Important Female Factors Affecting Success in Assisted Reproductive Technology Procedures
Infertility is a hot topic in the field of public health, affecting about 48.5 million couples worldwide with significant psychological, social, medical and economic consequences. Assisted Reproductive Technology offers solution to this problem. For patients that are unable to conceive naturally, medical advances have greatly expanded treatment options. Assisted Reproductive Technology has highly evolved since the first child was born in 1978. However, still many couples are unable to conceive even with all these advancements partly because infertility is a complex condition resulting from multiple factors. Some of these factors are women age, obesity, eating disorders, profession, environmental factors, stress, sleeping disorders and certain life style issues. The infertility could be due to male or female factor (s), however, this review focuses only on important female factors that are likely to impact outcome in Assisted Reproductive Technology procedure. The contents of this review are derived from PubMed literature search. Published articles were grouped into different categories. The relevant information is extracted and presented in a concise manner.
Introduction
The desire to reproduce is a basic human characteristic. However, for many individuals, the chances of having a genetic child are compromised by a number of factors [1]. The men and women both are prone to infertility. Due to significant differences in reproductive systems of men and women, the later is under a time restriction as men are able to produce sperm for all their life, whereas women are given a specific number of eggs. The loss of oocytes in females starts when they are in womb and continues until this pool is depleted. The quality of oocytes also decreases with age; therefore, female aging is associated with a dramatic increase in infertility, a high risk of miscarriage and giving birth to infants with Down’s syndrome [2]. Thus, female infertility is a frequent consequence of delaying conception to late reproductive years. Other factors that affect women fertility include obesity, eating disorders, profession, environmental factors, stress, sleeping disorders and certain life style issues. The female duration of subfertility, follicle stimulating hormone level on day-2 of the menstrual cycle, and number of oocytes, all reflect ovarian function and are predictors of pregnancy after IVF [3]. The purpose of this review is to discuss important physiological issues that affect female fertility.
Pathological conditions like tubal obstruction, severe endometriosis, endocrine hormone disturbances, polycystic ovarian syndrome, ovulatory dysfunction, diminished ovarian reserve, unexplained and male factor infertility are beyond the scope of this review, for which medical consultation from a fertility specialist is recommended.
Factors Affecting Female Fertility
Infertility is a condition when a couple fails to conceive after 12 consecutive months of regular unprotected sexual intercourse without the use of contraceptives or fails to carry a full term pregnancy. Slightly over half of all infertility cases are due to female conditions, while the rest are caused by male factors, unidentified factors or combination of both male and female factors.
General Health
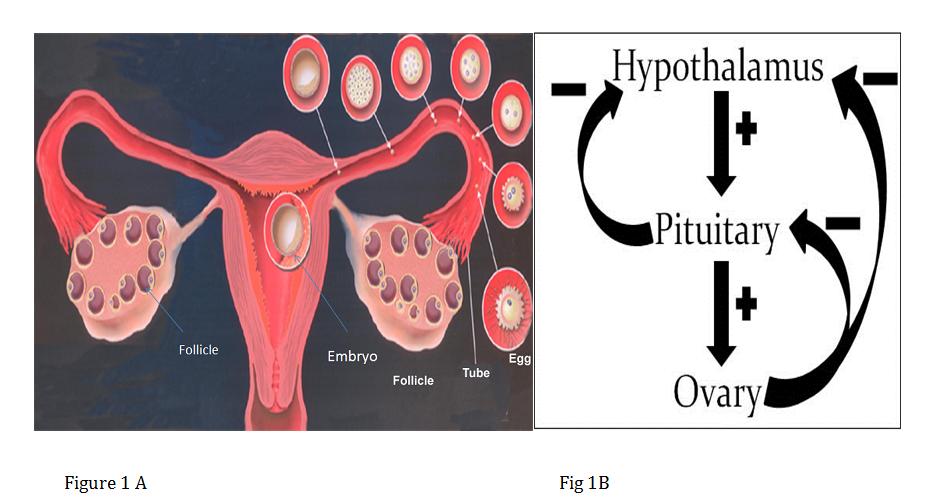
The components of female reproductive system are shown in Figure 1A. Briefly, they include; hypothalamus, pituitary, ovaries, fallopian tubes, uterus, cervix and vagina. A good general health is a prerequisite for normal fertility. Figure 1B explains some of the hormonal pathways affecting ovarian response. Any condition that affects the general health like diabetes or hypothyroidism or the normal hormonal release will also have impact on reproductive health.
Age
Infertility, spontaneous abortion and conception of trisomic offspring (e.g. Down’s syndrome babies in human) increase exponentially with age in mammals but in women there is an apparent acceleration in the rate from about age 37 [2]. As women increasingly defer child bearing due to educational, professional or personal pursuits, infertility problem is becoming a growing social, psychological, health and economic issue. Older women have an extremely high rate of early pregnancy loss of both chromosomally normal and abnormal conceptions and increased rates of spontaneous abortions. Trisomic and monosomic (aneuploid) embryos account for at least 10% of human pregnancies and, for women nearing the end of their reproductive lifespan, the incidence may exceed 50% [4]. The age-related increase in aneuploidy in human female is due to interaction between oogenesis and many endogenous and exogenous factors. Advances in preimplantation genetic diagnosis (PGD) and preimplantation genetic screening (PGS) in Assisted Reproductive Technology provide powerful approaches to detect aneuploidy in human embryos before implantation and to address questions about the influence of environmental factors on human female oogenesis.
Intra Uterine Insemination in women over 40 is associated with a low rate of ongoing pregnancy, therefore, it should not be offered always as the first line of treatment in this age group. When the predictive factors are positive IVF/ICSI seems to be good alternatives until 43 years of age. Currently, oocyte cryopreservation technology is available to women who intend to delay their childbearing age or protect their fertility from toxic agents [1] and to have child from their own eggs later. Devine, et al. 2015 [5] proposed 3 strategies for women who tend to delay child bearing. Strategy 1: Cryopreserve 16 MII oocytes at age 35 yrs, try timed intercourse for 6 months at age 40yrs, if no success, use frozen oocytes in 2 cycles. Strategy 2: Cryopreserve 16 MII at age 35yrs, try timed intercourse for 6 months at age 40 yrs, if no success, try 2 autologous IVF cycles before utilizing cryopreserved oocytes. Strategy 3: No oocyte cryopreservation, try timed intercourse for 6 months at age 40 yrs, if no success, try 2 IVF attempts. Strategy 4: The authors of this manuscript have observed that a new strategy is being adopted widely i.e. try 2 cycles of autologous IVF cycles at age 40 yrs and if no success, use donated eggs from young women below 35 yrs of age. Recently many donor egg banks are successfully operating in developed countries owing to the success of oocyte cryopreservation and thawing. Strategy 5: Some women may not have success through any of the above strategies and may have to choose the option of either child adoption or remain childless. Over 10-year follow-up survey indicated good psychological adjustment both in childless couples and in post- Assisted Reproductive Technology procedure parents [5]. These findings should be integrated into the information and counselling for would-be parents prior to infertility treatment.
Obesity
Obesity has a significant adverse impact on fertility and is a common problem amongst women of reproductive age. It not only reduces the chance of conception but also the response to fertility treatment and increases the risk of miscarriage, congenital anomalies and pregnancy complications [7]. Other risks include premature labor, stillbirth, perinatal risks such as gestational diabetes and hypertension, need for operative delivery, and other complications such as wound infection and thromboembolism [8]. A few causes of obesity are high calorie foods, devices that reduce or eliminate physical exertion, and nonphysical entertainment.
A normal female body mass index (BMI; body weight in kilograms divided by the square of the height in meters) is 20 – 24.9 kg/m2 and overweight is a BMI of ≥25 kg/m2. A moderate obesity is BMI of 30.0 – 34.9 kg/m2, severe obesity 35.0 – 39.9 kg/m2 and very severe obesity ≥ 40 kg/m2 [7]. For better outcome, treatment should be deferred until the BMI is less than 35 kg/m2. The weight reduction to a BMI of less than 30 kg/m2 is preferable. Obese women require significantly higher dose of rFSH (3272 IU vs. 2587 IU, p < 0.001) and days of stimulation (11.89 ± 4.57 vs. 10.42 ± 2.03, p < 0.001), but exhibit less oocytes retrieved and significantly lower fertilization rate (54.1% vs. 61.1%, p < 0.001) than normal weight women [9].
Eating Disorders
Eating disorders (EDs) are severe illnesses affecting adolescent females and young women of childbearing age with many negative consequences including infertility. The prevalence of current or past ED is estimated between 7.6% and 16% for clinical EDs and if subclinical ED is included, the prevalence reaches 16.7% to 44% [10]. The women suffering from EDs have endocrine dysfunctions, affecting sex hormones levels and fertility. The women with severe eating disorders suffer more often from an ovulatory infertility [11]. The infertility and routine health care visits may provide opportunities for early identification and treatment of women with ED symptomatology [12]. Reproductive outcomes are compromised in women with a history of ED, which emphasizes the importance of reproductive health counseling and monitoring women with ED [13].
Genetic
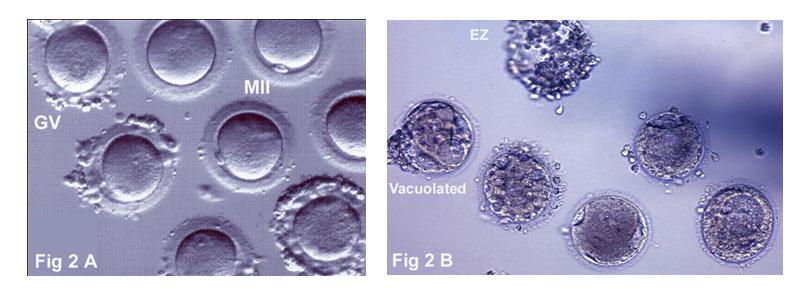
The quality of oocytes varies from cycle to cycle for the same patient and among patients. Normal, mature and functional oocytes are needed for fertilization and further development (Figure 2A). Anatomical, maturity and functional disturbances of oocytes result in impaired oocyte development (Figure 2B). The abnormal dispersion of oocyte chromosomes is indicator for cytoplasmic immaturity and cytoskeletal anomalies in the oocyte, affecting the normal zygote and embryo formation in human IVF-ET practice [14]. Some of these problems can be corrected by the reproductive endocrinologist, however, for genetic defect identification, PGD or PGS is required. The errors that lead to aneuploidy almost always occur in the oocyte. The process of reduction of chromosomes from 46 to 23 (Meiosis) is complex and the age-related increase in errors is not attributable to a single factor but to an interplay between oogenesis and a number of endogenous and exogenous factors [4]. The likelihood of a twin birth after IVF rises with increased concentrations of plasma folate and red-cell folate. The MTHFR genotype is linked to a woman's potential to produce healthy embryos, possibly through interaction with genes related to DNA methylation. In women likely to have a successful IVF pregnancy, high folate status increases the likelihood of twin birth after multiple embryo transfer.
Life Style
Lifestyle factors and nutritional status are critical determinants of normal reproductive function. A combination of reduced exercise, changes in dietary composition, and increased energy intake have contributed to a growing worldwide epidemic in obesity [15]. Lifestyle modifications, in particular a healthy diet and exercise during the 3-6 months before conception and during treatment, should result in better outcomes than requiring weight loss before fertility treatments [8]. Natural conception occurs more frequently in women who received a 6-month lifestyle intervention preceding infertility treatment [16]. Buck et al, 2016 [17] suggested that couples' lifestyles are associated with the risk of pregnancy loss, including during the preconception period, emphasizing the need for continued efforts to promote healthy lifestyles before pregnancy begins. The chances to obtain a pregnancy and a baby are 3-fold higher in obese infertile patients who perform physical activity regularly in comparison with those who do not, suggesting that regular physical activity before ART cycles improves the reproductive performance in obese women irrespective to body weight loss [18]. Food is used as a source of energy for a variety of essential and nonessential functions.
The women should continue to take daily multivitamins before and during pregnancy consistent with clinical guidance. The consumption of specific foods, drinks and some women’s social habits can affect reproductive outcomes. Alcohol and caffeine intake, as well as tobacco smoking, could be important factors in the failure of assisted reproduction procedure. The consumption of coffee is related to decreased fertilization capacity [15]. There appears to be grounds for caution and counselling where women have concerns about night shift work and their reproductive health. The night shift work may give rise to menstrual cycle disturbances. The endometriosis may be elevated in night shift workers but evidence is only preliminary [19]. Another study found that shift workers had increased rates of menstrual disruption and infertility but not early spontaneous pregnancy loss; however, night shifts were associated with increased early spontaneous pregnancy loss [20]. Varying work schedules are suspected of increasing risks to pregnant women and to fetal wellbeing. In particular, maternal hormonal disturbance arising from sleep deprivation or circadian rhythm disruption might impair fetal growth or lead to complications of pregnancy [21]. Other studies have not found conclusive evidence [22]. Thus, available evidence needs to be interpreted with caution, due to various limitations and inconsistencies among the studies in the measurement of night-work exposure and shift-work patterns [23, 24].
Exposure to Environmental Pollutants
Environmental pollutants refer to all of the exogenous, non-essential factors for humans, which, when released into the environment, can be detrimental to human health and/or to the environment. The industrialization of our society maximizes the use of these substances and poses a real problem for public health [25]. In addition to potential reproductive hazards of exposure to environmental contaminants, there is also evidence for adverse reproductive effects of the physical and psychosocial environments [26]. Environmental pollutants are a serious threat to female reproduction with harmful effects that disturb endocrine and reproductive functions. The environmental substances acting as endocrine disruptors seem to play a key role in the onset of mechanisms likely to cause premature ovarian insufficiency [25]. The Phthalates, bisphenol A, pesticides and tobacco were the most reported substances having a negative impact on ovarian function with an increased follicular depletion leading to an earlier menopause onset. In humans, while in- vitro studies have suggested an association between bisphenol A exposure and impaired oocyte meiosis, clinical evidence indicates possible adverse effects of bisphenol A exposure on IVF outcomes [27]. Therefore, products containing bisphenol A should not be used.
Conclusions
Despite significant advances in Assisted Reproductive Technology, many couples have to repeat the procedure multiple times or even fail to conceive. In addition to medical condition(s), many other factors affect success rate. Adapting healthy life style, avoiding environmental toxicants and initiating family creation process early in reproductive age ensure high success rate through Assisted Reproductive Technology procedure.
References
-
Brezina PR (2017) Fertility preservation for social and onco- fertility indications. Minerva Endocrinol.
-
Ford JH (2013) Reduced quality and accelerated follicle loss with female reproductive aging - does decline in theca dehydroepiandrosterone (DHEA) underlie the problem?. J Biomed Sci 20: 93.
-
vanLoendersloot LL, van Wely M, Limpens J, Bossuyt PM, Repping S, et al. (2010) Predictive factors in vitro fertilization (IVF): A systematic review and meta-analysis. Hum Reprod Update 16(6): 577-589.
-
Nagaoka SI, Hassold TJ, Hunt PA (2012) Human aneuploidy: mechanisms and new insights into an age-old problem. Nat Rev Genet 13(7): 493-504.
-
Devine K, Mumford SL, Goldman KN, HodessWertz B, Druckenmiller S, et al. (2015) Baby budgeting: oocyte cryopreservation in women delaying reproduction can reduce cost per live birth. Fertil Steril 103(6): 1446-1453.
-
Wischmann T, Korge K, Scherg H, Strowitzki T, Verres R (2012) A 10-year follow-up study of psychosocial factors affecting couples after infertility treatment. Hum Reprod 27(11): 3226- 3232.
-
Balen AH, Anderson RA, Policy & Practice Committee of the BFS (2007) Impact of obesity on female reproductive health: British Fertility Society, Policy and Practice Guidelines. Hum Fertil (Camb) 10(4): 195-206.
-
Meldrum DR (2017) Introduction: Obesity and reproduction. Fertil Steril 107(4): 831-832.
-
Zhang D, Zhu Y, Gao H, Zhou B, Zhang R, et al. (2010) Overweight and obesity negatively affect the outcomes of ovarian stimulation and in vitro fertilisation: a cohort study of 2628 Chinese women. Gynecol Endocrinol 26(5): 325-332.
-
Bruneau M, Colombel A, Mirallié S, Fréour T, Hardouin JB, et al. (2017) Desire for a child and eating disorders in women seeking in fertility treatment. PLoS One 12(6).
-
Assens M, Ebdrup NH, Pinborg A, Schmidt L, Hougaard CO, et al. (2015) Assisted reproductive technology treatment in women with severe eating disorders: a national cohort study. Acta Obstet Gynecol Scand 94(11): 1254-1261.
-
Cousins A, Freizinger M, Duffy ME, Gregas M, Wolfe BE (2015) Self-report of eating disorder symptoms among women with and without infertility. J Obstet Gynecol Neonatal Nurs 44(3): 380-388.
-
Linna MS, Raevuori A, Haukka J, Suvisaari JM, Suokas JT, et al. (2013) Reproductive health outcomes in eating disorders. Int J Eat Disord 46(8): 826-833.
-
Zhivkova R, Delimitreva S, Vatev I (2010) [Role of oocyte cytoplasmic factors in human IVF failure] AkushGinekol (Sofiia) 49(5): 26-32.
-
Braga DP, Halpern G, FigueiraRde C, Setti AS, Iaconelli A Jr, et al. (2012) Food intake and social habits in male patients and its relationship to intracytoplasmic sperm injection outcomes. Fertil Steril 97(1): 53-59.
-
van Oers AM, Groen H, Mutsaerts MA, Burggraaff JM, Kuchenbecker WK, et al. (2016) Effectiveness of lifestyle intervention in subgroups of obese infertile women: a subgroup analysis of a RCT. Hum Reprod 31(12): 2704-2713.
-
Buck LGM, Sapra KJ, Schisterman EF, Lynch CD, Maisog JM, et al. (2016) Lifestyle and pregnancy loss in a contemporary cohort of women recruited before conception: The LIFE Study. Fertil Steril 106(1): 180-188.
-
Palomba S, Falbo A, Valli B, Morini D, Villani MT, et al. (2014) Physical activity before IVF and ICSI cycles in infertile obese women: an observational cohort study. Reprod Biomed Online 29(1): 72-79.
-
Fernandez RC, Marino JL, Varcoe TJ, Davis S, Moran LJ, et al. (2016) Fixed or rotating night shift work undertaken by women: implications for fertility and miscarriage. Semin Reprod Med 34(2): 74-82.
-
Stocker LJ, Macklon NS, Cheong YC, Bewley SJ (2014) Influence of shift work on early reproductive outcomes: a systematic review and meta-analysis. Obstet Gynecol 124(1): 99-110.
-
Bonzini M, Palmer KT, Coggon D, Carugno M, Cromi A, et al. (2011) Shift work and pregnancy outcomes: a systematic review with meta-analysis of currently available epidemiological studies. BJOG 118(12): 1429-1437.
-
van Melick MJ, van Beukering MD, Mol BW, Frings- Dresen MH, Hulshof CT (2014) Shift work, long working hours and preterm birth: a systematic review and meta-analysis. Int Arch Occup Environ Health 87(8): 835-849.
-
Chau YM, West S, Mapedzahama V (2014) Night work and the reproductive health of women: an integrated literature review. J Midwifery Womens Health 59(2): 113-126.
-
Palmer KT, Bonzini M, Bonde JP, Multidisciplinary Guideline Development Group, Health and Work Development Unit, Royal College of Physicians Faculty of Occupational Medicine (2013) Pregnancy: occupational aspects of management: concise guidance. Clin Med (Lond) 13(1): 75-79.
-
Vabre P, Gatimel N, Moreau J, Gayrard V, Picard Hagen N, et al. (2017) Environmental pollutants, a possible etiology for premature ovarian insufficiency: a narrative review of animal and human data. Environ Health 16(1): 37.
-
Younglai EV, Holloway AC, Foster WG (2005) Environmental and occupational factors affecting fertility and IVF success. Hum Reprod Update 11(1): 43-57.
-
Machtinger R, Orvieto R (2014) Bisphenol A, oocyte maturation, implantation, and IVF outcome: review of animal and human data. Reprod Biomed Online 29(4): 404-410.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era