Recent Trends in Dengue Virus Infection; An Analysis of Virological, Clinical and Laboratory Profiles of Patients with Dengue Virus Infection in the Center for Clinical Management of Dengue Fever and Dengue Hemorrhagic Fever, Sri-Lanka
Background: Dengue is hyper-endemic with outbreaks around the country. Clinical presentation is influenced by presence of previous exposures to infection and circulating serotype. Changes in circulating serotype, frequently lead to outbreaks as well. Early identification of changes in circulating serotypes and clinical pattern is invaluable for outbreak prediction, control and efficient patient management. Objectives: Study aimed to describe demographic, clinical and laboratory parameters of dengue patients during the interepidemic period in Sri-Lanka, and to identify circulating serotypes and their association with clinical/laboratory parameters to understand future occurrence of dengue. Study design: Laboratory based cross-sectional study was conducted at National Arbovirus Diagnostic Laboratory, including 129 plasma samples tested positive by Dengue serotyping real-time PCR. All samples were also tested for secondary dengue. Results: Mean age was 20.8years and 41.8% belonged to 6-15years. Primary infection was noted in 56.9%.Majority had platelet <50,000/ uL, leucopenia, ALT and AST above the upper limit of the normal (38.7%, 58.1%, 55, 8% and 71.3% respectively). DENV2 was 45.7% and DENV3 was 27.1%. Severe dengue was seen in 48.1% in DENV3 cases. Majority with DENV2 had platelets < 50,000/uL (68.8%). Leucopenia (82.6%) was higher in DENV3. Primary and secondary infection for DENV2 was 43.9%&54.8%. For DENV3 primary infections (22%) were higher than secondary infections (19.4%). Conclusion: Primary non-severe dengue cases of were predominant. Principal circulating serotype was DENV2 with cocirculation of DENV3 and1.DENV2 was more frequently associated with secondary-infection, thrombocytopenia and elevated AST while DENV3 was mostly associated with primary-infection, severe dengue, leucopenia and elevated ALT.
Introduction
Dengue is one of the most evolving arbovirus infections in the world leading to significant health burden in tropical and subtropical countries. It is endemic in many of the WHO regions such as South East Asia, the Americas, the Western Pacific, Africa and Eastern Mediterranean regions and it is estimated that around 3.9 billion people are at risk of getting the infection with more than 70% of them living in Asian countries including Sri-Lanka [1, 2, 3].
The infection is due Dengue virus, a single stranded RNA virus belonging to the family Flaviviridae and is primarily transmitted by female Aedes mosquitoes; Aedesaegypti, which are prevalent in these tropical and subtropical areas.
The virus has four serotypes (DENV 1-4) which are genetically diverse but similar by about 60- 75% at amino acid level thus giving rise to the unique clinical and immunological picture in dengue [1]. Primary infection with one serotype confers lifelong homotypic immunity to the infecting serotype while providing short lived heterotypic protection to other serotypes. Therefore breakthrough infections by a different serotype (secondary dengue infection) can give rise to severe forms of dengue infection [4]. Moreover, several serotypes may co-circulate during an epidemic, thus increasing the health risks.
Clinical manifestations of the infection are diverse and may range from asymptomatic infection to severe forms such as dengue hemorrhagic fever, dengue shock syndrome or death. Many factors have been identified as prognostic markers predicting the severity of the disease such as low platelet count, improper fluid management, etc [5, 6, 7, 8]. Diagnosis of the infection is mainly clinical and may be supported by virological tests such as NS1 antigen testing, dengue specific antibody detection, dengue genome detection. There is no specific treatment for dengue and is predominantly based on fluid management and symptomatic therapy with analgesics and antipyretics.
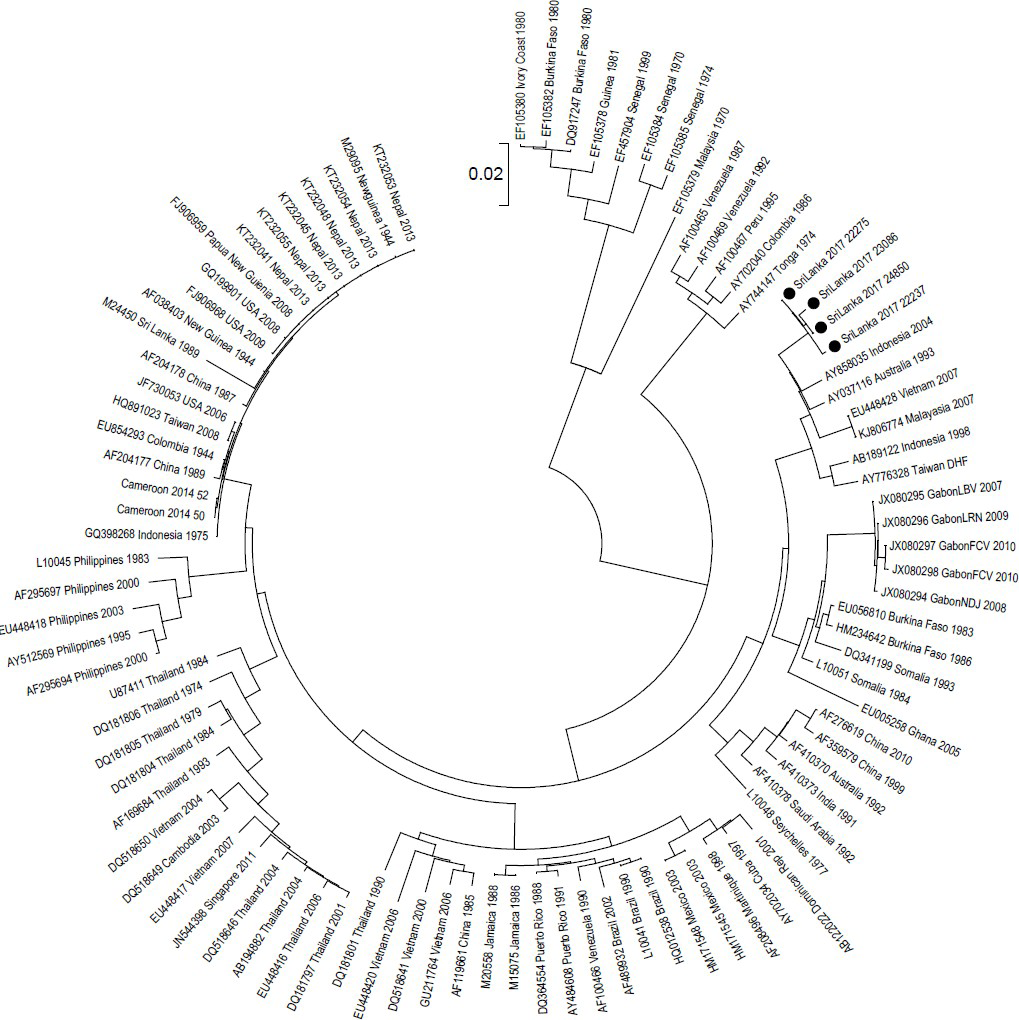
Sri-Lanka is hyper endemic for dengue virus infection and epidemics of dengue had been reported in the country for more than three decades. The first serologically confirmed case of Dengue occurred in 1962 following which the case burden rose dramatically over time [9]. All four serotypes of Dengue had been co-circulating in the country with time to time predominance of one or two serotypes. Dengue 1 and 2 had been predominant in 1960s, while DENV 3 & 4 were responsible for the outbreaks from 1970s to early 2000 followed by resurgence of DENV 1 in 2006-2010 and DENV 2 in 2017 epidemics [10, 11, 12]. The Dengue outbreak in 2017 due to DENV 2 was one of the largest outbreaks in the country and figure 1 depicts the phylogenetic analysis of the circulating viruses during the period. Various Scio-economic and cultural changes that occurred in Sri Lanka over time largely contributed to the spread of the vector and the virus throughout the country. Moreover, climatic changes also had a significant impact on dengue in Sri Lanka. Although, dengue cases are being reported year around throughout the country two main peaks are identifiable from October to December and from May to July.
A multitude of factors such as the infecting virus type, shifts in circulating serotypes, host immunity, vector, environment changes and accessibility to healthcare facilities play an important role in deciding the clinical outcome of dengue and occurrence of epidemics. Also the non-specific nature of the infection and lack of specific therapeutic measures makes it is important to have a high index of suspicion to identify clinical cases early and undertake necessary treatment. At the same time the circulating serotype has a significant impact on the severity of the disease due to the unique pathogenicity the virus has. Hence identification of changing serotypes over the time is important in predicting the severity and impact during epidemics.
Objectives
Therefore, the current study was formulated to describe the demographic, clinical and laboratory parameters of dengue infected patients during the inter-epidemic period in Sri Lanka, identify the circulating dengue serotypes and their association with clinical and laboratory parameters with the intent of predicting the future occurrence and severity of dengue in Sri Lanka.
Study Design
This laboratory based retrospective descriptive study was conducted at the National Arbovirus testing laboratory at the Medical Research Institute which is the premier laboratory for the diagnosis of dengue virus infection in the country. All blood/plasma samples sent from the Center for Clinical Management of Dengue Fever and Dengue Hemorrhagic Fever, Negambo, Sri-Lanka from December 2018 to February 2019) and tested positive by dengue serotyping real time PCR were included in the study. The Center for Clinical Management of Dengue Fever and Dengue Hemorrhagic Fever, Negambo, Sri-Lanka is one of two centers for the management of dengue virus infection of all age groups from all around the country. Clinical and laboratory details were collected using hospital records and the accompanying request form.
Samples tested positive for dengue virus by sero-typing real time PCR were also tested for the presence of secondary infection using the Panbio dengue IgG capture ELISA which only detect dengue IgG titers compatible with secondary dengue infection. Extraction of viral RNA (from 140µl of plasma) was carried out using the QIAmp® viral RNA mini kit by QIAGEN Germany and the extraction was carried out as per the manufacturer’s instructions. An additional centrifugation step was performed to remove any remaining ethanol and elutes were subjected to PCR assay without delay.
Dengue virus RNA detection and serotyping was done using the commercially validated Real Star® Dengue Type RT-PCR kit 1.0 according to manufacturer’s instructions using the Rotor-Gene Q 5plex real time PCR instrument. The kit detected all four dengue serotypes and had been in use for clinical diagnostics followed by verification within the laboratory for several years.
Commercially validated Panbio Dengue IgG capture ELISA kit by Abbott, USA, which detects dengue IgG of more than 2560 HAI titer, was used for the detection of secondary dengue infection. Secondary infection is characterized by high levels of specific IgG (> 2560 HAI titre) 1-2 days after the onset of infection. As per manufacture’s manual the serological sensitivity for secondary infection was 85.7% and serological specificity for primary infection was 93.3%. Serological specificity for seronegative samples was 100%.
Data analysis was conducted using the latest version of SPSS. Categorical variables were presented as frequencies/ percentages and chi-square or Fisher’s Exact Test was adopted to analyze the significance between categorical variables. The analyses were performed at 95% confidence with level of significance of p<0.05.
Results
A total of 129 Dengue real-time PCR positive patients were identified during the study period and their demographic, clinical and laboratory parameters are depicted in Table 1.
| Variable | Result (%) |
|---|---|
| Age range, mean (SD) | 4 months-96 years, 20.8years |
| (n=129) | -17.9 |
| Age breakdown | |
| < 5 years | 16 (12.4) |
| 6-15 years | 54 (41.8) |
| 16-25 years | 17 (13.2) |
| 26-35 years | 19 (14.7) |
| 36-45 years | 10 (7.8) |
| 46-55 years | 8 (6.2) |
| 56-65 years | 0 |
| 66-75 | 1 |
| 76-85 | 1 |
| 86-95 | 0 |
| 96-105 | 2 |
| No data | 1 |
| Gender (n=129) | |
| Female | 53 (41%) |
| Male | 53 (41%) |
| Data not available | 23 |
| Dengue category (n=129) | |
| Non severe Dengue | 72 (55.8%) |
| Severe Dengue | 41 |
| Deaths | 0 |
| Data not available | 16 |
| Infection Status (n=72) | |
| Primary | 41 (56.9%) |
| Secondary | 31 (43.1%) |
| Laboratory parameters | |
| Platelets (x 103/uL) n=129 | |
| Range, Mean | 4 – 220, 56 |
| < 50 | 50 (38.7%) |
| 51 – 100 | 22 |
| 101 – 150 | 12 |
| > 150 | 7 |
| Data not available | 38 |
| WBC count (x 103/uL)) n=129 | |
| Range, Mean | 1.12 – 9.8, 3.11 |
| Leucopenia | 75 (58.1%) |
| Normal count | 23 |
| Data not available | 31 |
| ALT (IU/mL) n=129 | |
| Range, Mean | 9 – 994, 129 |
| Normal | 31 |
| >ULN | 72 (55,8%) |
| Data not available | 26 |
| AST (IU/mL) n=129 | |
| Range, Mean (SD) | 13 – 2156, 224 |
| Normal | 11 |
| >ULN | 92 (71.3%) |
| Data not available | 26 |
Table 1: Demographic, clinical and laboratory parameters of study subjects.
Demographic, Clinical and Laboratory Parameters of the Study Subjects
The age of the subjects ranged from 4 months to 96 years and the mean age was 20.8 years with majority (41.8%) being within 6-15 year age category. Twelve point four percent were less than 5 years of age and 35.7% were within 16-45 years. Both males and females were present in similar percentages (41%) among the study subjects. Out of the 129 patients, 55.8% had non severe dengue during the study period and no deaths were reported. Moreover, primary infections were more common than secondary infections (56.9% vs 43.1%).
With regard to laboratory parameters platelet count ranged from 4 x 103/µL to 220 x 103/µL (mean – 56 x 103/ µL), WBC count from 1.12 x 103/µL to 9.8 x 103/µL (mean 3.11 x 103/µL), ALT from 9 IU/mL to 994 IU/mL (mean 129 IU/mL) and AST from 13 to 2156 IU/mL (mean 224.7 IU/ mL). Majority had a platelet count < 50,000 /µL, leucopenia, ALT and AST levels more than the upper limit of the normal (38.7%, 58.1%, 55, 8% and 71.3% respectively).
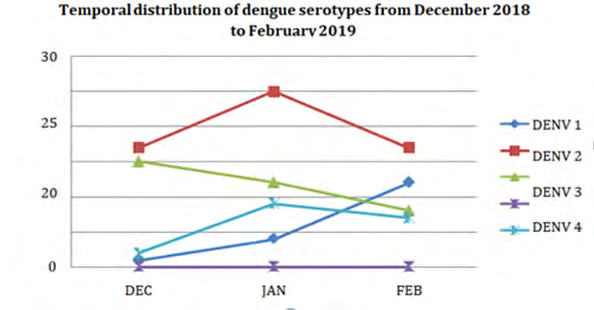
Identified Dengue Serotypes and their Temporal Distribution during the Study Period
DENV 2 was the predominant serotype identified with DENV 3 being the second commonest serotype. Fourteen percent of the subjects were infected with two serotypes and (Table 2) expresses the serotype distribution in the study population.
| Dengue Virus Type | No. (n = 129) | Percentage | |
|---|---|---|---|
| DENV 1 | 17 | 13.20% | |
| DENV 2 | 59 | 45.70% | |
| DENV 3 | 35 | 27.10% | |
| Dual* | 18 | 14.00% | |
| Total | 129 | 100.00% | |
| Variable | DENV 1 against other serotypes ( %, P value) | DENV 2 against other serotypes ( %, P value) | DENV 3 against other serotypes ( %, P value) |
| Median Age | 14years (n=17) | 26.9 years (n=58) | 14 yrs (n=35) |
| Dengue category Non severe Dengue | 82.40% | 58.90% | 51.90% |
| Severe Dengue | 17.60% | 41.10% | 48.10% |
| Laboratory parameters | |||
| Platelets< 50,000/µL | 40% | 68.80% | 63%, 0.7 |
| Luecopenia | 80% | 81.80% | 82.6%, 0.774 |
| ALT >ULN | 46.60% | 75% | 81.5%, 0.127 |
| AST > ULN | 86.60% | 93.10% | 85.2%, 0.418 |
Table 2: Dengue serotypes identified in the study population. *Comprised of 1&3, 1&2 and 2&3 DENV 2 was the most commonly identif
Association of Dengue Serotype with Demographic, Clinical and Laboratory Parameters
Table 3 & 4 describes the association of dengue serotypes with demographic, clinical, and laboratory parameters and infection status respectively. The mean age for DENV 1 and 3 were 14 years while for DENV 2 was 26.9 years. Non severe dengue was mostly seen in patients with DENV 1 infection (82.4%) and severe dengue was seen predominantly in DENV 3 infection (48.1%). Moreover, DENV 2 had the highest patient percentage for platelets less than 50,000 /µL (68.8%) and elevated AST (93.1%) while DENV 3 had most patients with leucopenia (82.6%) and elevated ALT (81.5%). None of the assessed parameters were significantly associated with any one of the DENV serotypes circulating during the study period.
Both primary and secondary infections were highest with DENV 2 (43.9% and 54.8% respectively). Moreover, for DENV 2 and 1 secondary infection rate was more than the primary infection rate while for DENV 3 rate of primary infections (22%) were higher than secondary infections (19.4%).
| Variable | Primary (%) | Secondary (%) | P value |
|---|---|---|---|
| DENV 1 | 14.6 | 25.8 | 0.23 |
| DENV 2 | 43.9 | 54.8 | 0.36 |
| DENV 3 | 22 | 19.4 | 0.78 |
Table 3: Association of Dengue serotype with infection status.
Discussion
The present study aimed at describing the demographic, clinical and laboratory parameters of patients presenting with Dengue virus infection during the inter epidemic season in Sri-Lanka and to identify the circulating Dengue serotypes and their association with the clinical presentation in order to predict the occurrence and severity of the upcoming dengue season.
In the current study, more than 75% of the infected patients were aged less than 45 years with majority being within the 6-15 year age group, which is in agreement with the characteristic age distribution seen during 2017 outbreak; one of the largest dengue outbreaks in Sri Lanka, as well as in several other previous Sri Lankan studies [13, 14, 15, 16]. At the same time globally also, frequently affected belonged to a similar age category, because they spend a significant time in public places due to work and education which make them more susceptible to be in contact with the principal vector [17, 18].
Both females and males were equally affected in the current study and the gender distribution of dengue in Sri Lanka was variable in previous studies conducted in the country as well. While some local and international studies reported that females were more frequently affected [15, 19] some others reported that males were the predominantly affected gender [16, 20, 21, 22]. Engagement of males and females in various outdoor activities due to various social and cultural reasons mainly affects the distribution and the relatively small sample size in the current study also may have had an impact on the generated value.
Clinical characteristics of the study subjects showed that majority of patients were belonging to non-severe dengue category but, had platelets less than 50,000/µL, leucopenia, elevated ALT and AST. Median AST level was more than ALT and increment of AST was observed more frequently than ALT which is a characteristic finding seen with hepatic involvement in dengue. All of these parameters closely agreed with local and international studies elsewhere [15, 16].
Furthermore, majority of the patients had primary dengue infection which usually is associated with less severe clinical presentation while the rate of secondary infections also followed closely. Local dengue sero-prevalence data is limited and one study demonstrated that the sero- prevalence was low in very young children and it gradually increased with age [23]. The pattern of age distribution in the current study, where a significant proportion was children may have had an impact on the primary infection rate.
When considering the circulating dengue serotype, all serotypes except DENV-4 were reported during the period with the predominant being DENV-2, coinciding with the hyper-endemic nature of the infection in Sri-Lanka. At the same time, it can be presumed that following it’s resurgence in 2017 DENV-2 is still circulating as the prominent serotype in Sri Lanka [12, 13].
On the other hand, DENV-1 and 3 were also circulating in significant percentages (13.2% and 27.1% respectively) with DENV 3 being higher in December to January and DENV-1 in February. At the same time it is evident that DENV 3 was more frequently associated with primary infection while DENV 1 and 2 were more associated with secondary infection keeping in line with the fact that DENV-3 had not been reported as a prominent serotype since 2004 [11]. However, none of the serotypes showed a significant association with either primary or secondary infection. These findings highlight concern whether DENV 3 can become predominant as time goes, thus paving way to another outbreak as a result of the shift in circulating serotypes.
Analysis of association of dengue serotypes with mean age of the study subjects revealed that while DENV 2 was infecting mainly adults (mean age 26 years), children were predominantly infected with DENV 1 and 3 (mean age 14 years), further confirming the data acquired for circulating serotypes over time and the rates obtained for infection status with each serotype.
With regard to association of serotypes with clinical and laboratory parameters, DENV 2 was associated with more frequent episodes of thrombocytopenia less than 50,000/µL and elevated AST, but other parameters such as severe dengue, leucopenia and high ALT were mainly associated with DENV 3. Parameters observed in the current study is comparable to studies elsewhere though none of the parameters in the present study showed a significant association. It is said that DENV 2 is associated with more severe infection by several studies [17, 18]. More so, DENV 3 is also associated with severe presentations of dengue according to a meta-analysis carried out in 2016 to analyze severity of dengue infection by different serotypes in primary and secondary infections reported that in south-east Asian region which stated that primary infections with DENV 3 was more severe and secondary infections with DENV-2, DENV-3 and DENV-4 was also more severe [24].
Considering the above factors, it is evident that in Sri Lanka during this inter epidemic period, the predominant circulating serotype is DENV-2 with co-circulation of DENV 3 and 1, thus can be predicted that severe forms of dengue would continue to be reported in the country during the upcoming season. On the other hand, both the DENV 3 and 1 show a probability of rising in numbers and may replace DENV-2. DENV 3 had not been reported in the country for some time leading to an immune naïve population who can contribute to increase spread of infection changing the predominant serotype, thus leading to an outbreak situation with severe cases.
Conclusion
Majority of the infected were children and young adults with cases of non-severe dengue being predominant. Majority had primary dengue infection. The predominant circulating serotype was DENV 2 with co-circulation of Dengue 3 and 1. DENV 2 was associated with more frequent episodes of secondary infection, thrombocytopenia and elevated AST while DENV 3 was mainly associated with primary infection, severe dengue, and leucopenia and elevated ALT.
References
-
Guzman MG, Harris E (2015) Dengue. Lancet 385(9966): 453-465.
-
Bhatt S, Gething PW, Brady OJ, Messina JP, Farlow AW, et al. (2013) The global distribution and burden of dengue. Nature 496(7446): 504-507.
-
Brady OJ, Gething PW, Bhatt S, Messina JP, Brownstein JS, et al. (2012) Refining the global spatial limits of dengue virus transmission by evidence-based consensus. PLoS Negl Trop Dis 6(8): e1760.
-
Halstead S (2019) Recent advances in understanding dengue. F1000Research 8: 1279.
-
Chuansumrit A, Puripokai C, Butthep P, Wongtiraporn W, Sasanakul W, et al. (2010) Laboratory predictors of dengue shock syndrome during the febrile stage. Southeast Asian J Trop Med Public Health 41(2): 326- 332.
-
Sutaryo (2004) Dengue. Medical Fakultas Kedokteran UGM, Yogyakarta.
-
Tantracheewathorn T, Tantracheewathorn S (2007) Risk factors of Dengue shock syndrome in children. J Med Assoc Thai 90(2): 272-277.
-
Kalayanarooj S, Nimmannitya S (2005) Is dengue severity related to nutritional status? Southeast Asian J Trop Med Public Health 36(2): 378-384.
-
Vitarana T, Jayakuru WS, Withane N (1997) Historical account of dengue haemorrhagic fever in Sri Lanka. WHO/SEARO Dengue Bulletin 21: 117-118.
-
Kulatilaka TA, Jayakuru WS (1998) Control of Dengue/ Dengue Haemorragic fever in Sri Lanka. Dengue Bulletin 22: 1-9.
-
Kanakaratne N, Wahala WM, Messer WB, Tissera HA, Shahani A, et al. (2009) Severe dengue epidemics in Sri Lanka 2003–2006. Emerg Infect Dis 15(2): 192-199.
-
Alia S, Khanb AW, Robinson AWT, Adnand M, Malik S, et al. (2018) The unprecedented magnitude of the 2017 dengue outbreak in Sri Lanka provides lessons for future mosquito-borne infection control and prevention. Infection, Disease & Health 23(2): 114-120.
-
Jayarajah U, Faizer S, De Zoysa IM, Seneviratne SL (2017) A Large Dengue Epidemic Affects Sri Lanka In 2017. International Journal of Progressive Sciences and Technologies (IJPSAT) 6(1): 84-86.
-
Udayanga L, Gunathilaka N, Iqbal MCM, Lakmal K, Amarasinghe US, et al. Comprehensive evaluation of demographic, socio-economic and other associated risk factors affecting the occurrence of dengue incidence among Colombo and Kandy Districts of Sri Lanka: a cross-sectionalstudy. Parasit Vectors 11(1): 478.
-
Ferede G, Tiruneh M, Abate E, Wondimeneh Y, Gadisa E, et al. (2018) A study of clinical, hematological, and biochemical profiles of patients with dengue viral infections in Northwest Ethiopia: implications for patient management. BMC Infect Dis 18: 616.
-
Kularatne SA, Gawarammana IB, Kumarasiri PR (2005) Epidemiology, clinical features, laboratory investigations and early diagnosis of dengue fever in adults: a descriptive study in Sri Lanka. Southeast Asian J Trop Med Public Health 36(3): 686-692.
-
Messer WB, Kanakaratne N, Thevanesam V, Ranawaka G, Shahani A, et al. (2012) Clinical features of hospitalized dengue patients in Sri Lanka from 2004 to 2006. Srilanka Journal of Infectious Diseases 2(1): 9-18.
-
Suppiah J, Ching SM, Amin-Nordin S, Mat-Nor LA, Ahmad- Najimudin NA, et al. (2018) Clinical manifestations of dengue in relation to dengue serotype and genotype in Malaysia: A retrospective observational study. PLoS Negl Trop Dis 12(9): e0006817.
-
Vicente CR, Herbinger KH, Fröschl G, Malta Romano C, de Souza Areias Cabidelle A, et al. (2016) Serotype influences on dengue severity: a cross-sectional study on 485 confirmed dengue cases in Vitória. BMC Infect Dis 16: 320.
-
Bosmasang E, Suzara-Masage EC (2008) Clinical and laboratory features of the dengue virus serotypes among infected adults in Cardinal Santos Medical Center. Philippine Journal of Microbiology and Infectious Diseases 37(2): 5-14.
-
Garg A, Garge J, Rao YK, Upadhyay GC, Sakhuja S, et al. (2011) Prevalence of dengue among clinically suspected febrile episodes at a teaching hospital in north India. J Infect Dis Immun 3(5): 85-89.
-
Anker M, Arima Y (2011) Male-female differences in the number of reported incident dengue fever cases in six Asian countries. Western Pac Surveill Response J 2(2): 17-23.
-
Verhagen LM, de Groot R (2014) Dengue in children. J Infect 69(1): 77-86.
-
Soo KM, Khalid B, Ching SM, Chee HY (2016) Meta- Analysis of Dengue Severity during Infection by Different Dengue Virus Serotypes in Primary and Secondary Infections. PLoS One 11(5): e0154760.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions