Prevelence of Pulmonary Tuberculosis, in Catchment Area of Khairpure Medical College Hospital Khairpure Mirs, Pakistan
<p>At present very limited empirical data available on the prevalence of pulmonary tuberculosis among residents of marginalized settings, in catchment area of khairpure medical college hospital khairpure Mir’s, Pakistan. As this disease is poor, low immunity, residing in low line community people. This study assessed the prevalence of pulmonary tuberculosis through active case detection and evaluated predictors of pulmonary tuberculosis among residents of two peri-urban neighborhoods of area of Khairpure medical college khairpure Pakistan. Cases continue to spread infection to close contacts, strategies for tuberculosis case detection need to be improved to minimize the M. tuberculosis transmission. Major threat for the population of khairpure Pakistan and, this infection of the lungs is caused by the Mycobacterium tubercular bacteria. Yet upto date data on the epidemiology of Pulmonary Tuberculosis, in Khairpure Mir’s, Pakistan. Catchment area of Teaching hospital, KMC, khairpure, was not available before this. This study was undertaken to determine the current prevalence rate of Pulmonary Tuberculosis and distribution, is first insight study in khairpure medical college khairpure Mirs, Pakistan, catchment area. As then (WHO) declared a state of global emergency for tuberculosis in 1993, due to the steady increase of the disease worldwide?<br />Result: Sample was taken from the patients irrespective of gender above the age of 15 years, who were advised for tuberculosis screening. Total number of patients were attended 7178 for screening and suspected for pulmonary tuberculosis, from which 785.10.9% were positive and 6392, 89% were negative.<br />Conclusion: This study highlights the poor operational performance of the passive and active case-detection approach in the current tuberculosis control program and indicates higher prevalence of pulmonary tuberculosis in Khairpure medical college hospital khairpure, Pakistan than current national estimates. Our results indicate that active detection of cases and future compare in using the approach outlined in this study and subsequent treatment of cases under DOTS (Tuberculosis is completely curable through short-course chemotherapy. Treating TB cases who are sputum-smearpositive (and who can therefore spread the disease to others) at the source, it is the most effective means of eliminating TB from a population. DOTS or Directly Observed Treatment Short course is the internationally recommended strategy for TB control that has been recognized as a highly efficient and cost-effective strategy. DOTS comprise five components. May have the potential to substantially reduce or not, the increase the burden of pulmonary tuberculosis. As undetected cases continue to spread infection to close contacts, Aerosols, coughing strategies for tuberculosis case detection need to be improved to minimize by vaccination, M. tuberculosis transmission. However, it is also relevant to note that additional costs would arise if active case finding were to be implemented. Improving passive and active case-detection is also a viable option; public health authorities at the very least may wish to consider augmenting health education efforts aimed at prompting health-seeking behavior to facilitate early case detection. Such efforts to improve passive case and active case finding, if combined with easily accessible DOTS infra-structure for treatment of detected cases, may help to diminish the high rate of tuberculosis.</p>
Introduction
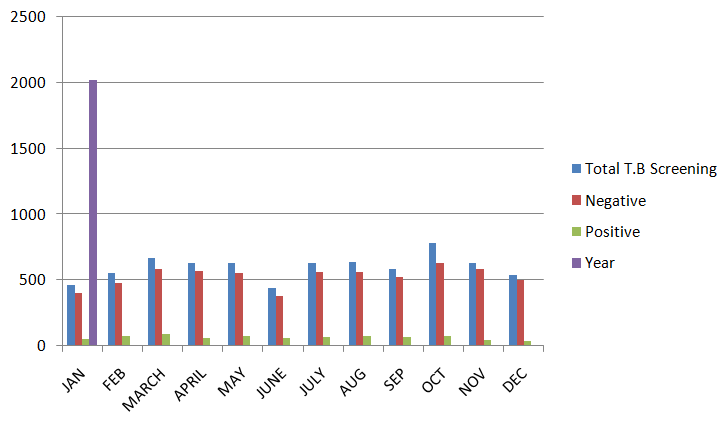
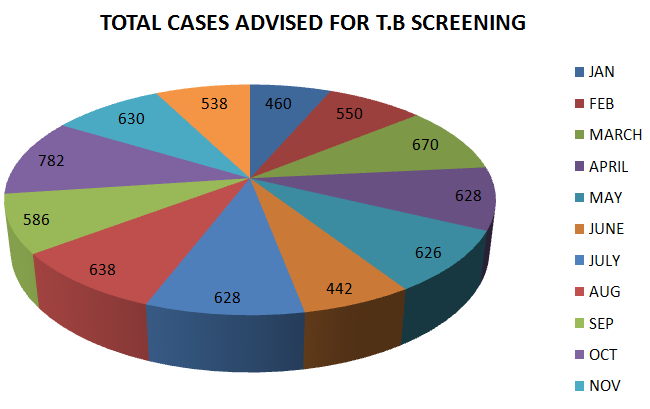
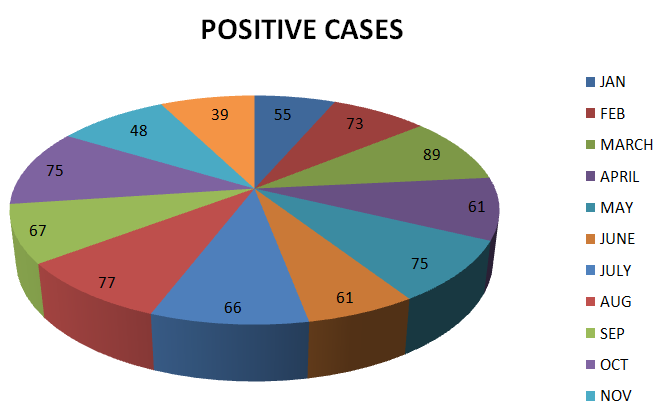
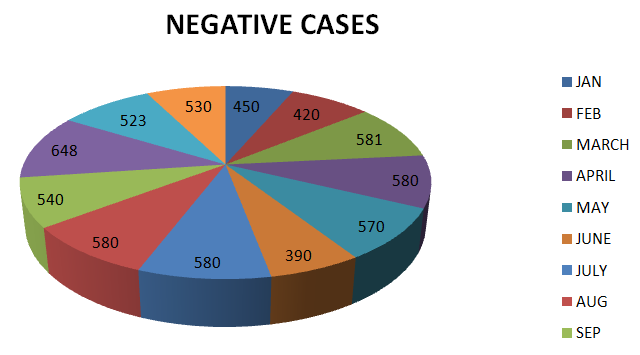
Tuberculosis is a chronic infectious disease caused by Mycobacterium tuberculosis and one of the leading causes of mortality worldwide [1, 2]. However, it is also relevant to note that additional costs would arise if active case finding were to be implemented. Extending such an approach to similar settings in Pakistan and other resource-constrained countries of south Asia would therefore require careful assessment of overall costs and cost-effectiveness [3]. Tuberculosis is a chronic infectious disease caused by Mycobacterium tuberculosis and one of the leading causes of mortality worldwide [1, 2]. Almost one-third of the world population (about 2 billion) is infected with M. However, 95% of tuberculosis cases and 98% of deaths due to tuberculosis occur in impoverished countries of Asia, Africa and South America [3, 4, 5, 6]. Tuberculosis and during the past decade even industrialized countries have faced a resurgence of tuberculosis [6]. However, 95% of tuberculosis cases and 98% of deaths due to tuberculosis occur in impoverished countries of Asia, Africa and South America [4, 5, 6, 7]. In this study, the prevalence (per 100,000) of pulmonary tuberculosis among those aged 15 years or more, who actually participated in the study was 329 (95% CI: 195– 519) and prevalence adjusted for non-sampling was 438 (95% CI: 281–651). These figures appear among the highest in world [8]. It is substantially higher than an earlier reported national figure of 171/100,000 for Pakistan [8] In Pakistan, the estimated incidence of all types of TB in 2011 was 231 per 100,000 populations with 64% cases detection rate for all types of TB. In 2014, the estimated TB prevalence was notified 342 per 100,000 populations in Pakistan, an incidence of 275 per 100,000 populations. The case detection rate for all types of TB are 58% while in 2014, 298446 cases were reported in the country [9]. None of the demographic and socio- economic factors was associated with pulmonary tuberculosis status of the subjects in this study. However, there were only 18 cases; the study had very low power to detect any such potential association of interest. Aside from cough of 2 or more weeks duration, which is incorporated within our algorithm, among the other symptoms considered, none was significantly associated with pulmonary tuberculosis status, which is in contrast to the finding of a study in Mexico [10, 11, 12, 13], wherein blood in sputum was significant predictor of pulmonary tuberculosis. This clinical variable was not statistically significant in our study perhaps due to the low power and may merit further evaluation. Taking into account the results of the univariate analysis, we may therefore conclude that only cough of 2 or more weeks of duration seem to be a reliable predictor of pulmonary tuberculosis status in this population. Pulmonary tuberculosis (TB) and diabetes mellitus (DM) may coexist frequently, particularly in a population at high risk of acquiring TB. DM has been reported to modify the clinical features of TB. Comp parative studies of TB in diabetics have provided conflicting results. In a recent study from Mexico, diabetic patients were older, had lower lung field lesions and had more multiple cavities [14]. In a Turkish study, DM did not affect the pres senting features of pulmonary TB and was only associated with lower lung field disease in females and in older patients [15]. In a random sample of 100 Indian diabetic patients, TB was diagnosed by a positive sputum result in 6% and by radiological examination in 27% [16]. Studies, the prevalence was particularly high in the age groups 40–50 years compared to the other age groups. In our study, the prevalence of TB increased progressively with duration of diabetes. The highest prevalence was seen in those who had been diagnosed with DM for more than 10 years. Comparative studies of type 1 DM and type 2 DM have shown that the prevalence of type 1 DM was 8-times higher in TB patients than in the general population, whereas the prevalence of type 2 DM was similar [17]. The reason for increased susceptibility of diabetics to TB may be multi factorial. Alveolar macrophages play a critical role in eliminating mycobacterium infection in collaboration with lymphocytes. Alveolar macrophages have been found to be less activated in TB patients complicated with DM which may contribute to increased susceptibility [18]. Cavitations were seen in only 26% of our patients. A higher rate of multiple capitation has been reported in many studies [15, 16, 19] but not in others [20]. Among diabetics, patients with type-1 diabetes were found to have more extensive lesions with multiple cavities [21]. The prevalence was particularly high in the age groups 40–50 years compared to the other age groups. In our study, the prevalence of TB increased progressively with duration of diabetes. The highest prevalence was seen in those who had been diagnosed with DM for more than 10 years. Comparative studies of Samples were taken from the patients irrespective of gender above the age of 15 years, who were advised for tuberculosis screening (Table 1, Figure 1). Total number of patients were attended 7178 for screening and suspected for pulmonary tuberculosis, from which 785.10.9% were positive (Figure 2) and 6393, 89% were negative (Figures 3 & 4).
type 1 DM and type 2 DM have shown that the prevalence of type-1 DM was 8-times higher in TB patients than in the general population, whereas the prevalence of type-2 DM was similar [17]. TB patients with type 1 DM have a more acute course of TB, rapid progression, and formation of extensive lesions with multiple cavities [21]. There was early clearance of bacilli and improvement in cavities in type 1 DM compared with type 2 DM.
| Abbreviations: | WHO: World Health Organisation; TB: | |
|---|---|---|
| Tuberculosis; DM: Diabetes Mellitus; DOTS: Directly | ||
| observed treatment short-course. |
Material and Methods
In the current study only the sputum smear, with protocol of AFB staining method and microscopy was performed. Therefore we cannot assume the degree of latent/asymptomatic TB infection. Hence further studies are recommended. A cross-sectional study was conducted in two peri-urban neighborhoods. January 2017 to December 2017. Systematic sampling design was used to select households for inclusion in the study. Consenting subjects aged 15 years or more from selected households were screened and, sputum samples were obtained. Sputum samples were subjected to direct microscopy by Ziehl-Neelson method.
Result
- Month
- Total No of Pt. Advised for T.B
- Negative Cases of
- Positive Cases of
- Tuberculosis
- Year 2017
- Screening
- Tuberculosis.
- Jan
- 460
- 450
- 55
- 2017
- Feb
- 550
- 420
- 73
- 2017
- March
- 670
- 581
- 89
- 2017
- April
- 628
- 580
- 61
- 2017
- May
- 626
- 570
- 75
- 2017
- June
- 442
- 390
- 61
- 2017
- July
- 628
- 580
- 66
- 2017
- Aug
- 638
- 580
- 77
- 2017
- Sep
- 586
- 540
- 67
- 2017
- Oct
- 782
- 648
- 75
- 2017
- Nov
- 630
- 523
- 48
- 2017
- Dec
- 538
- 530
- 39
- 2017
- Total
- 7178
- 6392 & percentage is 89%
- 786.and percentage is
- 10.9%
Table 2: Data of Patients who were advised for T.B Screening. January to December 2o17, in Khairpure Medical
Discussion
Tuberculosis is a chronic infectious disease caused by Mycobacterium tuberculosis and one of the leading causes of mortality worldwide [1, 2]. Taking into account the results of the univariate analysis, we may therefore conclude that only cough of 2 or more weeks of duration seem to be a reliable predictor of pulmonary tuberculosis status in this population. Pulmonary tuberculosis (TB) and diabetes mellitus (DM) may coexist frequently, particularly in a population at high risk of acquiring TB. DM has been reported to modify the clinical features of TB. Comp parative studies of TB in diabetics have provided conflicting results. In a recent study from Mexico, diabetic patients were older, had lower lung field lesions and had more multiple cavities [14]. Pulmonary Tuberculosis is a fatal disease, especially of poor people, low line people, immuno compromised and DM patients, Fever and cough are the common presenting symptoms. Lower lung field and bilateral or multi-lobar involvement is common. An associated effusion may be present. The mortality rate was 10% but was not associated with a particular radiographic appearance. Result shows in my study, of the 7178, 786, 10.9% were positive and active pulmonary Tuberculosis, and negative cases were 6392 and percentage were 89%, if we compare with our neighbor country 100 Indian diabetic patients, TB was diagnosed by a positive sputum result in 6% and by radiological examination in 27% [16]. So we claim there is low prevalence rate in my study area that is khairpure medical college hospital khairpure, Further it should be focused on success of DOTS program (Tuberculosis is completely curable through short-course chemotherapy. Treating TB cases who are sputum-smear positive (and who can therefore spread the disease to others) at the source, it is the most effective means of eliminating TB from a population. Strict monitoring is needed in regard of evaluation, and DOT program, for the eradication of pulmonary tuberculation from this area.
Conclusion
Pulmonary Tuberculosis is a fatal disease, especially of poor people, low line people, immuno compromised and DM patients, Result shows in my study, of the 7178, 785, 10.9% were positive and active tuberculosis and 6393, 89% were negative. This study highlights the poor operational performance of the passive and active case-detection approach in the current tuberculosis control program and indicates higher prevalence of pulmonary tuberculosis in Khairpure medical college hospital khairpure, Pakistan than current national estimates. Our results indicate that active detection of cases and future compare in using the approach outlined in this study and subsequent treatment of cases under DOTS (Tuberculosis is completely curable through short-course chemotherapy. Treating TB cases who are sputum-smear positive (and who can therefore spread the disease to others) at the source, it is the most effective means of eliminating TB from a population. DOTS or Directly Observed Treatment Short course is the internationally recommended strategy for TB control that has been recognized as a highly efficient and cost- effective strategy. DOTS comprises five components may have the potential to substantially reduce or not, the increase the burden of pulmonary tuberculosis. As undetected cases continue to spread infection to close contacts, Aerosols, coughing strategies for tuberculosis case detection need to be improved to minimize by vaccination, M. tuberculosis transmission. However, it is also relevant to note that additional costs would arise if active case finding were to be implemented. Improving passive and active case-detection is also a viable option; public health authorities at the very least may wish to consider augmenting health education efforts aimed at prompting health-seeking behavior to facilitate early case detection. Such efforts to improve passive case and active case finding, if combined with easily accessible DOTS infra-structure for treatment of detected cases, may help to diminish the high rate of tuberculosis.
References
-
Small PM (1996) Tuberculosis Research: Balancing the Portfolio. JAMA 276(18): 1512-1513.
-
Rajeswari R, Balasubramanian R, Muniyandi M, Geetharamani S, Thresa X, et al. (1999) Socio- economic impact of tuberculosis on patients and family in India. Int J Tuberc Lung Dis 3(10): 869-877.
-
Guwatudde D, Zalwango S, Kamya RM, Debanne SM, Diaz MI, et al. (2003) Burden of tuberculosis in Kampala, Uganda. Bull World Health Organ 81 (11): 799-805.
-
Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC (1999) Global Burden of Tuberculosis-Estimated Incidence, Prevalence, and Mortality by Country. JAMA 282(7): 677-686.
-
Sundre P, ten Dam G, Kochi A (1992) Tuberculosis: a global overview of the situation today. Bull World Health Organ. 70(2): 149-159.
-
Raviglione MC, Dye C, Schmidt S, Kochi A (1997) Assessment of worldwide tuberculosis controls. Lancet 350(9078): 624-629.
-
Ahmed Y, Mwaba P, Chintu C, Grange JM, Ustianowski A, et al. (1999) A study of maternal mortality at the University Teaching Hospital, Lusaka, Zambia: the emergence of tuberculosis as a major non-obstetric cause of maternal deaths. Int J Tuberc Lung Dis 3(8): 675-680. [INLINE_TABLE:4:0] [INLINE_TABLE:4:1]
-
Sanchez-Pérez HJ, Flores-Hernández JA, Jansá JM, Caylá JA, Martín- Mateo M (2001) Pulmonary tuberculosis and associated factors in areas of high levels of poverty in Chiapas, Mexico. Int J Epidemiol 30(2): 386-393.
-
Tupasi TE, Radhakrishna S, Rivera AB, Pascual ML, Quelapio MI, et al. (1999) The 1997 Nationwide Tuberculosis Prevalence Survey in the Philippines. Int J Tuberc Lung Dis 3(6): 471-477.
-
Ginsberg AM (1998) The tuberculosis epidemic: Scientific challenges and opportunities. Public Health Re 113(2): 128-136.
-
Sanchez-Perez HJ, del Mar Garcia Gil M, Halperin D (1998) Pulmonary tuberculosis in the border region of Chiapas, Mexico. Int J Tuberc Lung Dis 2(1): 37-43.
-
Pérez-Guzman C, Torres-Cruz A, Villarreal-Velarde H, Salazar-Lezama MA, Vargas MH (2001) Atypical radiol logical images of pulmonary tuberculosis in 192 diabetic patients: a comparative study. Int J Tuberc Lung Dis 5(5): 455-461.
-
Bacakoğlu F, Başoğlu OK, Cok G, Sayiner A, Ateş M (2001) Pulmonary tuberculosis in patients with diabetes mellitus. Respiration 68(6): 595-600.
-
Ezung T, Devi NT, Singh NT, Singh TB (2002) Pulmonary tuberculosis and diabetes mellitus––a study. J Indian Med Assoc 100(6): 376-379.
-
Chukanova VP, Sergeev AS, Pospelov LE, Sobkin AL (2000) Epidemiological and immunogenetic analysis of tuberculosis and diabetes mellitus association. Probl Tuberk 4: 11-14.
-
Wang CH, Yu CT, Lin HC, Liu CY, Kuo HP (1999) Hypodense alveolar macrophages in patients with diabetes mellitus and active pulmonary tuberculosis. Tuberculosis and lung diseases 79(4): 235-242.
-
Ikezoe J, Takeuchi N, Johkoh T, Kohno N, Tomiyama N, et al. (1992) CT appearance of pulmonary tuberculosis in diabetic and immuno compromised patients: comparison with patients who had no underlying disease. American Journal of Roentgenology 159(6): 1175-1179.
-
al-Wabel AH, Teklu B, Mahfouz AA, al-Ghamdi AS, el- Amin OB (1997) Symptomatology and chest roentgenographic changes of pulmonary tuberculosis among diabetics. East Afr Med J 74(2): 62-64.
-
Kossiĭ IUE , Karachunskiĭ MA , Kaminskaia GO , Chernykh NA , Zhukovskaia DE (2002) Pulmonary tuberculosis in patients with different types of diabetes mellitus. Problemy Tuberkuleza 002(5): 21- 24.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future