Covid and the Elderly What are the Lessons We´ve Learned?
Older people are disproportionately affected by the COVID-19 pandemic; although it is not the most affected age group, it is the one with the most serious forms and the highest fatality. This may be related to several issues: higher proportion of comorbidities such as hypertension, diabetes mellitus, cardiovascular disease, chronic obstructive pulmonary disease, etc, all of which are associated with both a higher frequency of infection and a higher fatality rate; less psychological and biological reserves, and finally immune senescence: immunological changes associated with aging. The pandemic presents itself, evolves diversely and impacts in different ways in the lives of young adults and elderly. In this brief review we try to explore diagnosis and evolvement of COVID-19 and impact of isolation in older adults.
Introduction
Older people are disproportionately affected by the COVID-19 pandemic [1]; Reports of the Covid19 pandemic show a greater vulnerability of the elderly: although it is not the most affected age group, it is the one with the most serious forms and the highest fatality. The causes of this association are multiple [2, 3].
On one hand, older people have a higher proportion of comorbidities such as hypertension, diabetes mellitus, cardiovascular disease, chronic obstructive pulmonary disease, etc, all of which are associated with both a higher frequency of infection and a higher fatality rate. On the other hand psychological and biological reserves are diminished in this population compared to that of young adults, and finally immunological changes associated with aging affect them negatively [4, 5, 6].
In Argentina, as well as in other countries, most of the cases were seen in young adults, but the case fatality rate (CFR) was higher in the elderly; as shown in graphic 1. By December 16th, 1,537,169 cases and 41763 deaths were reported in our country (data National Ministry of Health).
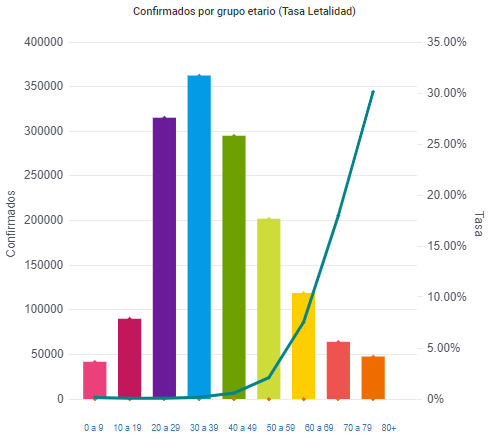
Graphic 1: Confirmed cases an case fatality rate according to age (National Ministry of Health. Argentina).
In graphic 2 we can see that in both men and women, the largest number of deaths occurred in older people.
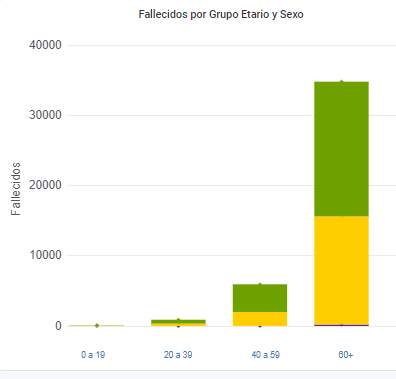
Graphic 2: Deaths according to gender and age (National Ministry of Health. Argentina) (December 16th 2020).
The pandemic presents itself, evolves diversely and impacts in different ways in the lives of young adults and elderly.
Different Clinical Presentation of Covid19 in the Elderly
Older people may develop uncommon signs of coronavirus infection. Differences in the clinical picture presented by elderly subjects compared to the younger are common in diseases in general, and in infectious diseases in particular [7]. This may result in a delayed diagnosis, or even more frequent diagnostic errors, which is detrimental to the future of these elderly patients. Thus, it is important to consider the risk of atypical presentation of coronavirus infection [8, 9].
The most frequent clinical and biological characteristics reported by different series differ between young and older adults. The main signs and symptoms that are pointed out as indicative of a suspected case such as fever, cough, odynophagia, respiratory difficulty, anosmia and dysgeusia are often not evident in the elderly.
The febrile response in older people may be absent even in severe infections in up to 30% of cases and up to 50% in frail* patients. Many times the drugs that patients consume for other causes such as chronic pain (NSAIDs, corticosteroids, etc.) alter the febrile response. Elderly also present a lower response to endogenous pyrogens and difficulties in the vasomotor response. All of this lead to a lower febrile response in these patients [10].
*Typical characteristics of frail patients are involuntary weight loss, cognitive disturbances, reduced mobility, and need for assistance in activities of daily living. Frailty scales such as FRAIL are a simple aid for classifying these patients [11].
Cough and respiratory distress: it is common for patients to present chronic cough either associated with drugs or with gastroesophageal reflux; in addition, the changes that occur in the respiratory system as age increases, cause the mechanisms of mucociliary clearance to be altered and the effectiveness of coughing decreases [12, 13].
Anosmia or dysgeusia: many patients have previous alterations in taste or smell and especially in patients with frailty it is difficult to investigate these symptoms [14].
It is common for older adults to present diffuse and unspecific symptoms in different infections, which makes diagnosis difficult. Symptoms such as deterioration of baseline functional status, falls, acute confusional syndrome, dehydration, desaturation, and hyporexia are frequent indicators of infections in this population [15].
Several authors noted that fever was less frequent in older people than in their younger counterparts affected with COVID-19 [16, 17, 18, 19].
Huang et al describe coronavirus infection in the first adults during the outbreak in China, with a median age of 49 years. Chinnadurai, et al. [20] instead, describe a much older population with a median age of 79 years. Comparing both papers we can see that the younger had more often fever (88.7%), cough (67.8%), asthenia/fatigue (38.1%), and sputum (33.7%). Diarrhea was rare (3.8%) [20, 21]. On the opposite, in the older population more than a quarter had diarrhea, while delirium was present in more than 60%. A fall was the first sign of the infection for more than a quarter of the elderly. Thrombopenia and lymphopenia have been frequently observed in adult patients with COVID-19. In Medetalibeyoglu´s series, lymphopenia was more frequent than thrombopenia or leukopenia. Inflammation, renal impairment or liver impairment affected more than half of observed patients. Comorbidities or pre-existing frailty could influence the frequency of these signs in older people with COVID-19 infection.
For all that has been said, it is essential to be alert to minimal symptoms, changes in patient´s baseline, desaturation, acute confusional syndrome, falls, hypoxemia (which can manifest itself as any of the above!) [22].
As an interesting diagnosis tool, D ´adamo et al raised “the ABCD diagnosis of Covid19” in older adults [23].
- A Awareness Be alert to the different forms of presentation of Covid19 infection, remembering the possibility of nonspecific symp- toms.
- B Behaviors Quickly take the necessary behaviors to evaluate and diag- nose the infection and thus be able to act with the AMs sus- pected of Covid.
- C Containment Contain the spread of infection to other individuals. In the case of patients in chronic care residences, screening pro- cedures should be established for both inmates and staff in charge.
- D Decisions Quickly decide the situation of the suspected MA with ad- equate diagnostic tests that allow it to be characterized as a confirmed case or to exclude it and avoid unnecessary isola- tion as well as delays in treatment.
Different Clinical Evolvement of Covid19 in the Elderly
Not only presentation, but clinical evolution as well is quite different in older adults, comparing them to the younger.
Symptoms described above, known as typical not only at diagnosis but during the disease such as fever, dry cough, fatigue, sputum production, shortness of breath, sore throat, headache, myalgia or arthralgia, chills, nausea or vomiting, nasal congestion, diarrhea, and less common as hemoptysis, or conjunctival congestion might or might not develop during the disease. Mild symptoms can be reported in some 80% of the patientes, bit are likely much more common in younger populations who may be undercounted in these estimates because they do not seek for medical attention or are not offered testing. Severe symptoms with shortness of breath and lung involvement are reported in 14% of the patients, and 5% develop critical illness [24].
The case fatality rate (CFR) in older adults may be beyond 8% , even 14.8% in those above the age of 80 in China, and up to 19.6% and 22.9% in the very old in Italy (older than 80 and 90 respectively) [25, 26].
Why the high mortality in older people? This population has high comorbidity, high prevalence of dementia and geriatric syndromes (especially in institutionalized patients, higher prevalence of frailty, and less physiological reserve and intrinsic capacity. Probably all those contribute negatively to older people’s response to disease and lead them to a bad outcome [27, 28]. In terms of comorbidities, while patients who reported no comorbid conditions had a CFR of 1.4%, patients with comorbid conditions had much higher rates: 13.2% for those with cardiovascular disease, 9.2% for diabetes, 8.4% for hypertension, 8.0% for chronic respiratory disease, and 7.6% for cancer; all of which are frequently present in the elderly [29].
In Argentina comorbid conditions were quite similar although more frequent in older adults, as shown in graphic 3. The most frequent comorbidities seen were diabetes, heart failure, neurological diseases, obesity, COPD, active oncological disease, kidney failure, active and past smoking, especially in older adults.
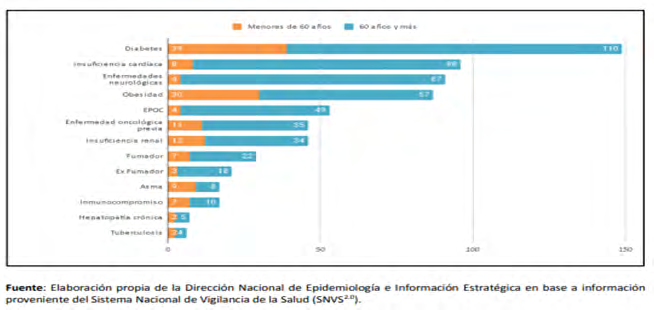
Graphic 3: Distribution of risk factors in confirmed deceased cases (National Direction of Epidemiology and Strategic information based on the National System of Health Surveillance.
Zhao, et al. [30] published differences in CT images between younger and elderly. Although a small number of patients (101 in total and only 14 older than 60 years), they pointed out that ground-glass opacities (>86%), and mixed GGO and consolidation were seen similar in both groups, consolidation alone was more common in older adults 41.4% vs 57.1% (nonsignificant P: 0.270) as well as pleural effusion (10.3% vs 35.7%) P: 0.011. 10% of the younger and none of the older patients had no signs in CT scan [30].
Isolation in the Elderly Impact on Daily Life
It is rational to protect older adults from infection through social isolation, however this measure can result in unintended consequences, since such measures are highly disruptive for individuals [31].
There is evidence that socially disconnected and isolated older adults are at increased risk of physical and mental health problems, including cardiovascular disease, stroke, depression, anxiety, dementia and premature death, and as a result can require additional health and social care support [32, 33, 34, 35]. Chronic loneliness has been associated with an increased number of doctor visits; in a study of 3,530 older adults living in the community in the United States, Gerst- Emerson et al. found an increased number of doctor’s visits for people reporting loneliness [36]. Low contact with friends in older adults, exclusion from social relationships and subjective feelings of exclusion have been negatively associated with well-being and associated with poor self- reported health [37, 38] Loneliness caused by social isolation has been associated with impaired cognitive function in older adults [39, 40, 41].
Those experiencing a high degree of loneliness have been found to be at increased risk of becoming physically frail. These data relate to social disconnection, isolation and loneliness more generally, as opposed to specifically in relation to social distancing in response to COVID-19 or other pandemics; therefore, self-isolation during pandemics may result in different physical and psychosocial consequences from loneliness at other times. However, this evidence suggests that the current social distancing policies could have important negative consequences, particularly if in place for an extended period. Final remarks:
- Although the group of the elderly is not the most affected in the COVID-19 Pandemic, it is the one with the most serious forms and the highest fatality rate.
- It is common for older adults to present diffuse and unspecific symptoms in different infections, such as COVID-19. Disease may present atypically with delirium, postural instability, desaturation, falls or diarrhea, without fever.
- The presence of comorbidities and immunological changes associated with immunosenescence are associated with the greater risk of the elderly for developing severe disease and mortality
- Especially in fragile patients a high diagnostic suspicion is required
- It is probable that the asymptomatic have an important role in the Covid transmission chain in relation to the elderly (frail / institutionalized / dependent)
- Social distancing and isolation may have negative consequences for older people, unrelated to COVID-19.
References
-
Liu W, Tao ZW, Lei W, Ming Li Y, Kui L, et al. (2020) Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease. Chin Med J (Engl) 133(9): 1032-1038.
-
Onder G, Rezza G, Brusaferro S (2020) Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 323(18): 1775-1776.
-
Williamson E, Walker AJ, Bhaskaran KJ, Bhaskaran K, Bacon S, et al. (2020) Open- SAFELY: factors associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients.
-
Bouza E, Brenes FJ, Domingo JD, JM Eiros Bouza, J González, et al. (2020) The situation of infection in the elderly in Spain: a multidisciplinary opinion document. Revista Española de Quimioterapia 33(5): 327-349.
-
Pawelec G (2012) Hallmarks of human “immunosenescence”: adaptation or dysregulation? Immun Ageing 9(1): 15.
-
Pawelec G (2018) Age and immunity: What is “immunosenescence”? Exp Gerontol 105: 4-9.
-
Janssens J, Krause K (2004) Pneumonia in very old. Lancet Infect Dis 4(2): 112-124.
-
Abbara A, Collin SM, Kon OM, Buell K, Sullivan A, et al. (2019) Time to diagnosis of tuberculosis is greater in older patients: a retrospective cohort review. ERJ Open Res 5(4): 00228-2018.
-
Godaert L, Bartholet S, Gazeuse Y, Brouste Y, Najioullah F, et al. (2018) Misdiagnosis of chikungunya virus infection: comparison of old and younger adults. J Am Geriatr Soc 66(9): 1768-1772.
-
Isaia G, Marinello R, Tibaldi V (2020) Atypical Presentation of Covid-19 in an Older Adult With Severe Alzheimer Disease. Am J Geriatr Psychiatry 28(7): 790- 791.
-
Morley JE, Vellas B, Abellan van Kan G, Anker SD, Bauer JM, et al. (2013). Frailty Consensus: A Call to Action Morley. Journal of the American Medical Directors Association 14(6): 392-397.
-
h t t p s : / / w w w. i n t ra m e d . n e t / c o n t e n i d o ve r. asp?contenidoid=94988
-
Dezube R (2019) Effects of Aging on the Respiratory System.
-
Syed Q, Hendler KT, Koncilja K (2016) The Impact of Aging and Medical Status on Dysgeusia. The American Journal of Medicine 129(7): 753.e1-6.
-
Berman P, Hogan DB, Fox RA (1987) The atypical presentation of infection in old age. Age Ageing 16(4): 201-207.
-
Medetalibeyoglu A, Senkal N, Kose M, Catma Y, Caparali EB, et al. (2020) Older Adults Hospitalized with Covid-19: Clinical Characteristics and Early Outcomes from a Single Center in Istanbul, Turkey. J Nutr Health Aging 24(9): 928-937.
-
Liu K, Chen Y, Lin R, Han K (2020) Clinical feature of COVID-19 in elderly patients: a comparison with young and middle-aged patients. J Infect 80(6): e14-e18.
-
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, et al. (2020) Clinical characteristics of coronavirus disease 2019 in China. New Eng J Med 382: 1708-1720.
-
Godaert L, Proye E, Tampere DD, Coulibaly PS, Hequet F, et al. (2020) Clinical characteristics of older patients: The experience of a geriatric short-stay unit dedicated to patients with COVID-19 in France. J Infect 81(1): e93-e94.
-
Chinnadurai R, Ogedengbe O, Agarwal P (2020) Older age and frailty are the chief predictors of mortality in COVID-19 patients admitted to an acute medical unit in a secondary care setting- a cohort study. BMC Geriatr 20(1): 409.
-
Huang C, Wang Y, Li X, Ren L, Zhao J, et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497-506.
-
Norman RE, Stall NM, Sinha Sk (2020) Typically Atypical: COVID‐19 Presenting as a Fall in an Older Adult. J Am Geriatr Soc 68(7): E36-E37.
-
D’Adamo H, Yoshikawa T, Ouslander J (2020) Coronavirus Disease 2019 in Geriatrics and Long-term Care: The ABCDs of COVID-19. J Am Geriatr Soc 68(5): 912-917.
-
Nanda A, krishna Vura NVR, Gravenstein S (2020) COVID-19 in older adults Aging Clinical and Experimental Research.
-
Wu Z, Mc Googan JM (2020) Characteristics of and important lessons from the Coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese CDC. JAMA 323 (13): 1239-1242.
-
(2020) Integrated surveillance of COVID-19 in Italy.
-
Cesari M (2018) Prevalence and risk factors for falls in an older community-dwelling population. J Gerontol A Biol Sci Med Sci 73: 1653-1660.
-
Bonanad C (2020) Coronavirus:the geriatric emergency of 2020. Joint document of the Section on Geriatric Cardiology of the Spanish Society of Cardiology and the Spanish Society of Geriatrics and GerontologyCoronavirus: the geriatric emergency of 2020. Joint document of the Section on Geriatric Cardiology of the Spanish Society of Cardiology and the Spanish Society of Geriatrics and Gerontology. Rev Esp Cardiol 73(7): 569-576.
-
Arentz M (2020) WHO-China Joint Mission. JAMA.
-
Zhao W (2020) Relation between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. AJR Am J Roentgenol 214(5): 1072-1077.
-
Wang C, Liu L, Hao X (2020) Evolving epidemiology and impact of non-pharmaceutical interventions on the outbreak of coronavirus disease 2019 in Wuhan, China. medRxiv 2020.03.03.20030593.
-
Cotterell N, Buffel T, Phillipson C (2018) Preventing social isolation in older people. Maturitas 113: 80-84.
-
Santini ZI, Jose PE, York Cornwell E (2020) Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): a longitudinal mediation analysis. Lancet Public Health 5: e62-70.
-
Courtin E, Knapp M (2017) Social isolation, loneliness and health in old age: a scoping review. Health Soc Care Community 25(3): 799-812.
-
Freedman A, Nicolle J (2020) Social isolation and loneliness: the new geriatric giants: approach for primary care. Can Fam Physician 66: 176-182.
-
Gerst Emerson K, Jayawardhana J (2015) Loneliness as a public health issue: the impact of loneliness on health care utilization among older adults. Am J Public Health 105(5): 1013-1039.
-
Dahlberg L, McKee KJ (2018) Social exclusion and well- being among older adults in rural and urban areas. Arch Gerontol Geriatr 79: 176-184.
-
Feng Z, Jones K, Phillips DR (2019) Social exclusion, self-rated health and depression among older people in China: evidence from a national survey of older persons. Arch Gerontol Geriatr 82: 238-244.
-
Yang R, Wang H, Edelman LS (2020) Loneliness as a mediator of the impact of social isolation on cognitive functioning of Chinese older adults. Age Ageing 49(4): 599-604.
-
Gale CR, Westbury L, Cooper C (2018) Social isolation and loneliness as risk factors for the progression of frailty: the English longitudinal study of ageing. Age Ageing 47: 392-397.
-
Nancy Morrow Howell, Natalie Galucia , Emma Swinford. Recovering from the covid 18 pandemic: a focus on older adults. Journal of Aging & social Policy 32(4-5): 526-535.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions