A Review on: Lumpy Skin Disease: Enhance Awareness on the Epidemiological situation and Diagnosis; Prevention and Control Measures in Ethiopia
Lumpy skin disease (LSD) is an economically significant viral disease of cattle and caused by lumpy skin disease virus (LSDV). The virus is belonging to the genus Capri poxvirus (CaPV) of the family Poxviridae. Recently, the disease has been rapidly spreading to the Middle East, South east Europe and parts of Russian federation. The disease causes significant economic loss due to hide damage, loss of milk production, mastitis, infertility and death. Clinically, LSD is characterized by circumscribed skin nodules, fever, and abortions in females and sterility in males. LSD damages hides and causes death due to secondary bacterial infections. LSD is principally transmitted by blood-feeding arthropod vectors. However, transmission of the disease between animals is inefficient. Diagnosis is mainly based on observation of clinical signs and identification of the agent using conventional and real-time PCR methods, electron microscopy, and isolation of the virus in cell cultures, and using conventional serological tests. In endemic countries, vaccination is the only effective method to control the disease using live attenuated vaccines derived from Kenyan sheep and goat pox virus (KSGP) strains. However, there are reports of insufficient protection of the existing vaccines. Therefore; there is a need for more extensive data from the field and for larger-scale clinical trials to ensure the efficacy and safety of the current vaccines.
Introduction
Lumpy skin disease (LSD) is an emerging viral disease of cattle caused by LSD virus (LSDV), belongs to the genus Capri poxvirus (CaPV) in the family Poxviridae which can lead to significant economic losses [1, 2]. The disease is characterized by circumscribed firm skin nodules covering all parts of the body, lesions in the mouth, pharynx, respiratory tract, pyrexia, enlarged lymph nodes [3, 4].
Until 1989, Lumpy skin disease is limited to African continent where the disease imposes serious constraints on livestock production and it is rapidly spreading throughout the Middle East regions and causes serious economic loss to the livestock industry [5, 6, 7, 8]. Furthermore, currently the disease has become a risk for European and Asian countries by moving beyond its usual territory [2]. LSD hinders cattle industry due to reduced milk production, mastitis, infertility, abortion, damaged hides, and sometimes death because of secondary bacterial infections [9, 10].
Severity of clinical signs depends on the strain of the virus and breed of infected cattle [3]. Impacts of the global climate changes were considered to have the potential risk factor to establish the disease outside Africa. In Ethiopia, LSD was first observed in the North-west part of the country in 1983 [11]. Now the disease has been spreading to almost all the regions and agro-ecological zones of the country [12, 13]. Ethiopia has the largest livestock population in Africa. The country has 60.39 million cattle, 31.3 million sheep and
32.74 million goat population [14].
Livestock industry plays an important role in the overall development of the country’s economy but, the country is facing serious economic losses from viral diseases of cattle. Major epidemic outbreaks of LSD have been reported in between 2000 and 2007 in different regional states of Ethiopia; Amhara, Oromiya, Southern Nations, Nationalities and Peoples regions, Tigray, et al. [12]. Similar outbreak eruption had also been reported in all major parts of the country between 2000 and 2015 [13].
Vaccination is the only effective method to control the disease in endemic areas. A movement restriction of infected and exposed animals alone is usually not effective [15]. Live attenuated Kenyan sheep and goat pox (KSGP) vaccines produced in Ethiopia, at National Veterinary Institute (NVI), and the most commonly used [16]. However, outbreaks were reported after animals have been vaccinated against LSD from different countries [17].
Moreover, sheep pox virus based vaccines have also elicited incomplete protection against LSDV [18]. Given that, LSD is economically important trans-boundary livestock disease and/or major constraints for livestock development in Ethiopia. Therefore, the objectives of this review article are:
- To enhance awareness on the epidemiology, diagnosis, prevention and control measures of Lumpy skin disease
- To recommend the development of new effective vaccines by characterizing LSDV circulating in the field
Literature Review
a. Epidemiology i. Historical Background of Lumpy Skin Disease: Lumpy skin disease was first recorded in Zambia in 1929. Soon after, the disease spread to other African countries causing severe outbreaks in the horn of Africa [19]. In 1970, it spread north into the Sudan and between 1981 and 1986 reached to Tanzania, Kenya, Zimbabwe, Somalia and Cameroon [20]. The disease is now enzootic throughout sub-Saharan African countries [19].
LSD was first diagnosed outside of Africa in Israel in 1989 and in subsequent years, cases were reported in Bahrain, Kuwait, Oman, Yemen, Lebanon, and Jordan. In 2006, the disease was re-introduced into Egypt through imported cattle from East Africa, and subsequently emerged throughout the Middle East. Since 2015 widespread LSDV outbreaks have occurred across several eastern European countries (Russia, Turkey, Greece, Albania, Bulgaria, Montenegro, Serbia, and Macedonia) [2, 21, 22].
b. Etiology Lumpy skin disease (LSD) is caused by lumpy skin disease virus (LSDV), belongs to the family Poxviridae, genus Capri poxvirus. This virus is closely related to sheep pox (SPPV) and Goat pox virus (GTPV) [23]. Serologically, it is difficult to differentiate CaPVs. Thus, LSDV is antigenically related to SPPV and GTPV [24]. The members of this family are among the largest of all viruses, enveloped , linear ovoid shape with a molecular brick shaped or ovoid virion measuring 220- 450nm by 140-266nm (Figure 1). LSDV is susceptible to sun light and detergents containing lipid solvents. The virus could be inactivated after heating for 1 hour at 55°C [25].
However, it withstands drying, pH changes if not an extreme pH and can remain viable for months in dark room such as infected animal shade off its host. LSDV can persist in skin plugs for about 42 days. It is likely that the viral type inclusion body protein in infected cells may protect the vision after the scab has disintegrated, although not yet proven [1].
c. Viral Genome LSDV has double-stranded DNA genome of about 151kb. The full-genome sequencing of LSDV consists of a central coding region bounded by identical 2.4 kbp-inverted terminal repeats and contains 156 putative genes [26]. These genes encode several pox viral proteins known to be structural or involved in virion morphogenesis and assembly. The terminal genomic sequences contain a unique complement of at least 34 genes which are responsible in virulence, host range and/ or immune evasion [27, 28].
The CaPVs homolog of G-protein-coupled chemokine receptor (GPCR) gene is one of the variable genes within the CaPVs and used for genetic differentiation between members of CaPV [26, 29].
Capri poxvirus nucleotide sequences are highly conserved and there is more than 95% homology amongst LSDV, SPPV and GTPV, LSDV is genetically and antigenically closely related to a strain of sheep and goat pox virus [28, 30]. LSDV has an additional nine genes that are non-functional in sheep pox and goat poxviruses, some of which are likely responsible for their ability to infect cattle [26].
Comparative sequence analysis of the two field isolates of LSDV with the genome of the South African Onderstepoort vaccine strain suggests that Capri poxvirus virulence are linked to a number of genes putatively involved in host immune-modulation [28]. Lumpy skin disease viruses have complement of genes such as IL-10, (IF-γ) receptor; IL-1R, IFN-α/β binding protein and IL-18 (binding protein) are secreted and responsible for modulation or evasion of host immune response, inhibition of host cell apoptosis and in cell or tissue tropism. Entrance of the virion particles in to the host cell membrane undergoes penetration and uncoating to carry out its replication independently to the host nucleus [31, 32].
![Figure 1: General structure of Capripoxvirus Source: https://viralzone.expasy.org/152 (accessed 03 May, 2020) **d. Viral Replication** Poxviruses carry out both replication and transcription their genome within the cytoplasm of infected cells and encode most of the proteins required for the synthesis of viral macro-molecules. After fusion of the virion with the plasma membrane or via endocytosis, the viral core has released into the cytoplasm. Transcriptase released from the core of the virion facilitates formation of mRNA within minutes after infection [33]. The polypeptides produced by translation of these mRNAs complete the uncoating of the core before the actual viral DNA synthesis begins 1.5 to 6 hours of infection. Two forms of virion have released from the infected cells (virion with one membrane, and virion with two membranes) and both types are infectious [34]. **e.** **Host Range** LSDV mainly affects cattle but also observed in domestic Asian water buffaloes [35,36]. The European breed (Bos Taurus) is usually more susceptible than Zebu or Sub- Saharan Africa breed (Bos indicus). LSD-like lesions have been observed in intra-dermally inoculated with LSD [37]. Moreover, giraffe and impala has experimentally infected with LSDV. Domesticated buffaloes are more susceptible to LSDV than wild buffaloes [38]. LSD clinical signs have also been observed in a two year female Arabian Oryx [39].](/fulltextimages/6690/fig_1.png)
Figure 1: General structure of Capripoxvirus Source: https://viralzone.expasy.org/152 (accessed 03 May, 2020) d. Viral Replication Poxviruses carry out both replication and transcription their genome within the cytoplasm of infected cells and encode most of the proteins required for the synthesis of viral macro-molecules. After fusion of the virion with the plasma membrane or via endocytosis, the viral core has released into the cytoplasm. Transcriptase released from the core of the virion facilitates formation of mRNA within minutes after infection [33]. The polypeptides produced by translation of these mRNAs complete the uncoating of the core before the actual viral DNA synthesis begins 1.5 to 6 hours of infection. Two forms of virion have released from the infected cells (virion with one membrane, and virion with two membranes) and both types are infectious [34]. e. Host Range LSDV mainly affects cattle but also observed in domestic Asian water buffaloes [35, 36]. The European breed (Bos Taurus) is usually more susceptible than Zebu or Sub- Saharan Africa breed (Bos indicus). LSD-like lesions have been observed in intra-dermally inoculated with LSD [37]. Moreover, giraffe and impala has experimentally infected with LSDV. Domesticated buffaloes are more susceptible to LSDV than wild buffaloes [38]. LSD clinical signs have also been observed in a two year female Arabian Oryx [39].
f. Transmission The principal means of transmission is believed to be mechanically by biting and blood-feeding arthropods. Under experimental condition, female mosquitoes such as Aedes aegypti have been also involved in the transmission of LSDV [10, 40]. Experimentally the virus was recovered from Stomoxys, Biomyia, Musca, Culicoides and Glossina species that may have a potential to transmit LSD, as all feed voraciously upon domestic cattle [41].
Three common African hard tick species, such as, brown tick (Rhipicephalus appendiculatus), the bont tick (Amblyomma hebraeum) and the African blue tick (Rhipicephalus (Boophilus) decoloratus) have been recorded in the transmission and epidemiology of LSD [2, 42]. Direct transmission of LSD by contact between animals is inefficient [3].
However, husbandry practices such as communal grazing and watering troughs, introduction of new animals to the herd might contribute towards the spread of the disease [43]. Secretions of infected animals include milk of lactating cows, blood, nasal and lachrymal, semen and saliva may be sources for the transmission of LSDV when nodules on the mucous membranes of the eyes, nose, mouth, rectum, udder and genitalia are ulcerated [1].
Experimentally, LSDV has been isolated from infected semen [43]. Similarly, transmission of LSDV to heifers via semen has been clearly demonstrated [44]. In most of Sub- Saharan Africa, LSD has been observed following the rainy seasons. LSD outbreaks are associated with the rainy season due to the abundance of arthropod vectors [45]. However, the incidence drops during the dry and cold weather seasons. In Ethiopia, higher prevalence of LSD has been related with risk factors like warm, humid agro-climate and abundance of vector population [12].
g. Morbidity and Mortality Rates In outbreaks of the disease, morbidity and mortality of the disease varies extremely depending on the ages, breeds, geographic location, and climatic condition, and virus virulence, immunological status of the host and the abundance of arthropod vectors [19]. Naturally, Bos Taurus (European breed) is more susceptible than BIos Indicus (local Zebu) and cows at peak lactations are usually the most severely affected [46].
The morbidity can reach as high as 100% in natural outbreaks while mortality rate rarely exceeds 5% [1]. In Ethiopia, the highest morbidity (15.1%) and mortality (5.37%) of LSD were recorded in vaccinated feedlot cattle [16]. Moreover, morbidity and mortality rates of 22.9% and 2.31% respectively reported in vaccinated cattle [47].
h. Geographic Distribution of Lumpy Skin Disease In the past, LSD was endemic throughout the entire continent of Africa, except Libya, Algeria, Morocco and Tunisia [19]. Now a days ,the disease has been moved beyond Africa and sporadic LSDV outbreaks were reported in the Middle East region; such as Israel, Bahrain, Kuwait, Oman, Yemen and the West Bank (Figure 2) [8].
![Figure 2: Geographical distribution of LSD, OIE Data [2]. https://www.researchgate.net/figure/Geographical- distribution-of-lumpy-skin-disease_fig1_283791807 [accessed 27 Jul, 2020].](/fulltextimages/6690/fig_2.png)
Similarly, in recent times, new cases of LSDV have been reported in Iran, Azerbaijan, Iraq, Greece, and Cyprus between 2014 and 2015 [21, 46]. Between 2015 and 2016, the first incursion of LSDV was reported in the European Union territory and in the northern Caucasus region of Russia [21, 46]. Lebanon and Jordan joined LSD-affected countries in 2012 and 2013. Moreover, the armed Conflicts in Syria may allow the disease to spread into LSDV free European countries using Turkey as a portal of introduction [2].
i. Status of Lumpy Skin Disease in Ethiopia Currently LSD has been recorded to almost all the regions and agro-ecological zones of Ethiopia [11, 12]. However, according to the country’s outbreak report database, at least one LSD outbreak was occurred from the period 2000- 2009. As a result, Amhara and West Oromiya in 2000/2001, Oromiya and SNNP regions in 2003/2004, Tigray, Amhara and Benishangul regions in 2006/2007 and the outbreak numbers were progressively increased in central parts of Oromiya region in 2007/2009 [12].
LSD epidemic reoccurs after an interval of 5-6 years cycle in unvaccinated cattle population [30]. This also supports which stated that, outbreak occurs in epidemics several years apart. In Ethiopia, the national disease outbreak report during these 10 years has showed that the disease spreads almost too all the regional states of the country and in different agro- climatic zones [12, 48].
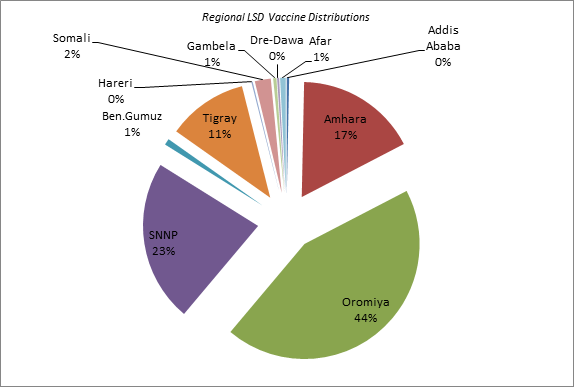
Based on outbreak reports, KS-1 vaccine distributions were carried out from the period 2014 to 2018 (Table 1) in different regional states of Ethiopian to prevent cattle against LSD. The regional delivery of the vaccines indicates that, the greatest number of live attenuated KS-1 vaccines vaccine sales in National Veterinary Institute (NVI) revealed that the number of LSD outbreak was increased (personal communication from vaccine sales directorate).
| Regions | 2014 | 2015 | 2016 | 2017 | 2018 | Total |
|---|---|---|---|---|---|---|
| Addis Ababa | 93,200 | 194,840 | 110,800 | 2,800 | 8,600 | 410,240 |
| Amhara | 4,481,000 | 5,335,000 | 662,150 | 3,861,500 | 6,809,800 | 21,149,450 |
| Oromiya | 11,301,400 | 9,352,860 | 13,921,340 | 8,653,500 | 11,061,800 | 54,290,900 |
| SNNP | 2,281,100 | 6,787,400 | 8,142,690 | 3,000,700 | 8,032,500 | 28,244,390 |
| Ben.Gumuz | 204,200 | 280,300 | 340,000 | 278,200 | 1,102,700 | |
| Tigray | 2,700,000 | 2,900,000 | 771,290 | 3,600,000 | 4,000,000 | 13,971,290 |
| Hareri | - | - | 205,000 | 25,000 | - | 230,000 |
| Somali | - | - | 1,477,500 | 1,000,000 | 300,000 | 2,777,500 |
| Gambela | - | 560,300 | - | - | - | 560,300 |
| Dre-Dawa | 50,000 | 100,000 | 100,400 | 100,000 | 300 | 350,700 |
| Afar | - | 200 | 243,550 | 240,000 | 501,600 | 985,350.00 |
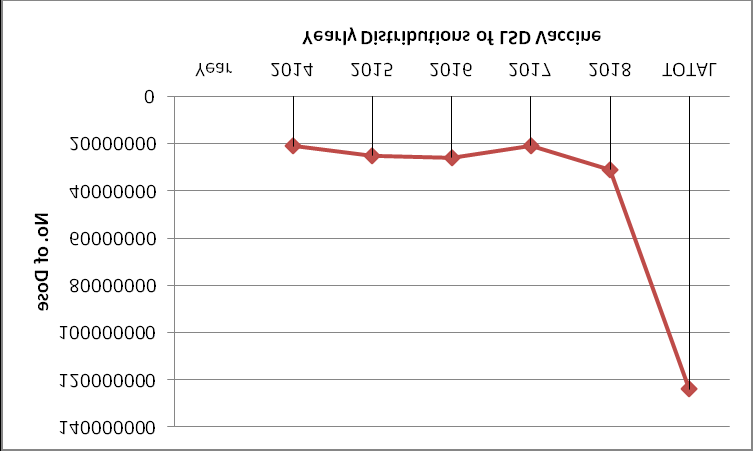
| Grand Total | 21,110,900 | 25,230,600 | 25,915,020 | 20,823,500 | 30,992,800 | 123,662,580 |
Table 1: Yearly distribution of LSDV vaccines from 2014-2018. Source: National Veterinary Institute’s Sales Directorate.
Annually, LSD vaccine distributions were increasing (except in 2017) from the period 2014 to 2018 (Figure 4). In 2018, the highest number of LSD vaccines (13%) was distributed within the country to control the disease; this trend has showed that LSD outbreaks are dramatically increasing in Oromiya, SNNP, and Amhara and Tigray regions in every year. Most of the LSD vaccine sales in Ethiopia have been carried out consistently associated with outbreaks of the livestock diseases; because mainly reactive vaccination campaigns have been practiced using KS-1 vaccine following outbreak reports (also applies for other animal diseases in Ethiopia).
However; timely diagnosis of susceptible animals are important to implement LSD control measures. Disease prevention should be implemented via vaccination with sheep pox and attenuated LSDV based vaccines [48]. In 2014, field visits were carried out in some districts of Ethiopia such as; Debre-Zeit, Addis Ababa, Ambo, Ginchi, Holeta and Selale based on LSD outbreak reports to NVI. I was conducted interview with cattle owners and veterinarians about the prevalence of the disease and their vaccination strategy to control the disease. Some owners started vaccinating animals when the disease is already circulating in the area. Among the vaccinated group some animals developed clinical sign three to six days following vaccination with live attenuated KSGP vaccines.
However, animals will develop protective immunity from 10 to 21 days post vaccination, and then require an annual booster dose [49]. Some cattle owners also did not vaccinate their animals for the last 5-6 years and this could be an indication of lack of sufficient herd immunity. Some owners were not willing to vaccinate lactating cows and beef cattle due to lack of awareness. The storage temperature was not maintained as manufacturer’s labeled (-20OC. Healthy and incubating animals were vaccinated with the same needles. A few number of dairy farms followed regular vaccination programs are protected from LSD. Therefore this will be the reason of detecting clinical signs in vaccinated animals with KSGP.
j. Economic Importance of the Disease Due to its rapid spread of the virus in susceptible cattle populations and its economic consequences on the global cattle industry, LSD is categorized as a modifiable disease by the World Organization for Animal Health (OIE) [19].
The economic importance of LSD is reflected with loss of milk production, temporary or permanent sterility in bulls and cows, damage to hides and death due to secondary bacterial infections, costly control and eradication measures and enforced animal movement restrictions [19, 20, 50]. Moreover, LSD is one of the trans-boundary diseases extending beyond its traditional boundaries. Hence, movement restriction of live animals and animal products can significantly affect the global trade [2].
In Ethiopia, the financial losses estimated based on milk, beef, draught power, mortality, treatment and vaccination costs for individual head of local zebu to be 6.43 USD and for the Holstein Friesian 58 USD [12] and the total loss of USD 667,786 in feedlots in and around Adama due to mortality and rejection [50]. Furthermore, total losses of 51,590 USD from death of 108 cattle had been calculated in central Ethiopia [16].
Diagnosis
Diagnosis of LSD is often based on characteristic clinical signs and clinical diagnosis. In naturally infected animals, the following Clinical manifestations have been observed: such as; Lachrymation, nasal discharge, enlarged lymph nodes, high fever (>40.50C), drop in milk yield, generalized skin nodules (Figure5), necrotic pox lesions around muzzle (Figure 6), Skin lesions in the legs and secondary bacterial infections, deep scab formations (sit-fast) (Figure 7), and mastitis [51].
Milder forms of LSD could be confused with other diseases causing skin lesions such as pseudo-lumpy skin disease (bovine herpesvirus-2 infection), insect bites, demodecosis, and dermatophilosis. Moreover, diseases causing mucosal lesions, such as Rinder pest, bovine viral diarrhea/mucosal disease, and bovine malignant catarrhal fever, also makes field diagnosis complex [49].


![Figure 7: Necrotic nodules and deep scab formation (sit- fast). Source: Author, 2014 (figures 5, 6 and 7) Effective control or eradication of LSD in endemic and non-endemic areas requires rapid and accurate diagnostic methods to confirm a presumptive diagnosis [52]. However, mild and subclinical forms require rapid and reliable laboratory testing to confirm diagnosis [53]. Most commonly used methods of diagnosing LSD are detecting LSDV DNA which is most rapidly done by using the polymerase chain reaction method (PCR) [54].](/fulltextimages/6690/fig_7.png)
Figure 7: Necrotic nodules and deep scab formation (sit- fast). Source: Author, 2014 (figures 5, 6 and 7) Effective control or eradication of LSD in endemic and non-endemic areas requires rapid and accurate diagnostic methods to confirm a presumptive diagnosis [52]. However, mild and subclinical forms require rapid and reliable laboratory testing to confirm diagnosis [53]. Most commonly used methods of diagnosing LSD are detecting LSDV DNA which is most rapidly done by using the polymerase chain reaction method (PCR) [54].
A variety of molecular tests using Capripoxvirus-specific primers are considered sensitive and specific for LSDV identification [29, 55]. Electron microscopy can be used to identify the classic poxvirus virion but cannot differentiate to genus or species level [49], and virus isolation using cell culture followed by PCR is important to confirm the virus identity [56]. Virus isolation on primary or secondary bovine dermis cells or lamb testis cells is considered to be the most sensitive. All CaPVs share a common major antigen for neutralizing antibodies, therefore; it is not possible to distinguish strains of CaPVs using serology-based diagnostic techniques [49].
Virus neutralization tests and electron microscopy examination are widely used as gold standard methods for the detection of CaPV infection [56]. Serological assay methods such as indirect enzyme linked immuno-sorbent assay (iELISA), western blotting, agar gel immuno-diffusion test and the indirect fluorescent antibody test are also used to diagnose LSD. However, Serological assessment of antibodies to a CaPVs may sometimes be difficult due to the cross-reactivity encountered with other poxviruses as well as to the low antibody titers elicited in some animals following mild infection or vaccination. Therefore, PCR was the test of choice for rapid detection and identification of the LSD outbreak causative agents [49].
k. Treatment, Prevention and Control Unfortunately there are no specific antiviral drugs available for the treatment of lumpy skin disease. However, Sick animals may be removed from the herd and given supportive treatment such as antibiotics, anti-inflammatory drugs, and vitamin injections to treat secondary bacterial infections or to improve the animal’s appetite [57]. LSD thought to be transmitted primarily by blood-feeding insects; hence quarantine and movement restriction alone are not very effective to control LSD unless supported by mass vaccination [57]. Therefore, efficient insect control may reduce the rate of LSDV transmission [58]. All strains of CaPVs from cattle, sheep and goat origin, share a common major antigen that makes it possible to use sheep pox or goat pox vaccine against LSDV infection in cattle [59].
In endemic countries, vaccination against LSD with live attenuated vaccines are the only effective method to control and prevent the disease [60]. Because immunity to CaPVs is mainly cell mediated and is better stimulated by the use of live vaccines. CaPV vaccine strains include LSDV Neethling, Kenyan sheep and goat pox virus (KSGPV) O-240 and O-180 strains, Yugoslavian RM65 sheep pox (SPP) strain, Romanian SPP, and Gorgan goat pox (GTP) strains have been used for the control of LSD [5, 18, 59]. Homologous live attenuated (Neethling strain) LSD vaccines are more successful than vaccines based on attenuated sheep pox viruses. Heterologous live attenuated virus vaccine may cause local and sometimes severe reactions [57].
Partial sequences of (KSGPV) O-240 strain has shown to be LSDV and not SPPV or GTPV [61]. Soon after, the complete genome sequences of the strain KSGP O-240 was confirmed to be LSDV [62]. In 2006, the use of live attenuated KSGP O-240 vaccine strain in Egypt [63] and RM65 SPP vaccine to cattle from 2006 and 2007 did not provide complete protection against LSDV in Israel [18]. Similar phenomenon has also been reported in Egypt in 2016 [64]. In Ethiopia, the KS- 1vaccine did not provide complete protection against LSDV. Then, challenge experiments has to be carried out to measure cellular and humoral immune responses [16]. However, field report in Kenya has showed that the KSGP strain is safe and protective [65]. Thus, vaccines with demonstrated safety and efficacy in challenge experiments have been recommended to solve these disagreements [66].
Conclusion
In conclusion, the present review has shown that LSDV is prevalent to almost all the regions and agro-ecological zones of Ethiopia and the disease poses considerable economic losses to cattle populations. Transmission commonly is by blood-feeding arthropods and direct contact is considered to be relatively ineffective. Although vaccination with KSGP is a realistic approach to control the disease in endemic countries, but several reasons were forwarded to defend the efficacy or effectiveness of KSGP vaccines. Hence, the occurrence of LSD after vaccination with KSGP strain will be suggestive of insufficient protection. Therefore, in order to come across these disagreements between these results, the following recommendations are forwarded:
- Detailed epidemiological investigations should be done to fully establish mode of LSD transmission;
- Full genome sequencing should be done to design a safe vaccines with good protection
- Further molecular characterization should be done on the existing vaccines;
- Vaccine efficacy should be measured in large-scale challenge studies;
- To create sufficient herd immunity, regular Vaccination campaigns should be implemented by effective and potent vaccine.
Ethical Statements
This article did not include animal experiments
Funding Sources
This article did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing Interests
The author declares that there is no conflict of interest regarding the publication of this article.
Additional Information
No additional information is available for this article.
Acknowledgements
The author highly acknowledges the National Veterinary Institute’s vaccine Sales Directorate Director Mr Mesfin Tadesse for his valuable information support.
References
-
Babiuk S, Bowden TR, Boyle DB, Wallace DB, Kitching RP (2008) Capripoxviruses: An emerging worldwide threat to sheep, goats and cattle. Transboundary and Emerging Diseases 55(7): 263-272.
-
Tuppurainen ESM, Venter EH, Shisler JL, Gari G, Mekonnen GA, et al. (2017) Review: Capripoxvirus Diseases: Current Status and Opportunities for Control. Transboundary and Emerging Diseases 64(3): 729-745.
-
Carn VM, Kitching RP (1995) An investigation of possible routes of transmission of lumpy skin disease virus (Neethling). Epidemiology and Infection 114(1): 219- 226.
-
Prozesky L, Barnard BJ (1982) A study of the pathology of lumpy skin disease in cattle. Onderstepoort Journal of Veterinary Research 49(3): 167-175.
-
Panel E (2015) Scientific Opinion on lumpy skin disease. EFSA Journal 13(1): 3986.
-
Ahmed WM, Zaher KS (2008) Observations on lumpy skin disease in local Egyptian cows with emphasis on its impact on ovarian function. AJMR 10(2): 252-257.
-
Mulatu E, Feyisa A (2018) Review: Lumpy Skin Disease. Journal of Veterinary Science & Technology 9(3): 1-8.
-
(2014) FAO, Emergence of lumpy skin disease in the Eastern Mediterranean Basin countries,” Empres watch, 30.
-
Abutarbush SM (2015) Lumpy Skin Disease. Jordanian Experiences With Control/Vaccination LSD Online meeting 17(3): 1268-1276.
-
Chihota CM, Rennie LF, Kitching RP, Mellor PS (2001) Mechanical transmission of lumpy skin disease virus by Aedes aegypti (Diptera: Culicidae). Epidemiology and Infection 126(2): 317-321.
-
Mebratu GY, Kassa B, Fikre Y, Berhanu B (1984) Observation on the outbreak of lumpy skin disease in Ethiopia. Revue delevage et de medecine veterinaire des pays tropicaux 37(4): 395-399.
-
Gari G, Waret Szkuta A, Grosbois V, Jacquiet P, Roger F (2010) Risk factors associated with observed clinical lumpy skin disease in Ethiopia. Epidemiology and Infection 138(11): 1657-1666.
-
Molla W, de Jong MCM, Frankena K (2017) Temporal and spatial distribution of lumpy skin disease outbreaks in Ethiopia in the period 2000 to 2015. BMC Veterinary Research 13(1): 310.
-
(2018) CSA, The Federal Democratic Republic of Ethiopia Centeral Statistical Agency Agricultural Sample Survey 2017/18 (2010 E.C.): Report on area and production for major crops (private peasant holdings, Meher season),” Statistical Bulletin No. 584, 1: 57.
-
Kitching RPP (1986) The control of sheep and goat pox. Revue Scientifique et Technique de l’OIE 5(2): 503-511.
-
Ayelet G, Haftu R, Jemberie S, Belay A, Gelaye E, et al. (2014) Lumpy skin disease in cattle in central Ethiopia : outbreak investigation and isolation and molecular detection of lumpy skin disease virus. 33(1408): 1-23.
-
Tamam SM (2006) Isolation of Lumpy skin disease virus form naturally infected cattle previously vaccinated with live attenuated sheep poxvirus vaccine. Journal of Veterinary Medical Research 16(1): 27-31.
-
Brenner J, Bellaiche M, Gross E, Elad D, Oved Z, et al. (2009) Appearance of skin lesions in cattle populations vaccinated against lumpy skin disease: Statutory challenge. Vaccine27(10): 1500-1503.
-
Tuppurainen ESMM, Oura CAL (2012) Review: Lumpy Skin Disease: An Emerging Threat to Europe, the Middle East and Asia. Transboundary and Emerging Diseases 59(1): 40-48.
-
Davies FG (1982) Observations on the epidemiology of lumpy skin disease in Kenya. Journal of Hygiene 88(1): 95-102.
-
Al Salihi KA, Hassan IQ (2015) Lumpy Skin Disease in Iraq: Study of the Disease Emergence. Transboundary and Emerging Diseases 62(5): 457-462.
-
Alkhamis MA, VanderWaal K (2016) Spatial and temporal epidemiology of lumpy skin disease in the Middle East, 2012-2015. Frontiers in Veterinary Science 3: 19.
-
Babiuk S, Wallace DB, Smith SJ, Bowden TR, Dalman B, et al. (2009) Detection of Antibodies Against Capripoxviruses Using an Inactivated Sheeppox Virus ELISA. Transboundary and Emerging Diseases 56(4): 132-141.
-
Mangana Vougiouka O, Markoulatos P, Koptopoulos G, Nomikou K, Bakandritsos N, et al. (2000) Sheep poxvirus identification from clinical specimens by PCR, cell culture, immunofluorescence and agar gel immunoprecipitation assay. Molecular and Cellular Probes 14(5): 305-310.
-
Davies FG, Otema C (1981) Relationships of capripox viruses found in Kenya with two Middle Eastern strains and some orthopox viruses. Research in Veterinary Science 31(2): 253-255.
-
Tulman ER, Afonso CL, Z Lu, Zsak L, Kutish GF, et al. (2000) Genome of Lumpy Skin Disease Virus. 75(15): 122-7130.
-
Johnston JB, McFadden G (2003) Poxvirus Immunomodulatory Strategies: Current Perspectives. Journal of Virology 77(11): 6093-6100.
-
Kara PD, Afonso CL, Wallace DB, Kutish GF, Abolnik C, et al. (2003) Comparative sequence analysis of the South African vaccine strain and two virulent field isolates of Lumpy skin disease virus. Arch Virol 148(7): 1335-1356.
-
Goff Cle, Charles Euloge Lamien, Emna Fakhfakh, Amélie Chadeyras, Elexpeter AbaAdulugba, et al. (2009) Capripoxvirus G-protein-coupled chemokine receptor: A host-range gene suitable for virus animal origin discrimination. Journal of General Virology 90(8): 1967- 1977.
-
Woods JA (1988) Lumpy skin disease-A review Tropical Animal Health and Production, 20(1): 11-17.
-
Lalani AS, Jennefer Masters, Wei Zeng, John Barrett, Rajeet Pannu, et al. (1968) Use of Chemokine Receptors by Poxviruses. Science 286(5446): 1968- 1971.
-
Fleming SB, Haig DM, Nettleton P, Reid HW, McCaughan CA, et al. (2000) Sequence and Functional Analysis of a Homolog of Interleukin-10 Encoded by the Parapoxvirus Orf Virus. Virus Genes 21(1): 85-95.
-
Moss B (2013) Poxvirus DNA replication. Cold Spring Harbor Perspectives in Biology 5(9): 1-12.
-
Yang Z, Reynolds SE, Martens CA, Bruno DP, Porcella SF, et al. (2011) Expression Profiling of the Intermediate and Late Stages of Poxvirus Replication. Journal of Virology 85(19): 9899-9908.
-
Elhaig MM, Selim A, Mahmoud M (2017) Lumpy skin disease in cattle: Frequency of occurrence in a dairy farm and a preliminary assessment of its possible impact on Egyptian buffaloes. Onderstepoort Journal of Veterinary Research 84(1): 1-6.
-
Sprygin A, Pestova Y, Wallace DB, Tuppurainen E, Kononov AV (2019) Transmission of lumpy skin disease virus: A short review. Virus Research 269: 197637.
-
Capstick PB, Coackley W (1961) Protection of Cattle against Lumpy Skin Disease: I.-Trials with a Vaccine against Neethling Type Infection. Research in Veterinary Science 2(4): 362-368.
-
Young E, Basson PA, Weiss KE (1970) Experimental infection of game animals with lumpy skin disease virus (prototype strain Neethling). Onderstepoort Journal of Veterinary Research 37(2): 79-87.
-
Greth A, Gourreau JM, Vassart M, Nguyen Ba Vy, Wyers M, et al. (1992) Capripoxvirus disease in an Arabian oryx (Oryx leucoryx) from Saudi Arabia. Journal of wildlife diseases 28(2): 295-300.
-
Chihota CM, Rennie LF, Kitching RP, Mellor PS (2003) Attempted mechanical transmission of lumpy skin disease virus by biting insects. Medical and Veterinary Entomology 17(3): 294-300.
-
Tuppurainen E, Venter EH, Shisler JL, Gari G, Mekonnen GA, et al. (2017) Review : Capripoxvirus Diseases : Current Status and Opportunities for Control. Review : Capripoxvirus Diseases 64(3): 729-745.
-
Lubinga JC, Tuppurainen ESM, Stoltsz WH, Ebersohn K, Coetzer JAW, et al. (2013) Detection of lumpy skin disease virus in saliva of ticks fed on lumpy skin disease virus- infected cattle. Experimental and Applied Acarology 61(1): 129-138.
-
Irons PC, Tuppurainen ESM, Venter EH (2005) Excretion of lumpy skin disease virus in bull semen. Theriogenology 63(5): 1290-1297.
-
Annandale CH, Holm DE, Ebersohn K, Venter EH (2014) Seminal Transmission of Lumpy Skin Disease Virus in Heifers. Transboundary and Emerging Diseases 61(5): 443-448.
-
Davies FG (1991) Lumpy skin disease, an African capripox virus disease of cattle. British Veterinary Journal 147(6): 489-503.
-
Tageldin MH, Wallace DB, Gerdes GH, Putterill JF, Greyling RR, et al. (2014) Lumpy skin disease of cattle: An emerging problem in the Sultanate of Oman. Tropical Animal Health and Production 46(1): 241-246.
-
Ayelet G, Abate Y, Sisay T, Nigussie H, Gelaye E, et al. (2013) Lumpy skin disease: Preliminary vaccine efficacy assessment and overview on outbreak impact in dairy cattle at Debre Zeit, central Ethiopia. Antiviral Research 98(2): 261-265.
-
Molla W, Frankena K, Gari G, de Jong MCM (2017) Field study on the use of vaccination to control the occurrence of lumpy skin disease in Ethiopian cattle. Preventive Veterinary Medicine 147: 34-41.
-
(2010) OIE, lumpy skin disease. pp: 1-13.
-
Alemayehu G, Zewde G, Admassu B (2013) Risk assessments of lumpy skin diseases in Borena bull market chain and its implication for livelihoods and international trade. Tropical Animal Health and Production 45(5): 115-1159.
-
Rozstalnyy A, Aguanno R, Beltran alcrudo D (2017) Lumpy Skin Disease : Situation, surveillance and control activities in Turkey.
-
Tuppurainen ESMM, Venter EH, Coetzer JAWW (2005) The detection of lumpy skin disease virus in samples of experimentally infected cattle using different diagnostic techniques. Onderstepoort Journal of Veterinary Research 72(2): 153-164.
-
Soliman HMT, Abdelrahman KA (2008) Polymerase chain reaction for rapid diagnosis of a recent lumpy skin disease virus incursion to Egypt.
-
Gelaye E, Mach L, Kolodziejek J, Grabherr R, Loitsch A, et al. (2017) A novel HRM assay for the simultaneous detection and differentiation of eight poxviruses of medical and veterinary importance. Scientific Reports 7: 1-11.
-
Gelaye E, Lamien CE, R Silber, Tuppurainen ESM, Grabherr R, et al. (2013) Development of a Cost-Effective Method for Capripoxvirus Genotyping Using Snapback Primer and dsDNA Intercalating Dye. PLoS One 8(10):1- 10.
-
Bowden TR, Babiuk SL, Parkyn GR, Copps JS, Boyle DB (2008) Capripoxvirus tissue tropism and shedding : A quantitative study in experimentally infected sheep and goats. Virology 371(2): 380-393.
-
Al-Salihi K (2014) Lumpy Skin disease : Review of literature. Mirror of Research in Veterinary Sciences and Animals 3(3): 6-23.
-
Tuppurainen ESM (2013) Mechanical transmission of lumpy skin disease virus by Rhipicephalus appendiculatus male ticks. Epidemiology and Infection 141(2): 425-430.
-
Kitching RP, Mellor PS (1986) Insect transmission of capripoxvirus. Research in Veterinary Science 40(2): 255-258.
-
Hunter P, Wallace D (2001) Lumpy skin disease in Southern Africa: A review of the disease and aspects of control. Journal of the South African Veterinary Association 72(2): 68-71.
-
Lamien CE (2011) Use of the Capripoxvirus homologue of Vaccinia virus 30kDa RNA polymerase subunit (RPO30) gene as a novel diagnostic and genotyping target: Development of a classical PCR method to differentiate Goat poxvirus from Sheep poxvirus. Veterinary Microbiology 149(1): 30-39.
-
Vandenbussche F, Mathijs E, Haegeman A, Al-majali A, Van Borm S, et al. (2016) Complete Genome Sequence of Capripoxvirus Strain KSGP 0240 from a Commercial Live Attenuated Vaccine 4(5): e01114-16.
-
Salib FA, Osman AH (2011) Incidence of lumpy skin disease among Egyptian cattle in Giza Governorate, Egypt. Veterinary World 4(4): 162-167.
-
Abdallah FM, El Damaty HM, Kotb GF (2018) Sporadic cases of lumpy skin disease among cattle in Sharkia province, Egypt: Genetic characterization of lumpy skin disease virus isolates and pathological findings. Veterinary World 11(8): 1150-1158.
-
Davies FG, Mbugwa G (1985) The alterations in pathogenicity and immunogenicity of a Kenya sheep and goat pox virus on serial passage in bovine foetal muscle cell cultures. Journal of Comparative Pathology 95(4): 565-572.
-
Tuppurainen ESMM (2014) Characterization of sheep pox virus vaccine for cattle against lumpy skin disease virus. Antiviral Research 109(1): 1-6.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions