Evaluation of Antibody Response in COVID-19 Recovered Population of Swat Kp, Pakistan
A novel coronavirus disease now known as the Coronavirus disease 2019 (COVID-19) is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). It poses a huge challenge to the society, economy, and public health worldwide. At present, the antibody responses to SARS-CoV-2 remain largely unknown especially in remote regions of developing countries. The objective of the study was to evaluate the antibody response in COVID-19 recovered patients and vaccinated individuals of district Swat. COBAS-511 machine was used for quantitative detection of COVID-19 antibodies in 3 cc venous blood collected from selected patients and was stored in collection tubes followed by subsequent centrifugation to separate the serum. Further to ensure the variable factors does not affect the accuracy of the study, 95 questionnaires were distributed where the participants were asked to disclose basic information (name, age, gender, address, area, COVID-19 test, vaccinated or nonvaccinated, signs and symptoms, antibiotics/antivirals used during the infection time) since it is important to confirm patients' health status and to clearly determine whether they can donate plasma. Participant’s age ranging from 15 to 63 were involved in these studies. As per findings of this study, people aged 45 to 55 years had high levels of antibodies against COVID-19. In age wise antibody response level women were found to have higher antibody levels than men. Among the variable factors, the most common pre-complications were heart disease and diabetes, such individuals had higher levels of anti-COVID-19 antibodies than those with no prior health complications. The level of antibodies was significantly higher in patients that received anti-COVID-19 vaccines post recovery as compared to those that did not receive vaccine. However further study will be required to validate these preliminary observations.
Introduction
In December 2019, a coronavirus (CoV) hit the city of Wuhan, China and was declared a public health emergency. Later, this virus was identified as a novel coronavirus-2019 (2019nCoV), and the disease caused is known as Coronavirus disease-2019 (COVID-19). It is now known as severe acute respiratory syndrome coronavirus-2 (SARS-COV-2). This virus is responsible for severe human respiratory diseases and has resulted in a pandemic with more than 274,029,005 human infections and 5,362,728 deaths according to WHO reports. Human to Human transmission is very rapid with fatality rate of ~2-3.5% and till date no proper treatment is available to cope it [1]. The mortality rate for hospitalized patients ranged between 11% and 15% [2].
The SARS-COV-2 genome contains four structural proteins (including spike (S) and Nucleocapsid (N)), eight accessory proteins and fifteen nonstructural proteins. ACE2 membrane receptors, located on the surface of the host cell, are recognized by the S protein’s receptor binding domain (RBD). The N protein is a structurally helical nucleocapsid protein of the virus that plays a key role in transcription, viral replication, and packaging.
This virus mainly causes high fever, cough, sore throat, fatigue, rhinorrhea, and dyspnea. These symptoms differ from general pneumonia in that they are not specific. Those infected with SARS-CoV-2 suffer from neurological symptoms [3] for example insomnia, myalgia, and dizziness. Some patients also experienced digestive symptoms, including diarrhea. There are few asymptomatic patients, and most patients present with nonspecific symptoms upon admission. SARS-CoV-2 infected pregnant women had similar symptoms to adult patients, and a third of their neonates were infected with the virus. SARS-CoV-2 is transmitted by close contact, droplets from infected person. For coronavirus infection, no specific treatment has been approved.
This disease can be controlled through source control, personal protection, and early diagnosis, isolation, and supportive treatment. Moreover, there is no antiviral treatment available for SARS or MERS that has been shown to be effective.
The recurrence of positive COVID-19 results may be linked to a patient’s immunity since a decrease in immunity could easily result in an emergence of viral load within the body and recurrence of illness. An early COVID-19 study showed positive immunoglobulin M (IgM) and immunoglobulin G (IgG) levels in the blood of 16 patients with COVID-19 paces of half (8/16) and 81% (13/16) on Day 10 of disease and paces of 81% (13/16) and 100% (8/16) on Day 15, individually [4]. The antiSARS-CoV IgG antibodies in humans may last up to 12 years according to another SARS study [5]. It is possible for patients who recover from SARS- CoV-2 to carry protective antibodies and suppress the virus for a long time, but this does not guarantee that the patient will not relapse with it in the future [6]. In patients who died from viral pneumonia, there were significant reductions in CD3+, CD3+ CD4+, and CD3+ CD8+ T cell absolute counts. Therefore, decreased cellular immunity can result in disease, which may be linked to reactivation of nucleic acids following discharge. There are significant interferences in the evaluation of therapeutic antibodies and vaccines aimed at combating COVID-19. The cross-reactivity of anti-SARS-CoV antibodies with the COVID-19 spike protein was evaluated due to the high identity of SARS-CoV’s receptor binding domain (RBD) and SARS-CoV-2. Antibodies are neutralized mainly by the spike protein. A human monoclonal antibody specific for SARS-CoV, CR3022, fixes strongly with the COVID-19 RBD.
Several vaccines are now available. In early December 2020, a mass vaccination program started. Thirteen vaccines have been administered (across four platforms). COVID-19 vaccines provide protection against the disease, to develop an immunity against the SARS-COV-2. Vaccination reduces the risk of contracting an illness and its consequences. The virus is less likely to cause illness if you have this immunity. It’s also helpful to get vaccinated to protect others, since vaccinating prevents you from becoming infected and from contracting diseases, which means you are less likely to pass on infection to other people. COVID-19 infection can cause serious illness in high-risk individuals, for example those with other medical conditions, older adults, and healthcare providers. Vaccines for SARS-CoV-2 are now widely available which are safe, effective and reduce the risk of illness.
A serological test known as the ELISA / CLIA tests blood samples for antibodies to the SARSCoV-2. This test provides reliable information about two values: IgG type antibodies (past infection) and IgM type antibodies (acute infection). Today, this is the most reliable method of determining whether antibodies have been made against COVID-19. If IgG antibodies are present, then it proves that the patient has had the disease in the past.
In laboratories, antibody detection is done by lateral flow, ELISA, or chemiluminescent immunoassay (CIA), which may require skilled workers and specialized equipment for some assays. In addition, IgG and IgM can be detected separately, or as a total antibody (Ig). Some tests detect antibodies against both immunodominant proteins (multiplex assays), while others detect antibodies against either S or N proteins.
Importance of the study is to evaluate the antibodies response in the COVID-19 recovered patients by measuring the quantity of antibodies in their blood/ plasma and to check durability/ stability of antibodies produced for their use in plasma therapy. This is important to check the health status of recovered patients and to see if the person is suitable for plasma donation. To evaluate the antibodies response in the COVID-19 recovered patients in District Swat. To determine the factors that are linked with COVID-19 in local population of District Swat.
Materials and Methods
Study Design
This current study was carried out in district Swat, Khyber Pakhtunkhwa, Pakistan. It has a total area of 5337 sq.kms and a population of 2.3 million, including 50.8%
males and 49.2% females. The study was designed to include patients from all different regions of district Swat. The study included COVID-19 recovered patients discharged from the central hospital Saidu Sharif, Swat. Study included COVID-19 patients who recovered within last 6 months of the study and vaccinated individuals. Individuals from different walks of life (university and college students, laboratory, operators, professors, labors) were included in the study to ensure randomization of the data. Samples were collected from both (male and female) with age range from 15 to 63. A total of 95 questionnaires were distributed among the participants to ensure proper randomization and asses different variables (age, gender, and any other previous medical conditions) that might affect the outcome of the study. Written and verbal consent were taken from all the participants and their information were kept secret. Study was evaluated by the ethical review committee of University of Swat.
COVID-19 Antibody Quantification
Quantitative detection of COVID-19 antibodies was done by using COBAS-511 machine. The blood was stored in gel tubes before being centrifuged at 4000rpm for 3 minutes, the serum was isolated was run in COBAS-511 (Roche Diagnostics) according to the manufacturer’s instructions. The cut off values of less than 1U/ml is taken as non-reactive for antibodies while the value above 1.2U/ml is considered reactive for antibodies. The higher value for antibodies represents the strong immune response.
Data collection
Samples were taken by two methods as per directions of international Pathologist following WHO protocols, which are Nasopharyngeal swab and Oropharyngeal swab. Nasopharyngeal swabs samples were 92 whereas only 3 samples were collected using Oropharyngeal swabs. 3 cc of venous blood from COVID-19 recovered patients were taken to compare the antibodies levels based on age, gender, BCG and non-BCG vaccinated individuals, and individuals vaccinated for SARS-CoV-2.
Statistical analysis
Collected data was analyzed using SPSS Software (version 16.0). Pie charts and bar charts were made using MS office Excel software for graphical representation of the study outcomes.
Results
Antibodies response comparisons
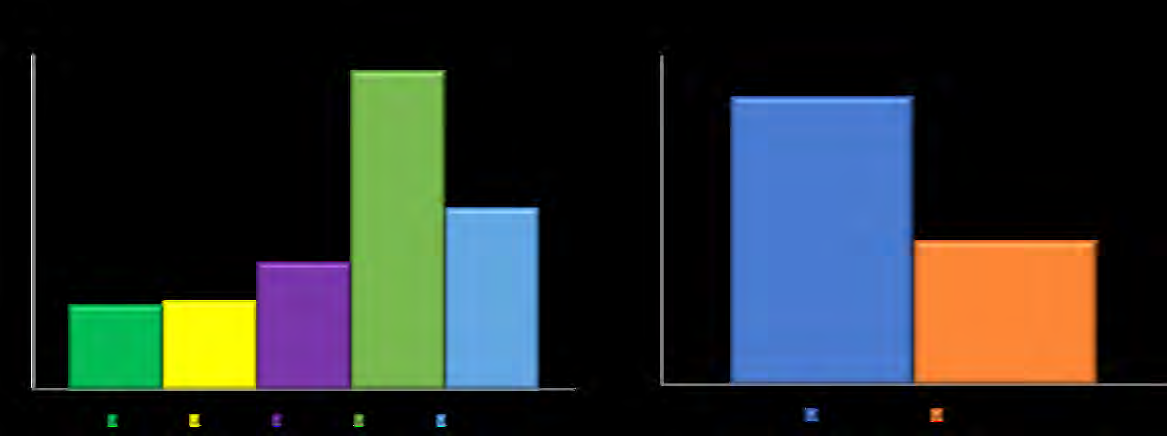
Age/gender wise antibodies response in COVID-19 recovered patients: The antibodies response of participants was almost similar in age group 15-25 (22.54%) and 26- 35 (23.39%) years and lowest in comparison to other age groups. However, in age group of 36-45 (33.92%) years the antibody response was slightly higher as compared to the first two groups. Participants in age group 45-55 (85.26%) years had the highest antibodies response to COVID-19 followed by age group above 55 years with around 48.55%. The age wise antibody response is presented in (Figure 1a). The gender wise antibodies response was higher in female (52.42%) than male (26.07%). The gender wise antibodies response is presented in (Figure 1b).
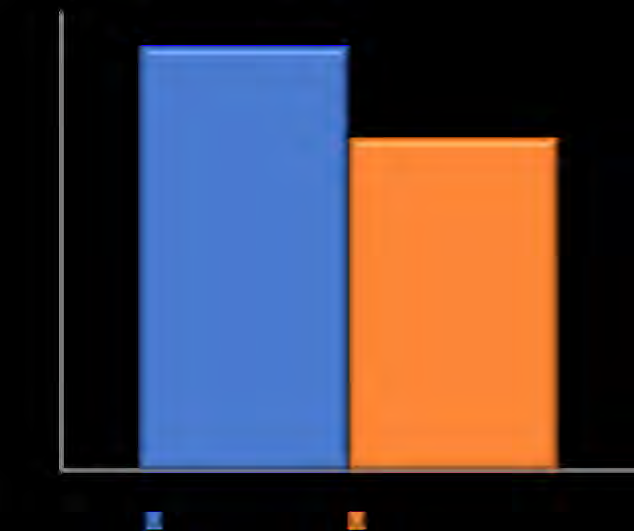
Antibodies response in vaccinated and non-vaccinated individuals: Several SARS-CoV-2 vaccines are available and administered across Pakistan. The study also investigated the antibodies level of participants that received vaccine after recovery from COVID-19. The vaccinated individuals were found to have higher level of anti-COVID19 antibodies than individuals that did not receive COVID-19 vaccine. The bar graph in (Figure 2) presents the antibody response in participants.
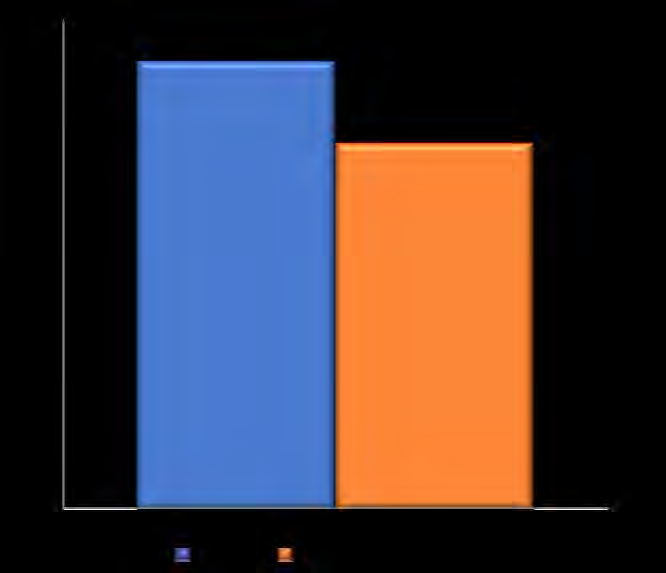
Antibodies response in BCG and non-BCG vaccinated individuals Another important factor considered in this study was antibodies response in participants that received BCG vaccination to those that did not receive BCG vaccine. The data revealed higher anti-COVID-19 antibodies in BCG vaccinated (55%) individuals that non-BCG vaccinated (45%). The antibodies response in BCG and non-BCG vaccinated individuals are presented in (Figure 3).
Questionaries Response
Of the 95-questionnaires distributed among the participants of which 48 were males and 47 were females. The questionnaire presented to the participants of this study is provided in supplementary materials. The data disclosed revealed that 79% of the participant experienced similar symptoms (fever, cold, and cough), 20% of participants experienced shortness of breath and only 1% of the participants were found to had diarrhea during the infection period.
The participants were asked if any of their family member has contracted the infection. The outcome of the survey revealed that only 19 participants had family member with COVID-19 infections whereas the remaining 76 participants were the first individuals to have contracted the infection.
The anti-COVID-19 antibodies response in individuals (aged 45 and above) with severe disease conditions (Cardiac vascular disease, diabetes, asthma, bronchitis, or any other respiratory disease) were reported to have higher antibodies
Discussion
In 2019 a coronavirus pandemic was caused by the SARS-CoV-2 virus, which is a single stranded RNA virus that can be passed between humans. The COVID-19 virus is likely to develop because of SARS-CoV-2 infection. This usually triggers a robust and persistent immune response. These include a virus-specific antibody, memory B cells, and effector and memory CD8+ T cells [7]. A large array of clinical tests has been developed to detect SARS-CoV-2 specific serum-related immune globulins M (IgM) and G (IgG) antibodies to help diagnose the infection. Serum SARS-CoV-2 antibody detection plays an important role in the identification and isolation of COVID-19 patients due to its high sensitivity [8]. It has been controversial whether antibodies against SARSCoV-2 are important. The study was conducted to determine the antibodies response in the COVID-19 recovered patients. In this study COVID-19 antibodies were determined by using COBAS-511 machine. We followed up 95 COVID-19 recovered patients from district Swat who recovered from COVID-19 in the last 6 months including those that received vaccinations post COVID-19 recovery.
The highest level of anti-COVID-19 antibodies was reported in age group 35-45 years followed by age group 55 years and older whereas younger recovered patients has comparatively lower antibodies level, these findings were in line with as reported by Wu, et al. 2020 [9]. Frasca, et al. has also reported the level of antibodies response decrease with aging [10].
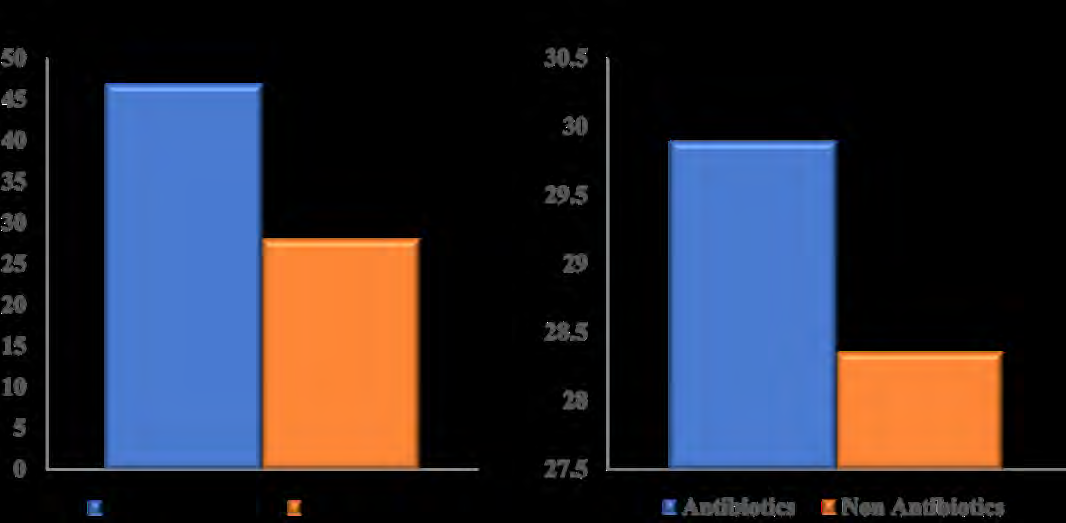
Female individuals were found to have a stronger antibodies response as compared to males (figure 2b). These findings are supported by previously vetted data, as reported by Bunder, et al. women have more robust immune responses to infections and vaccinations as well as a greater susceptibility to autoimmune conditions than men [11]. The response of antibodies against COVID-19 in individuals with severe medical complications such as heart disease or diabetes had higher antibodies response then participants that did not had any medical complications prior to COVID-19. Further studies on how patients with prior medical complications developed higher levels of anti- COVID-19 antibodies might provide valuable evidence for development of anti-SARS-CoV-2 vaccine. Additionally, the variation in antibody level demonstrates the significance of titrating convalescent plasma prior to using it for the treatment and prevention of COVID-19. Previously Imai et al., 2021 in their systematic review and meta-analysis showed a response than those without any prior conditions (Figure 4a). The participants that used different antibiotics/antivirals during the infection period were found to have higher antibodies levels than those that did not use any (Figure 4b).
higher antibody response in COVID19 patients with a greater disease severity, as compared to the low antibody response rates in milder cases [12].
The study also found that participants using different antibiotics had high antibody responses compared to participants not using antibiotics. Additionally, we also found that participants who were injected with BCG had high levels of antibodies in comparison to those who had not received BCG injections.
Based on signs and symptoms, the fever, cold and cough mostly occurred in patients 76%, shortness of breath 4% and diarrhea 20%. The same kind of analysis were performed by Gholami, et al. 2020, according to their results, the fever was 55% found that fever is one of the most remarkable symptoms in patients infected with the coronavirus [3, 13, 14]. This was determined by their systematic review where the fever was 88%. Cough is another important factor of COVID-19 in patients. Additionally, coughing patients may transfer the disease from one patient to another. The cough in the study of Gholami, et al. is 17.9%. Study indicates that cough was 67.7%. Diarrhea is another important clinical symptom of COVID-19. In the study of Gholami, et al. showed that diarrhea was 12.5% individually [15].
This current research study has multiple shortcomings. The study only included a small number of individuals and cannot represent the overall population of the district. Further extended studies are required to validate the outcomes on a larger level, even though this study can provide a base for further detailed studies. The study did not include follow up of the patients post COVID-19 which can further explain the decrease in antibodies level with time in different individuals.
Conclusion
This study concludes that people of age group 45-55 years have higher antibody levels, furthermore similar findings were observed in gender wise antibodies level comparison. Another factor contributing to the higher antibodies level in participants of this study was BCG vaccines where individuals that received the vaccine had higher level of antibodies as compared to those that did not receive the vaccine. The findings are of good value in improving efficiency of vaccines against new variants of SARS-CoV-2 and plasma therapy. Furthermore, detail study with large sample size would be required to validate our findings.
Conflict of Interest
The authors declare no conflict of interest.
Acknowledgement
We are highly thankful to our supervisor Prof, Dr Fazal Akbar Director, Center for Biotechnology and Microbiology, University of Swat for his ample support and providing best working environment.
References
-
Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497-506.
-
Chen N, Zhou M, Dong X, Qu J, Gong F, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223): 507-513.
-
Ma H, Hu J, Tian J, Zhou X, Li H, et al. (2020) Visualizing the naovel coronavirus (COVID-19) in children: what we learn from patients at wuhan childrens hospitals. SSRN Journal.
-
Zhang W, Du RH, Li B, Zheng XS, Yang XL, et al. (2020) Molecular and serological investigation of 2019-nCoV infected patients: implication of multiple shedding routes. Emerg Microbes Infect 9(1): 386-389.
-
Guo X, Guo Z, Duan C, Chen Z, Wang G, et al. (2020) Long- term persistence of IgG antibodies in SARS-CoV infected healthcare workers. Medrxiv.
-
Bentivegna E, Sentimentale A, Luciani M, Speranza ML, Guerritore L, et al. (2020) New IgM seroconversion and positive RT-PCR test after exposure to the virus in recovered COVID-19 patient. J Med Virol 93(1): 97-98.
-
Wheeler SE, Shurin GV, Yost M, Anderson A, Pinto L, et al. (2021) Differential Antibody Response to mRNA COVID-19 Vaccines in Healthy Subjects. Microbiol Spectr 9(1): e0034121.
-
Zainol Rashid Z, Othman SN, Abdul Samat MN, Ali UK, Wong KK, et al. (2020) Diagnostic performance of COVID-19 serology assays. Malays J Pathol 42(1): 13-21.
-
Wu F, Liu M, Wang A, Lu L, Wang Q, et al. (2020) Evaluating the association of clinical characteristics with neutralizing antibody levels in patients who have recovered from mild COVID-19 in Shanghai, China. JAMA Intern Med 180(10): 1356-1362.
-
Frasca D, Diaz A, Romero M, Garcia D, Blomberg BB, et al. (2020) B cell immunosenescence. Annu Rev Cell Dev Biol 36: 551-574.
-
Bunders MJ, Altfeld M (2020) Implications of sex differences in immunity for SARSCoV-2 pathogenesis and design of therapeutic interventions. Immunity 53(3): 487-495.
-
Imai K, Kitagawa Y, Tabata S, Kubota K, Nagura-Ikeda M, et al. (2021) Antibody response patterns in COVID 19 patients with different levels of disease severity in Japan. J Med Virol 93(5): 3211-3218. $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \frac {1}{2} \mathrm {B} ^ {2} + \frac {1}{2} \mathrm {C} ^ {2} $$
-
Gholami A, Hemati R, Khorshidi A, Borji M, Kalvandi G, et al. (2020) The prevalance of clinical symptoms in Children and adolscent with COVID-19: A systematic review and meta-analysis study.
-
Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez- Ocampo E, Villamizar-Peña R, Holguin-Rivera Y, et al. (2020) Clinical, laboratory and imaging features of COVID-19: A systematic review and metaanalysis. Travel Med Infect Dis 34: 101623.
-
Yang Y, Xiao Z, Ye K, He X, Sun B, et al. (2020) SARS-CoV2: characteristics and current advances in research. Virol J 17(1): 117.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions