Prevalence Along with Diagnostic Modalities and Treatment of Female Infertility Due to Female Genital Disorders
Infertility is a communal pathological ailment now-a-days worldwide and approximately females are mostly suffering from this condition. In previous studies, out of 2.4 million married couples have females in between the ages from 15-44 year; 1.0 million couples were suffering from primary infertility and 1.4 million couples had secondary infertility. The infertility causes are ovulatory factors, dietary factors, psychological factors, abnormal endocrine functions, fallopian tube disorders etc. PCOS, PIDs, endometriosis. The ultrasonography is the most powerful tool for diagnosis. The treatment involves medical, surgical and assisted reproduction. Medical treatment includes clomiphene, metformin, iron & folic acid supplements along with oralcontraceptives. Surgical treatment is operative laparoscopy and assisted reproduction is achieved by IVF, GIFT & IUI etc. It is concluded from the study that the percentage prevalence of female infertility among ages was higher in age group (25-34) years (76%) and it was mostly secondary infertility (54%). The main pathological factor of female infertility in Sialkot city was PCOS, which was 52% of evaluated patients. Commonly used diagnostic tools were ultrasonography with prevalence of 100% and endocrine tests (72%). In prescription trend, anti-obesity drugs, anti-oestrogen drugs and oral-contraceptives were commonly prescribed and other treatment interventions were also seen in few patients.
Introduction
Infertility is a medical condition in which a couple having consistent, unprotected mating within the time period of one or additional years but is unable to conceive [1]. Infertility in women is occurs due to female genital disorders i.e. PCOS, PID and endometriosis are discussed in this literature. Furthermore, medical histories and objective finding help to reveal the causes of female infertility. Previous studies have concluded that 37% of infertility factors are associated with female partner [2]. Globally, round about 72.4 million women (20-44yrs of age) have fertility problems from which approximately 40.5 million are pursuing infertility medical care and 32.6 million are not seeking infertility medical care [3]. PCOS is one of the major causes of ovulation disorders, premature ovarian failure (POF) & reduced ovarian reserve may occur. Chlamydial infections cause fallopian tubes (acute salpingitis) obstruction that leads to the failure of an ovum to pass through it and unite with the sperms resulting in infertility [4]. Erectile dysfunction, ejaculation problems, concentrated semen, atrophies after invasive procedures androgens and thyroxin imbalanced or vasectomy can lead to infertility or subfertility [5]. In endometriosis, pain during defecation and urination, ectopic growth of uterine tissue, dysmenorrhoea, dyspareunia & pelvic pain can occur [6]. Symptoms of estrogen deficiency develop in many, but not all, patients. These symptoms include vasomotor symptoms (hot flashes and night sweats), sleep disturbance, and dyspareunia related to vaginal dryness. However, not all patients have profound estrogen deficiency, and a vaginal examination often shows effects suggesting normal estrogen levels [7]. Semen analysis is done to analyse the sperm count, sperm shape, sperm motility as well as sperm dysfunction [8]. The ultrasonography (USG) and sonohysteroscopy is used to examine the pelvic cavity and organs located in it [9]. Gonadotropins are the hormones which induce ovulation [10].
Methodology
Study Design and Sample Size
The study was a cross sectional prevalence study to assess the female infertility and its associated genital disorders, types, diagnostic tool and possible treatment plans. The study was done by taking samples of 50 patients from specified age groups at different times and did this work from different hospitals in different areas of Sialkot and their regions i.e. civil hospital, Memorial Christian hospital, Islam Central hospital, Khalida Memorial hospital and others.
Method of Data Collection
Firstly, a formal permission was taken from the respective authors to use and translate the assessment measures. After that, the informed consent was taken from the concerned authorities of various academic institutes. The nature of research was briefed to each of the participant and it was assured that the information obtained from them will be held confidential and would not be used for any other work except for this research. The participants were given the freedom to withdraw from the research at any moment. Patients of different age groups were included in the study and were divided into four corresponding sub groups of age from puberty to menopause i.e. 15-24 years, 25-34 years, 35-45years & >45 years. Participants were asked to comment on the relevance of the questions that were present in the questionnaire. The average time required to complete the questions (by self-report) was 10 minutes (Range 5-20 minutes). Data collection was done from archived data sheets and worksheets.
Patient was asked to fill the consent form attached to the research work. Patients were asked to bring the prescription along with their recent lab reports. Patients were asked to provide detailed medication history including OTC medication. The data collected from the participants on the questionnaire form that was designed by the support of supervisors. The pharmacist treated the patients by asking them different questions about their disease, family history and other relevant data.
Inclusion Criteria
Patients having consistent, unprotected mating within the time period of one or additional years but is unable to conceive were included in study. Patient who has signed the informed consent form, patients from puberty to menopause and married women only were included.
Data Analysis
The data was presented in the form of frequency and percentages. It was interpreted and analyzed from worksheets and excel sheets and the graphs of corresponding data collection made from various hospitals were plotted.
Results
Prevalence, Type of Infertility and Pathological Factors of Infertility in Females Among Various Age Groups
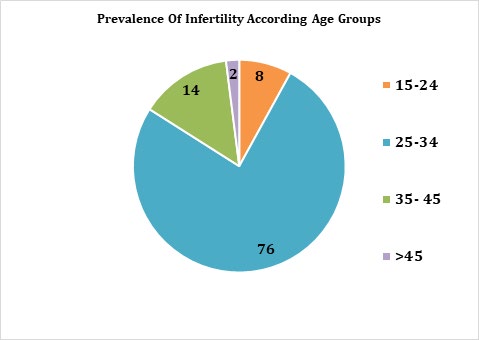
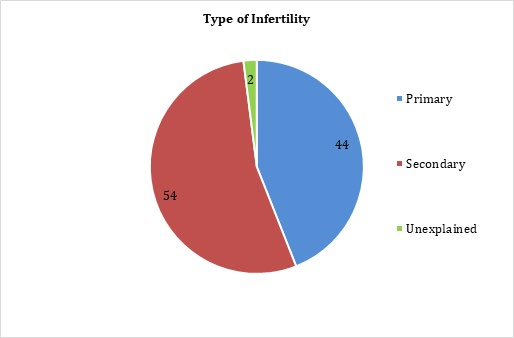
Female patients were divided into 4 categories by age: 15-24 years, 25-34 years, 35-45years and >45 years. Graph clearly demonstrated that the age between 15- 24 years, 4 cases had infertility, while 25-34 years of age group represents peak age group of females suffering from infertility (38 cases), within the age group of 35-45 years, infertility cases (7 cases) had seen. There was only one case of infertility seen in females of >45 years of age because at that age, female is near the menopause. Infertility is closely related to the reproductive age of a female and this age starts from puberty and end at menopause. In Pakistan, usual marriage ages are between 25-35years and at this age infertility is meant to be occurred related to various pathological factors and reproductive cycle irregularities. The hormonal changes in body take place and the level of female reproductive hormones decreases with ages i.e. oestrogen secretion releases at peak in between 15-40 years. Out of 50 participants, types of infertilities were checked i.e. primary infertility and secondary infertility. As the graph demonstrated, 44% (22 cases) were seen to have primary infertility and 54% (27 cases) were seen to have secondary infertility. Only single case of unexplained infertility was seen during the research process in Sialkot.
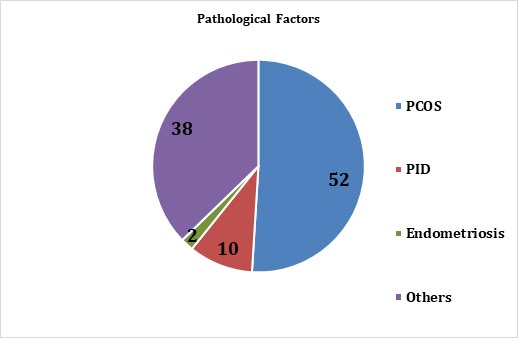
Total 52% (26 cases) females were suffering from PCOS i.e. anovulatory disorder, 10% (5 cases) females had PID i.e. fallopian tube disorder, no patient of endometriosis was seen during study 0% (no case) and 38% (19 cases) females had other that above mentioned pathological factors i.e. cervical fibroids, premature ovarian failure, decreased ovarian reserve, endocrine disorders, male factors, psychological disorders etc. PCOS were most common cause of female infertility and is associated with certain symptoms like hirsuitism, obesity, acne and ovarian cysts seen via ultrasonography. PID was associated with tubal blockade and operative laparoscopy was performed to diagnose and treat such pathological condition.
| Parameters | Frequency | Percentage | |
|---|---|---|---|
| Age Groups | 15-24 | 4 | 8 |
| Age Groups | 25-34 | 38 | 76 |
| Age Groups | 35-45 | 7 | 14 |
| Age Groups | >45 | 1 | 2 |
| Type of Infertility | Primary | 22 | 44 |
| Type of Infertility | Secondary | 27 | 54 |
| Type of Infertility | Unexplained | 1 | 2 |
| Type of Infertility | PCOS | 26 | 52 |
| Pathological Factor | PID | 5 | 10 |
| Pathological Factor | Endometriosis | 1 | 2 |
| Pathological Factor | Others | 19 | 38 |
Table 1: Prevalence, type of infertility and pathological factors of infertility in females among various age groups.
Diagnostic Tools for Measuring Infertility in Females
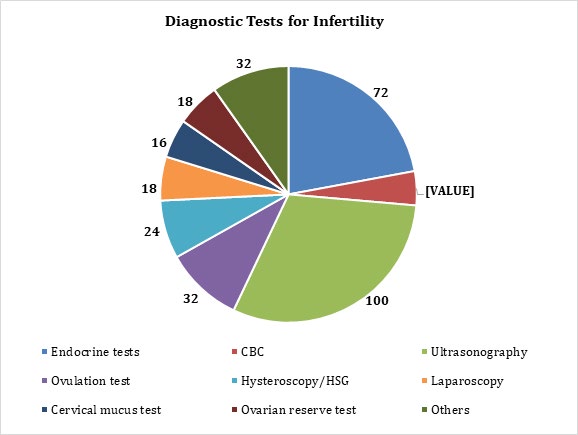
Overall 72% endocrine tests, 14% CBC, 100% ultrasonography, 32% ovulation test, 24% hysteroscopy/ HSG, 36% laparoscopy, 16% cervical mucus test, 18% ovarian reserve test & 16% other tests i.e. semen analysis, BP, blood glucose test etc were done.
| Diagnostic Tools | Frequency | Percentage |
|---|---|---|
| Endocrine Tests | 36 | 72 |
| CBC | 7 | 14 |
| Ultrasonography | 50 | 100 |
| Ovulation Test | 16 | 32 |
| Hysteroscopy/HSG | 12 | 24 |
| Laparoscopy | 9 | 18 |
| Cervical Mucus Test | 8 | 16 |
| Ovarian Reserve Test | 9 | 18 |
| Others | 16 | 32 |
Table 2: Diagnostic tools for measuring infertility in females.
Treatment Trends for Management of Infertility in Females
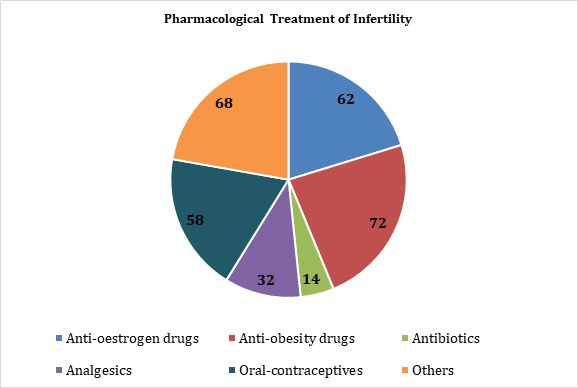
The prescriptions of 50 patients were evaluated in this study. Drugs were prescribed according to the pathological factor associated with female infertility i.e. PCOS, PID etc. 31 patients were prescribed anti-oestrogen drugs (clomiphene) for anovulation, anti-obesity drugs (metformin) were prescribed in 36 prescriptions to deal with PCOS, 7 patients were prescribed antibiotics for PID infections , analgesics (NSAIDs) for pelvic pain were prescribed to 16 patients, a combination of oral-contraceptives( norgestrel/estradiol) prescribed to 29 patients for treating menstrual irregularities & 34 patients were prescribed other medications i.e.
calcium , iron, folic acid , vitamin D & E supplements. Usual combination of anti-obesity drugs, anti-oestrogen drugs & oral contraceptives was prescribed for treating PCOS and menstrual irregularities associated infertility & antibiotics with analgesics for PID.
Out of 50 patients, 9 patients have undergone surgical procedure i.e. operative laparoscopy and blockade of fallopian tubes was checked. Assisted reproduction was another intervention seen during the study which includes IVF, GIFT, intrauterine insemination & hysteroscopic hydrotubation. Out of 50 patients, 5 patients were treated with assisted reproduction.
| Medication | Frequency (N) | Percentage (%) | |
|---|---|---|---|
| Pharmacological Interventions | Anti-oestrogen drugs | 31 | 62% |
| Pharmacological Interventions | Anti-obesity drugs | 36 | 72% |
| Pharmacological Interventions | Antibiotics | 7 | 14% |
| Pharmacological Interventions | Analgesics | 16 | 32% |
| Pharmacological Interventions | Oral-contraceptives | 29 | 58% |
| Pharmacological Interventions | Others | 34 | 68% |
| Miscellaneous Interventions | Surgical treatment | 9 | 18% |
| Miscellaneous Interventions | Assisted reproduction | 5 | 10% |
Table 3: Treatment trends for management of infertility in females.
Discussion
Infertility, defined as the inability of a sexually active couple to conceive after 1 year of regular intercourse without contraception, affects approximately 15% of couples, and male factors are the cause in 20% -50% of cases [11]. Higher prevalence has been seen from 25-34 years of age group and lesser rate of prevalence has been seen from age group greater than 45 years. According to a survey conducted (July 1988 – June 1989) in three regions of France. The main exaggerating causes of female infertility were ovulation disorders (32%) and tubal damage (almost 26%), and of male infertility oligo-terato-asthenozoospermia (approximately 21%), asthenozoospermia (17%), teratozoospermia (10%) and azoospermia (9%) [12]. Further studies provide an evidence of endometriosis insights into lethal ovarian carcinogenesis resulting in female infertility at the age of 25 to 40 years [13]. Secondary type of infertility is much more common than primary type of infertility. The incidence of varicocele is much higher factor in secondary infertility compared with primary infertility [14]. Higher prevalence rate has been seen from females suffering from PCOS. The prevalence of polycystic ovaries, ovarian size and morphology, menstrual history, features of androgen excess, fertility status, serum hormone levels should be assessed from each participant to check PCOS. Most of the studies shows that serum levels of oestradiol and FSH were similar in PCOS and non‐PCOS women, but LH was distributed around a higher median in PCOS women. Median testosterone and androstenedione levels were the same in PCOS and non‐PCOS women. Ovarian volume (each ovary separately) is mostly larger in women with PCOS irrespective of current OCP (oral contraceptive pill) usage. The prevalence of polycystic ovarian morphology is much high but it was accompanied by minimal clinical manifestations and superficially no deleterious effects on earlier fertility [15]. All the participants were diagnosed mainly via ultrasonography in order to check the pelvic cavity and cysts in ovaries. Tubal patency was checked via laparoscopy and endocrine tests included FSH, LH detection, progesterone, androgens etc. ultrasound is most common investigational modality for checking ovaries and for estimation of female infertility reasons [16].
The current common use of Doppler ultrasound technique to examine blood flow in the uterus and ovaries in infertile patients and during early female pregnancy. The overall basics of Doppler ultrasound and different techniques of measuring blood flow are also used from the viewpoint of the technician who may be unfamiliar with physics and terminology of Doppler. The normal values in menstrual cycle and the association of uterine and ovarian blood flow to infertility and to implantation following in- vitro fertilization can be presented by this technique. Normal standards for uterine blood flow in the first 16 weeks of pregnancy and effect of sex steroids and ovulation induction on their values can be described. The possible relationship of defective uterine blood flow and effect of drugs can be explored. Doppler blood flow studies also provide significant information about possible causes of some of disorders of infertility and early pregnancy and methods of treatment [17].
Ultrasound has become an important help for the judgement of infertility by demonstration of pelvic organs, growing ovarian follicles, of intra-follicular arrangements and the cyclic uterine endometrial changes. Ultrasonic discriminations of ovaries and their developments such as the ovarian artery can be described. By ultrasound, average ovarian blood flow can be measured. During hormone stimulated cycles, the overall ultrasonic examination is repeated through ovulation, induction and even subsequently. The average diameter of growing follicle is also measured. Femara (generic letrozole) and Clomid (having generic clomiphene) are fertility medications used for exciting ovulation. Combination drug therapies have been considered to improve pregnancy rates [18]. Previously, combinations of different hormonal therapies (anti-estrogen, tamoxifen with an androgen, testosterone undecanoate) in 212 patients with idiopathic oligozoospermia and the 82 normozoospermic men with female factor subfertility significantly enhanced sperm parameters and the spontaneous pregnancy rate [19]. Other smaller randomized trials using the combinations of hormonal therapy with antioxidants (anti-estrogen, clomiphene with an antioxidant, L-carnitine / vitamin E) have shown previously a beneficial effect on sperm considerations and pregnancy rates [20]. The antioxidants in combination had a helpful impact on overall pregnancy rates [21].
Conclusion
It is concluded from the study that the percentage prevalence of female infertility among ages was higher in age group (25-34) years (76%) and it was mostly secondary infertility (54%). The main pathological factor of female infertility in Sialkot city was PCOS, which was 52% of evaluated patients. Commonly used diagnostic tools were ultrasonography with prevalence of (100%) and endocrine tests (72%). In prescription trend, anti-obesity drugs, anti- oestrogen drugs and oral-contraceptives were commonly prescribed and other treatment interventions were also seen in few patients.
References
-
Habbema JDF, Collins J, Leridon H, Evers JL, Lunenfeld B, et al. (2004) Towards less confusing terminology in reproductive medicine: a proposal. Human Reproduction 19(7): 1497-1501.
-
Unuane D, Tournaye H, Velkeniers B, Poppe K (2011) Endocrine disorders & female infertility. Best Practice & Research Clinical Endocrinology & Metabolism 25(6): 861-873.
-
Boivin J, Bunting L, Collins JA, Nygren KG (2007) International estimates of infertility prevalence and treatment-seeking: potential need and demand for infertility medical care. Human Reproduction 22(6): 1506-1512.
-
Brunham RC, Maclean IW, Binns B, Peeling RW (1985) Chlamydia trachomatis: its role in tubal infertility. Journal of Infectious Diseases 152(6): 1275-1282.
-
Dubin L, Amelar RD (1971) Etiologic factors in 1294 consecutive cases of male infertility. Fertility and sterility 22(8): 469-474.
-
Mounsey AL, Wilgus A, Slawson DC (2006) Diagnosis and management of endometriosis. American family physician 74(4): 594-600.
-
Kim TJ, Anasti JN, Flack MR, Kimzey LM, Defensor RA, et al. (1997) Routine endocrine screening for patients with karyotypically normal spontaneous premature ovarian failure. Obstetrics & Gynecology 89(5): 777-779.
-
Afzelius BA, Eliasson R, Johnsen O, Lindholmer C (1975) Lack of dynein arms in immotile human spermatozoa. The Journal of cell biology 66(2): 225-232.
-
Brody S, Hill K, Mejia C, Bispham A, Warden G (2002) Sonohysteroscopy (SHS): a new diagnostic tool to identify uterine causes of implantation failure. Fertility and sterility 77: S13.
-
Macnaughton M (1973) Treatment of female infertility. Best Practice & Research Clinical Endocrinology & Metabolism 2(3): 545-560.
-
Gnoth C, Godehardt E, Frank Herrmann P, Friol K, Tigges J, et al. (2005) Definition and prevalence of subfertility and infertility. Human reproduction 20(5): 1144-1147.
-
Thonneau P, Marchand S, Tallec A, Ferial ML, Ducot B, et al. (1991) Incidence and main causes of infertility in a resident population (1 850 000) of three French regions (1988-1989). Human reproduction 6(6): 811-816.
-
Brinton LA, Lamb EJ, Moghissi KS, Scoccia B, Althuis MD, et al. (2004) Ovarian cancer risk associated with varying causes of infertility. Fertility and sterility 82(2): 405-414.
-
Gorelick JI, Goldstein M (1993) Loss of fertility in men with varicocele. Fertility and sterility 59(3): 613-616.
-
Clayton RN, Ogden V, Hodgkinson J, Worswick L, Rodin DA, et al. (1992) How common are polycystic ovaries in normal women and what is their significance for the fertility of the population? Clinical Endocrinology 37(2): 127-134.
-
Brody S, Hill K, Mejia C, Bispham A, Warden G (2002) Sonohysteroscopy (SHS): a new diagnostic tool to identify uterine causes of implantation failure. Fertility and sterility 77: S13.
-
Dickey RP (1997) Doppler ultrasound investigation of uterine and ovarian blood flow in infertility and early pregnancy. Human reproduction update 3(5): 467-503.
-
Adamopoulos DA, Nicopoulou S, Kapolla N, Karamertzanis M, Andreou E (1997) The combination of testosterone undecanoate with tamoxifen citrate enhances the effects of each agent given independently on seminal parameters in men with idiopathic oligozoospermia. Fertility and sterility 67(4): 756-762.
-
Adamopoulos DA, Pappa A, Billa E, Nicopoulou S, Koukkou E, et al. (2003) Effectiveness of combined tamoxifen citrate and testosterone undecanoate treatment in men with idiopathic oligozoospermia. Fertility and sterility 80(4): 914-920.
-
Moradi M, Moradi A, Alemi M, Ahmadnia H, Abdi H, et al. (2010) Safety and efficacy of clomiphene citrate and L-carnitine in idiopathic male infertility: a comparative study. Urology journal 7(3): 188-193.
-
Showell MG, Mackenzie Proctor R, Brown J, Yazdani A, Stankiewicz MT, et al. (2014) Antioxidants for male subfertility. Cochrane Database of Systematic Reviews (12): CD007411.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions