Prevelence of VDRL Positive in Syphilis, in Catchment Area of Khairpure Medical College Hospital Khairpure Mirs Pakistan
VDRL tests result confirms the patient is suffering from Venereal Disease Research Laboratory (VDRL) positive. The VDRL (Venereal Disease Research Laboratory) test is a serological test used to detect antibodies and thereby screen individuals against syphilis (caused by bacteria called Treponema pallidum). Because of its relatively high sensitivity, and to monitor patients' response to treatment. (The VDRL titre generally comes down with appropriate therapy). Generally a titre of greater than or equal to 1 in 16 is considered indicative of syphilis. However, a limitation of the VDRL test is the fact that its specificity is limited, and can give false positive reactivity (due to cross reactivity with other antibodies). Therefore to confirm syphilis infection specific Treponemal tests such as TPPA (Treponema pallidum Particle agglutination test) or TPHA (Treponema pallidum Haemagglutination test) are used to confirm syphilis. However, these tests are never used in isolation, and assessment of the clinical context (syphilitic ulcer or chancre, rash, lymphadenopathy, history of recent sexual exposure prior to development of signs of The VDRL, however, remains a popular test for syphilis because of the simplicity, relatively low cost, and for its utility in monitoring response to therapy. Most cases of syphilis respond easily to antibiotic treatment (e.g. penicillin) of adequate dose and duration, and a four-fold decline in titre is indicative of a therapeutic response (e.g. from 1/16 to 1/4 or less). Most individuals would become non-infectious after adequate treatment. In some cases however, the antibody response becomes ‘serofast’ (i.e. do not become non-reactive or negative, despite an initial decline, and may continue to give reactive results).<br />Result: Data was collected from January 2017 to December 2017 from which were 42, 2.58% were positive, screened for VDRL, on Elisa method, of the 16215. Patients of either sex, with more than thirty years of age were included. From which 42, 2.58% were positive on Elisa method OUT OF 16215 cases who were asked for screening for syphilis from OPD.<br />Conclusion: Data of 12 months suggest a to very low positive 42,2.58% of the16215 cases of syphilis, on VDRL Test. prevalence rate screened by VDRL test is very low even negligible positive cases of syphilis, at KMC Hospital catchment area Khairpure Mir’s, Pakistan. The modes of transmission of Syphilis are though sex, blood transfusion also plays an important role for prevalence of syphilis. And VDRL is popular method for the syphilis screening method in Pakistan and worldwide accepted method of screening of syphilis, which is sexual transmitted disease. AND using of different partners for sex, blood transfusion, and blood bank running in the town with non qualified pathologists, and blood Transfusion without screening for syphilis, as the major causing factors.
Introduction
Not all sexually transmitted infections (STIs) are reproductive tract infections, nor are all reproductive tract infections sexually transmitted. The ‘ST’ in ‘STI’ denotes the manner of transmission of infection, while reproductive tract infection refers to the site of infection. In 1999, 340 million new cases of four curable STIs (gonorrhea, chlamydia, syphilis and trichomoniasis) occurred. These infections represent a major global health problem leading to morbidity, mortality and stigma. Control of STIs has been given priority since the advent of the HIV/ AIDS epidemic, in recognition of their role in facilitating the sexual transmission of HIV. Although the course of many of these STIs is benign even without treatment, some infections may lead to long-term sequel, including pelvic inflammatory disease, infertility and cervical cancer. Their epidemiological profile varies with geography and depends upon ethnic, demographic, social and economic factors [1]. Syphilis emerged as a major STI in Faisalabad. Syphilis, caused by Treponema pallidum, facilitates the transmission of HIV [1] We observed a 29.5% prevalence of syphilis, which supports the studies by Basal et al and Rehan, reporting 32.4% and 31.6% syphilis infection rate, respectively, in the region. In the United States, the rate of syphilis infection was 2.1 cases per 100,000 persons in 1999 [2]. Syphilis infection has reached alarming rates (13.8%-19.5%) in China [3]. In the Peruvian Amazon, it was 6.3% [4]. Different studies have reported the prevalence of active syphilis as follows, 9% in Northwestern Tanzania, 1.8% in China, 4% in South Africa and 0.2% in South Korea [5, 6]. In the rural population of Punjab, India, syphilis was altogether absent [7]. 1Religious and social ethics are highly admired and deeply ingrained in the Pakistani society. Many people in Pakistan are severely disadvantaged in terms of income, education, power structure, or gender. Addressing these basic issues of human rights lies at the core of achieving better health outcomes. Certain key features have a direct bearing on Pakistan's health- delivery system: the population size and distribution, the country's geography, the gender ratio and the socioeconomic development of people. The majority of the population, 69%, is rural. Poverty is widespread-31% of Pakistanis subsist on US$1 per day, and 85% earn less than US$2 per day. With only 22% of the population economically active, the proportion of people officially unemployed is currently 20%. All these factors are compounded by cultural practices. Pakistan is a male- dominated society, and prejudice against women is reflected in the higher female mortality rate and low literacy rate. This combination of factors gives rise to strong negative repercussions on health [1, 2, 3]. Dynamic changes in clinical patterns of STIs must be acknowledged and tracked in populous cities like Faisalabad. The present study assesses the prevalence and knowledge of some common STIs in Faisalabad, Pakistan. Religious and social ethics are highly admired and deeply ingrained in the Pakistani society. Many people in Pakistan are severely disadvantaged in terms of income, education, power structure, or gender. Addressing these basic issues of human rights lies at the core of achieving better health outcomes. Certain key features have a direct bearing on Pakistan's health-delivery system: the population size and distribution, the country's geography, the gender ratio and the socioeconomic development of people. The majority of the population, 69%, is rural. Poverty is widespread-31% of Pakistanis subsist on US$1 per day, and 85% earn less than US$2 per day. With only 22% of the population economically active, the proportion of people officially unemployed is currently 20%. All these factors are compounded by cultural practices. Pakistan is a male-dominated society, and prejudice against women is reflected in the higher female mortality rate and low literacy rate. This combination of factors gives rise to strong negative repercussions on health [8, 9, 10]. Dynamic changes in clinical patterns of STIs must be acknowledged and tracked in populous cities like Faisalabad. The present study assesses the prevalence and knowledge of some common STIs in Faisalabad, Pakistan. During infection, Hemophilus ducreyi thrives in the extracellular environment comprised of antibacterial components, such as phagocytes, of the innate and adaptive immune responses [10]. Our observed prevalence of H ducreyi infections (1.4%) was in accordance with that reported in Durban, South Africa (1.2%) [11]. Five-year (1995-1999) surveillance for STIs in Saudi Arabia indicated a 0.2% prevalence of cancroids [12]. Contrary to our findings, H ducreyi occurrence rates of 3% in Paris, 13% in Kuwait and 17.2% in rural Pakistan have been reported [13]. Lack of knowledge and misconceptions in beliefs and attitudes were prominent in our cohort, as reported earlier [14, 15, 16]. Although relatively fewer numbers of sexual partners per subject were reported in this study, consistent condom use was low. There is an acute need to enhance condom usage and STI-related counseling. In addition, health services need to be modified to ensure early diagnosis and treatment. Pakistan is a Muslim country where lay knowledge regarding STIs is poor. Surveillance arrangements are limited and frequently ignored, with the result that the true incidence of STIs is unknown. Modern diagnostic techniques are not widely deployed, and there is little standardization of medical arrangements. Syphilis emerged as a major STI in Faisalabad. Syphilis, caused by Treponema pallidum, facilitates the transmission of HIV [3]. We observed a 29.5% prevalence of syphilis, which supports the studies by Basal, et al. & Rehan, reporting 32.4% and 31.6% syphilis infection rate, respectively, in the region. In the United States, the rate of syphilis infection was 2.1 cases per 100,000 persons in 1999 [4]. Syphilis infection has reached alarming rates (13.8%-19.5%) in China [8]. In the Peruvian Amazon, it was 6.3% [6]. Different studies have reported the prevalence of active syphilis as follows, 9% in Northwestern Tanzania, 1.8% in China, 4% in South Africa and 0.2% in South Korea [7]. In the rural population of Punjab, India, syphilis was altogether absent [17]. The factors that determine health behaviors in Pakistan may be seen in various physical, socioeconomic, cultural and political contexts. Religious and social ethics discourage open discussion of sexual matters. The low social status of women limits their economic options, and women may exchange sex for money or other forms of support. Poor health services offer little for the prevention and treatment of STIs. Various factors, including proximity, affordability, availability, family pressure and strong community opinion, lead to self-care and consultation with traditional healers, Hakeem’s or even quacks. Long-held misconceptions continue to contribute to the national neglect of STI treatment and prevention. Prompt STI detection, prevention and STI- related counseling in STI clinics for vulnerable groups, as well as educational interventions, should be the requisites of public and private health sectors in Pakistan [18]. According to the World Health Report 1999, STIs excluding HIV accounted for 1.2% disability adjusted life years (DALYs) during 1998; 0.8% among males and 1.7% among females [19]. Because STIs and their squeal have a widespread effect on men, women, youth and newborns, the problem of curable STIs is costly to individuals and the health care system. The World Bank has estimated that STIs collectively rank second in importance among diseases for which intervention is possible and those four curable STIs, gonorrhea, chlamydia infection, syphilis and cancroids rank among the top 25 causes of healthy days of life lost in sub-Saharan Africa. Epidemiological studies from sub-Saharan Africa, Europe and North America have suggested that there is approximately four times greater risk of becoming HIV-infected in the presence of a genital ulcer such as caused by syphilis and/or cancroids; and a significantly, increased risk in the presence of STIs such as gonorrhea, chlamydia infection and trichomoniasis, which cause local accumulations of lymphocytes and macrophages [17]. In order to evolve effective prevention strategies as well as efficient and cost-effective means for treating sexually transmitted infections, it is important to have a better understanding of what STIs the men are most likely to encounter, what are the most common modes of transmission and where the men are most likely to get treatment for such diseases. The aim of this present study was to generate similar data for Pakistan covering the afore-said parameters. Syphilis causes significant morbidity 1-5. It is also highly infectious. It is estimated that 30-60% of sexual contacts of individuals with early syphilis acquire syphilis3. It is also an important facilitator of HIV transmission [19, 17].
Syphilis is characterized by a prolonged latent stage in which the patient is infectious but asymptomatic [1, 2, 3]. Serological tests with high sensitivity and specificity are available for screening of asymptomatic individuals and for confirmation of diagnosis in those with clinical signs suggestive of the disease [1, 8, 18]. Despite being a readily treatable infection, syphilis remains a common sexually transmitted infection. Although accurate figures about the prevalence of syphilis are not available, population-based studies have shown the seropositivity in various groups of our population [20, 18]. Screening in medicine, is a strategy used in a population to detect a disease in individuals without signs or symptoms of that disease [17, 18]. Points to be considered in the evaluation of mass screening programs include, incidence and prevalence of the disease, available screening tests, predictive value of tests used, yield, acceptance, follow-up services, costs and benefits, and control over the spread of infection. Given the prolonged latent stage of the syphilis and availability of serological tests with high sensitivity and specificity and very cheap curative treatment, an important factor for evaluating the cost effectiveness and benefit of routine screening for syphilis in a given population, is the seropositivity of the disease in that population [3, 5, 18]. Syphilis seropositivity data provide valuable information about community syphilis morbidity for use in prevention and control programs.35.There is no data regarding seropositivity of syphilis in Pakistani soldiers, hence it is not possible to evaluate the need for routine screening. Aim of this cross sectional study was to know the seropositivity of syphilis in a cohort of Pakistani soldiers [18].
Material and Method
Study Area
This descriptive hospital based study was conducted between January, 2017 to December, 2017 at Khairpure medical college teaching hospital from pathological laboratory catchment Area (Table 1). This hospital is a 500 bed Medical college based hospital khairpure Mirs Pakistan. That offers both emergency care and specialized care for patients of all ages. The pathological research laboratory Khairpure medical college teaching hospital from pathological laboratory catchment Area is situated in the hospital premises.
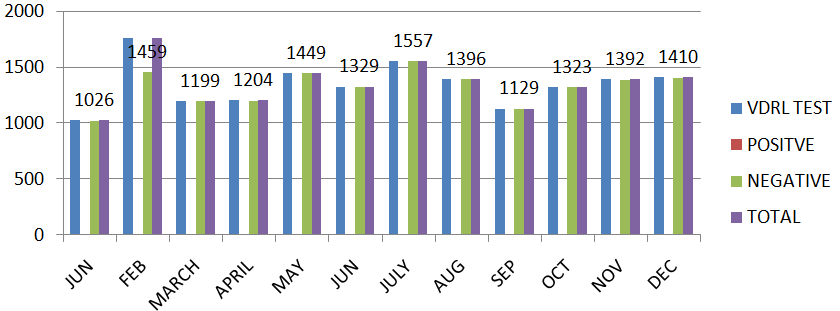
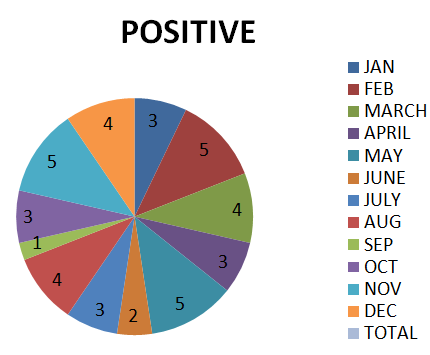
| Month | VDRL Test | Positive | Negative | Total |
| Jan | 1029 | 3 | 1026 | 1029 |
| Feb | 1764 | 5 | 1759 | 1764 |
| March | 1203 | 4 | 1199 | 1203 |
| April | 1207 | 3 | 1204 | 1207 |
| May | 1454 | 5 | 1449 | 1454 |
| June | 1331 | 2 | 1329 | 1331 |
| July | 1560 | 3 | 1557 | 1560 |
| Aug | 1400 | 4 | 1396 | 1400 |
| Sep | 1130 | 1 | 1129 | 1130 |
| Oct | 1326 | 3 | 1323 | 1326 |
| Nov | 1397 | 5 | 1392 | 1397 |
| Dec | 1414 | 4 | 1410 | 1414 |
| Total | 16215 | 42.258% | 16173 | 16215 |
Table 1: KMC teaching Hospital Khairpur Mir’s, month Wise VDRL Report from January to December, 2017.
After getting verbal consent from all eligible subjects, pre-test counseling was done with the assurance that all information obtained would be kept confidential and for the purpose of research only.
All Patients above thirty years, with either sex, suspected for and referred and suspected for syphilis (Figure 1), the subjects were interviewed on a structured questionnaire regarding age, sex, place of residence, literacy level, exposure to blood transfusions, and sexual contact, family history etc.
Screening for Syphilis through VDRL Test on Chromatography
A two to three-milliliter blood sample was collected by venepuncture aseptically into a sterile test tube from each patient and tested for syphilis on VDRL method antibodies within first one hours of collection. The screening was performed through the Chromatography, detection of surface antigen of Syphilis. Samples positive for either Syphilis. Samples repeatedly reactive for syphilis, considered positive (Figure 2). The subjects positive for syphilis were referred to the department of Medicine for further evaluation and treatment (Table 2).
| Month | Positive | VDRL Test | Negative | Total |
|---|---|---|---|---|
| Jan | 3 | 1029 | 1026 | 1029 |
| Feb | 5 | 1764 | 1759 | 1764 |
| March | 4 | 1203 | 1199 | 1203 |
| April | 3 | 1207 | 1204 | 1207 |
| May | 5 | 1454 | 1449 | 1454 |
| June | 2 | 1331 | 1329 | 1331 |
| July | 3 | 1560 | 1557 | 1560 |
| Aug | 4 | 1400 | 1396 | 1400 |
| Sep | 1 | 1130 | 1129 | 1130 |
| Oct | 3 | 1326 | 1323 | 1326 |
| Nov | 5 | 1397 | 1392 | 1397 |
| Dec | 4 | 1414 | 1410 | 1414 |
| Total | 42.258% | 16215 | 16173 | 16215 |
Table 2: Shows the Positive 42 VDRL advised for Screening for Syphilis of the 16215 patients advised Suspected for Table 2: Shows
Discussion
Data of 12 months suggest a to very low positive 42,2.58% of the 16215 cases of syphilis, on VDRL Test. prevalence rate screened by VDRL test is very low even negligible positive cases of syphilis, at KMC Hospital catchment area Khairpure Mir’s , Pakistan [20]. The modes of transmission of Syphilis are though sex, blood transfusion also plays an important role for prevalence of syphilis. And VDRL is popular method for the syphilis screening method in Pakistan and worldwide accepted method of screening of syphilis, which is sexual transmitted disease. AND using of different partners for sex, blood transfusion, and blood bank running in the town with non qualified pathologists, and blood Transfusion without screening for syphilis, , as the major causing factors. If we compare the result of another area of Pakistan there is high no of perseverance rate of syphilis. Syphilis emerged as a major STI in Faisalabad. Syphilis, caused by Treponema pallidum, facilitates the transmission of HIV [1]. We observed a 29.5% prevalence of syphilis, which supports the studies by Basal, et al. & Rehan, reporting 32.4% and 31.6% syphilis infection rate, respectively, in the region. In the United States, the rate of syphilis infection was 2.1 cases per 100 000 persons in 1999 [4]. Syphilis infection has reached alarming rates (13.8%-19.5%) in China [5]. In the Peruvian Amazon, it was 6.3% [8]. Different studies have reported the prevalence of active syphilis as follows, 9% in Northwestern Tanzania, 1.8% in China, 4% in South Africa and 0.2% in South Korea [7]. In the rural population of Punjab, India, syphilis was altogether absent [20]. Religious and social ethics are highly admired and deeply ingrained in the Pakistani society. Many people in Pakistan are severely disadvantaged in terms of income, education, power structure, or gender. Addressing these basic issues of human rights lies at the core of achieving better health outcomes. Certain key features have a direct bearing on Pakistan's health- delivery system: the population size and distribution, the country's geography, the gender ratio and the socioeconomic development of people. The majority of the population, 69%, is rural. Poverty is widespread-31% of Pakistanis subsist on US$1 per day, and 85% earn less than US$2 per day. With only 22% of the population economically active, the proportion of people officially unemployed is currently 20%. All these factors are compounded by cultural practices. Pakistan is a male- dominated society, and prejudice against women is reflected in the higher female mortality rate and low literacy rate. This combination of factors gives rise to strong negative repercussions on health [1, 2, 3, 4, 5]. Dynamic changes in clinical patterns of STIs must be acknowledged and tracked in populous cities like Faisalabad. The present study assesses the prevalence and knowledge of some common STIs in Faisalabad, Pakistan. if take prevalence rate of syphilis , Faisalabad the town of Pakistan there is very high that is 29%,In USA its 2 per one lack, in CHINA its 19.5%. Above study shows the prevalence rate of syphilis is very low at my study area i.e. Khairpure medical college hospital khairpure, Pakistan catchment area. Further this percentage that is 2.58% of my study area is very low but it should be zero tolerance.
References
-
Kinghorn GR (2010) Syphilis and Bacterial Sexually Transmitted Infections. In: Burn T, et al. (Eds.), Rook’s Textbook of Dermatology 8th (Edn.), Oxford: Wiley- Blackwell, pp: 34.1-34.37.
-
Shaikh BT, Hatcher J (2005) Complementary and alternative medicine in Pakistan: Prospects and limitations. Evid Based Complement Alternat Med 2(2): 139-142.
-
Shefer T, Strebel A, Wilson T, Shabalala N, Simbayi L, et al. (2002) The social construction of sexually transmitted infections (STIs) in South African communities. Qual Health Res 12(10): 1373-1390.
-
Singh AE, Romanowski B (1999) Syphilis: review with emphasis on clinical, epidemiologic, and some biologic features. Clin Microbiol Rev 12(2): 187-209.
-
Hope-Rapp E, Anyfantakis V, Fouéré S, Bonhomme P, Louison JB, et al. (2010) Etiology of genital ulcer disease. A prospective study of 278 cases seen in an STD clinic in Paris. Sex Transm Dis 37(3): 153-158.
-
Jawad F (2003) Diabetes in Pakistan. Diabetes Voice 48: 12-14.
-
Mosha F, Nicoll A, Barongo L, Borgdorff M, Newell J, et al. (1993) A population-based study of syphilis and sexually transmitted disease syndromes in north- western Tanzania. 1. Prevalence and incidence. Genitourin Med 69(6): 415-420.
-
Egglestone SI, Turner AJ (2000) Serological diagnosis of syphilis. PHLS Syphilis Serology Working Group. Serological diagnosis of syphilis. Commun Dis Public Health 3: 158-162.
-
Sanchez MR (2008) Syphilis. In: Wolff K (Eds.), Fitzpatrick’s dermatology in general medicine 7th (Edn.), New York, Mc Graw Hill pp: 1955-1977.
-
World Bank (1993) the World Development. Report 1993 Washington, the World Bank.
-
O′Farrell N, Morison L, Moodley P, Pillay K, Vanmali T, et al. (2008) Genital ulcers and concomitant complaints in men attending a sexually transmitted infections clinic: Implications for sexually transmitted infections management. Sex Transm Dis 35(6): 545- 549.
-
Madani TA (2006) Sexually transmitted infections in Saudi Arabia. BMC Infect Dis 6: 3.
-
Goh BT (2005) Syphilis in adults. Sex Transm Infect 81(6): 448-452.
-
Raheel H, White F, Kadir MM, Fatmi Z (2007) Knowledge and beliefs of adolescents regarding sexually transmitted infections and HIV/AIDS in a rural district in Pakistan. J Pak Med Assoc 57(1): 8-11.
-
Al-Mutairi N, Joshi A, Nour-Eldin O, Sharma AK, El- Adawy I, et al. (2007) Clinical patterns of sexually transmitted diseases, associated sociodemographic characteristics, and sexual practices in the Farwaniya region of Kuwait. Int J Dermatol 46(6): 594-599.
-
Haque N, Zafar T, Brahmbhatt H, Imam G, ul Hassan S, et al. (2004) High-risk sexual behaviours among drug users in Pakistan: Implications for prevention of STDs and HIV. Int J STD AIDS 56(1): 65-72.
-
Golden MR, Marra CM, Holmes KK (2003) Update on syphilis, resurgence of an old problem. JAMA 290(11): 1510-1514.
-
Ejaz A, Khan EA, Khokhar N, Malik GJ (2004) seropositivity of syphilis in asymptomatic adults seeking employment abroad. Rawal Med J 29: 65-67.
-
Cho YH, Kim HO, Lee JB, Lee MG (2003) Syphilis prevalence has rapidly decreased in South Korea. Sex Transm Infect 79(4): 323-324.
-
Jindal N, Aggarwal A, Gill P, Sabharwal, Sheevani BB (2009) Community-based study of reproductive tract infections, including sexually transmitted infections, among the rural population of Punjab, India. Indian J Community Med 34(4): 359-361.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future