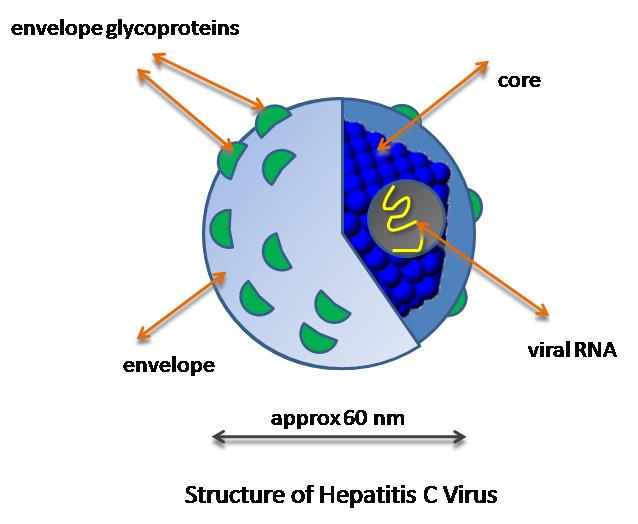
The high replication rate of the virus together with the error-prone RNA polymerase of HCV led to the large inter-patient genetic diversity of HCV strains. Moreover, the extent of viral diversification of HCV strains within a single HCV-positive individual increase significantly over time resulting in the development of quasispecies [8]. Viral Structure: HCV virions have a spherical envelope containing tetramers (or dimer of heterodimers) of the HCV E1 and E2 glycoproteins (Figure 1). Inside the virions a spherical structure has been observed representing the nucleocapsid (core) that harbours the viral genome [9].
Epidemiology
Prevalence and Incidence
The World Health Organization estimates that 130– 150 million individuals worldwide are chronically infected (WHO, 2010). The number of patients actually HCV RNA positive is estimated to be around 80 to 90% of all HCV-antibody positive persons. Certain groups are preferentially affected: the highest risk factor in most instances is injection drug use, but patients undergoing hemodialysis and persons who received blood transfusions before 1991 are at risk also [6]. It is difficult to determine the number of new HCV infections, as most acute cases will not be noticed clinically. Fewer than 25% of acute cases of hepatitis C are clinically apparent [10].
Because chronic liver disease may develop many years after infection, the past incidence is a major determinant of the future burden of HCV-associated complications [11]. In Egypt, as there has been an ongoing high risk for decades, the high magnitude of the current burden of HCV-related chronic disease is predicted to continue into the future [12]. Global mortality due to hepatitis C infection is approximately 700,000 individuals per year [13].
Transmission
- Parenteral exposure to the HCV is the most efficient means of transmission. The following possible routes of infection have been identified in anti-HCV-positive blood donors (in descending order of transmission risk):
- Injection drug use
- Blood transfusion
- Sex with an intravenous drug user
- Having been in jail more than three days
- Religious scarification
- Having been struck or cut with a bloody object
- Pierced ears or body parts
- Immunoglobulin injection Very often in patients with newly diagnosed HCV infection no clear risk factor can be identified [6].
Natural History
Acute Hepatitis
HCV incubation period (range 1-26 weeks) after exposure. However, the majority of newly infected patients will be asymptomatic and clinically non-apparent or mild course. Symptoms include malaise, nausea, and right upper quadrant pain. Loss of HCV RNA, which indicates a hepatitis C cure, occurs in fewer than 20% of patients [14].
Chronic Hepatitis
Hepatitis C is considered to be chronic after six months. About 75% of patients with acute hepatitis C will progress to chronic infection. Most of them will have persistently elevated liver enzymes in follow-up. Most patients with chronic infection are asymptomatic or have only mild nonspecific symptoms as long as cirrhosis is not present [15]. The most frequent complaint is fatigue. Less common manifestations are nausea, weakness, myalgia, arthralgia, and weight loss [16]. Aminotransferase levels can vary considerably over the natural history of chronic hepatitis C [6].
The risk of developing cirrhosis is estimated to be around 10 to 20% within 20 years, with some studies showing estimates of up to 50% [17]. About 30% of patients will not develop cirrhosis for at least 50 years [4].
Cirrhosis and Hepatic Decompensation
Complications of hepatitis C occur mostly in patients who develope cirrhosis. The risk for decompensation is estimated to be close to 5% per year in cirrhotics [4]. Once decompensation has developed the 5-year survival rate is roughly 50% [5]. Liver transplantation is then the only effective therapy. Hepatocellular carcinoma (HCC) also develops solely in patients with cirrhosis (in contrast to chronic hepatitis B) [6].
Extrahepatic manifestations
About 30 to 40% of patients with chronic hepatitis C develop an extrahepatic manifestation of HCV include essential mixed cryoglobulinemia, lymphoma (Figure 2).
Autoimmune thyroiditis, membranoproliferative glomerulonephritis Dermatologic disease, porphyria cutanea tarda, lichen planus, Diabetes mellitus [18].
![Figure 2: Extrahepatic manifestations of hepatitis C virus infection by organ. Information adapted from [19].](/fulltextimages/3512/fig_2.png)
Disease Progression
Several factors affect Chronic HCV progression as follows:- More rapid progression is seen in males older than 40- 55 [20]. Slower progression has been noted in African- Americans [21]. Human leukocyte antigen (HLA) expression may influence the cellular immune response specific to HCV [22]. Alcohol increase HCV replication, enhance the progression of chronic HCV, and accelerate liver injury [23]. Liver damage is usually worse and progression faster in patients with dual HBV/HCV infections and co-infection with several genotypes may have a worse outcome as compared to mono-infection [6].
Diagnosis
Often Hepatitis C is diagnosed accidentally so, HCV diagnostics should be performed in all patients presenting with increased aminotransferase levels, with a history of enhanced risk of HCV transmission and with chronic liver disease of unclear etiology [24].
Serologic Assays
The 3rd generation enzyme-linked immunoassays (EIAs allow the detection of anti-HCV antibodies approximately four to six weeks after infection with a sensitivity of more than 99% [25]. One quantitative HCV core antigen assay (Architect HCV Ag, Abbott Diagnostics) has been approved so far. This assay comprises 5 different antibodies, is highly specific (99.8%) and shows equivalent sensitivity for determination of chronic hepatitis C as HCV RNA measurement [26]. but, the sensitivity of the core antigen assay is lower in comparison to highly sensitive HCV RNA assays [24].
Nucleic Acid Testing for HCV
1. Qualitative HCV RNA tests include the qualitative real time (RT)-PCR, [27]. 2. HCV RNA quantification can be achieved either by target amplification techniques (competitive and real- time PCR) or by signal amplification techniques (branched DNA (bDNA) assay) [24].
HCV Genotyping
HCV is heterogeneous with enormous genomic sequence variability due to its rapid replication cycle producing 1012 virions a day and low fidelity of the HCV RNA polymerase. Six genotypes (1-6), multiple subtypes (a, b, c…) and most recently a seventh HCV genotype have been characterized. Within one subtype, numerous quasispecies exist and may emerge during treatment with specific antivirals. Because the currently recommended treatment durations and ribavirin doses depend on the HCV genotype, HCV genotyping is mandatory in every patient considering antiviral therapy (Figure 3). Both direct sequence analysis and reverse hybridisation technology allow HCV genotyping [28]. However, in Egypt where genotype 4 is the predominant type, genotype pretesting may be ignored to save fund [29].
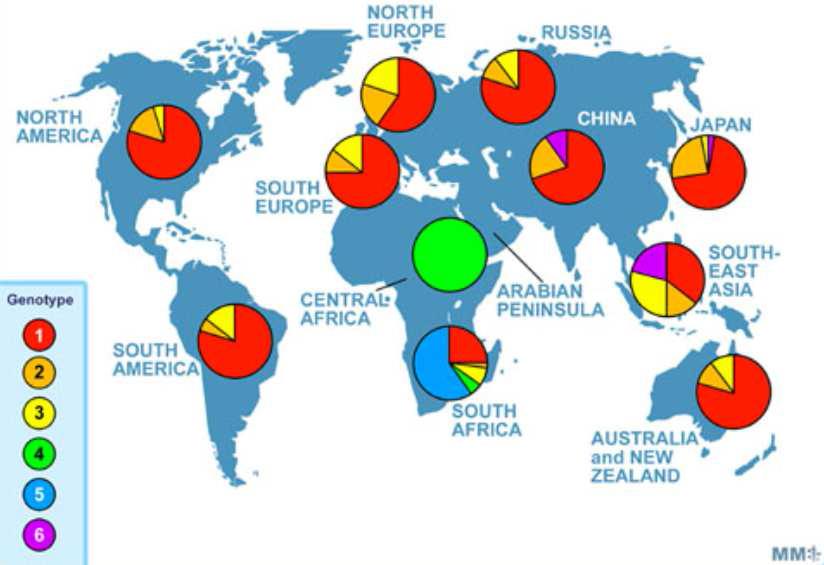
Global distribution of HCV genotypes
Source: WHO Hepatitis C Fact Sheet no. 164 (July 2012): http://www.who.int/mediacentre/factsheets/fs164/en/i ndex.html. Source image: http://www.gregoryledet.com/?p=60.
Interpretation of HCV Assays
Interpretation of HCV according to Anti-HCV antibodies and HCV, RNA detection (Table 1).
| HCV RNA | Status | |
|---|---|---|
| + | + | 1 Depending on clinical status: acute or chronic HCV infection |
| + | - | 1 Resolution of HCV—acute HCV infection during a period of low-level viremia |
| - | + | 1 Early acute HCV infection1 Chronic HCV in a setting of immunosuppressed + status1 False-positive HCV RNA test |
| - | - | 1 No HCV infection |
Table 1: Anti-HCV antibodies and HCV, RNA detection.
Diagnosing Acute Hepatitis C
When acute hepatitis C is suspected, the presence of both anti-HCV antibodies and HCV RNA should be tested.
For HCV RNA detection, When HCV RNA is detected in seronegative patients, acute hepatitis C is very likely. When patients are positive for both anti-HCV antibodies and HCV RNA, it may be difficult to discriminate between acute and acutely exacerbated chronic hepatitis C. Anti- HCV IgM detection will not suffice because its presence is common in both situations [27].
Diagnosing Chronic Hepatitis C
When chronic hepatitis C is suspected, screening for HCV antibodies by 2nd or 3rd generation EIAs is adequate because their sensitivity is >99%. When anti-HCV antibodies are detected, the presence of HCV RNA has to be determined in order to discriminate between chronic hepatitis C and resolved HCV infection [27].
References
-
Kim WR (2002) The burden of hepatitis C in the United States. Hepatology 36 (5 Suppl 1): S30-S34.
-
Waheed Y (2015) Ledipasvir and sofosbuvir: Interferon free therapy for hepatitis C virus genotype 1 infection. World J Virol 4(1): 33-35.
-
Tanaka Y, Agha S, Saudy N, Kurbanov F, Orito E, et al. (2004) Exponential spread of hepatitis C virus genotype 4a in Egypt. J Mol Evol 58(2): 191-195.
-
Poynard T, Bedossa P, Opolon P (1997) Natural history of liver fibrosis progression in patients with chronic hepatitis C. The OBSVIRC, METAVIR, CLINIVIR, and DOSVIRC groups. Lancet 349(9055): 825-832.
-
Planas R, Balleste B, Alvarez MA, Rivera M, Montoliu S, et al. (2004) Natural history of decompensated hepatitis C virus-related cirrhosis. A study of 200 patients. J Hepatol 40(5): 823-830.
-
Wasmuth JC (2011) Epidemiology, transmission and natural history of hepatitis C. _In:_ Mauss S, Berg T, Rockstroh J, Sarrazin C, Wedemeyer H (Eds.), Short guide to hepatitis C. Düsseldorf: Flying Publisher, pp: 13-19.
-
Simmonds P, Bukh J, Combet C, Deleage G, Enomoto N, et al. (2005) Consensus proposals for a unified system of nomenclature of hepatitis C virus genotypes. Hepatology 42(4): 962-973.
-
Bukh J, Miller RH, Purcell RH (1995) Biology and genetic heterogeneity of hepatitis C virus. Clin Exp Rheumatol 13(13): S3-S7.
-
Wakita T, Pietschmann T, Kato T, Date T, Miyamoto M, et al. (2005) Production of infectious hepatitis C virus in tissue culture from a cloned viral genome. Nat Med 11(7): 791-796.
-
Wasley A, Grytdal S, Gallagher K (2008) Surveillance for acute viral hepatitis-United States, 2006. MMWR Surveill Summ 57: 1-28.
-
Perz JF, Alter MJ (2006) The coming wave of HCV- related liver disease: dilemmas and challenges. J Hepatol 44(3): 441-443.
-
Alter MJ (2007) Epidemiology of hepatitis C virus infection. World J Gastroenterol 13(17): 2436-2441.
-
GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013.
-
Hoofnagle JH (1997) Hepatitis C: the clinical spectrum
-
Merican I, Sherlock S, McIntyre N, Dusheiko GM (1993) Clinical, biochemical and histological features in 102 patients with chronic hepatitis C virus infection. Q J Med 86(2):119-125.
-
Sangiovanni A, Prati GM, Fasani P, Ronchi G, Romeo R, et al. (2006) The natural history of compensated cirrhosis due to hepatitis C virus: A 17-year cohort study of 214 patients. Hepatology 43(6): 1303-1310.
-
Zignego AL, Craxi A (2008) Extrahepatic manifestations of hepatitis C virus infection. Clin Liver Dis 12(3): 611-636.
-
Negro F, Forton D, Craxì A, Sulkowski MS, Feld JJ, et al. (2015) Extrahepatic morbidity and mortality of chronic hepatitis C. Gastroenterology 149(6): 1345- 1360.
-
Svirtlih N, Jevtovic D, Simonovic J, Delic D, Dokic L, et al. (2007) Older age at the time of liver biopsy is the important risk factor for advanced fibrosis in patients with chronic hepatitis. Hepatogastroenterology 54(80): 2324-2327.
-
Sterling RK, Stravitz RT, Luketic VA, Sanyal AJ, Contos MJ, et al. (2004) A comparison of the spectrum of chronic hepatitis C virus between Caucasians and African Americans. Clin Gastroenterol Hepatol 2(6): 469-473.
-
Hraber P, Kuiken C, Yusim K (2007) Evidence for human leukocyte antigen heterozygote advantage against hepatitis C virus infection. Hepatology 46(6): 1713-1721.
-
Gitto S, Micco L, Conti F, Andreone P, Bernardi M (2009) Alcohol and viral hepatitis: A mini-review. Dig Liver Dis 41(1): 67-70.
-
Lange C and Sarrazin C (2011). Diagnostic tests in acute and chronic hepatitis C. Short guide to hepatitis C. Flying publisher, pp: 20-32.
-
Colin C, Lanoir D, Touzet S, Meyaud-Kraemer L, Bailly F, et al. (2001).Sensitivity and specificity of third- generation hepatitis C virus antibody detection assays: an analysis of the literature. J Viral Hepat 8(2): 87-95. of disease. Hepatology 26(3 Suppl 1): 15S-20S.
-
Lauer GM and Walker BD (2001) Hepatitis C virus infection. N Engl J Med 345(1): 41-52. K, et al. (2009) A new sensitive and automated chemiluminescent microparticle immunoassay for quantitative determination of hepatitis C virus core antigen. J Virol Methods 157(1): 8-14.
-
Nolte FS, Fried MW, Shiffman ML, Ferreira-Gonzalez A, Garrett CT, et al. (2001) Prospective multicenter clinical evaluation of AMPLICOR and COBAS AMPLICOR hepatitis C virus tests. J Clin Microbiol 39(11): 4005-4012.
-
Bowden DS, Berzsenyi MD (2006) Chronic hepatitis C virus infection: genotyping and its clinical role. Future Microbiol 1(1): 103-112.
-
Zekri AR, Bahnassy AA, Ramadan AS, El-Bassuoni M, Badran A, et al. (2001) Hepatitis C virus genotyping versus serotyping in Egyptian patients. Infection 29(1): 24-26.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions