Correlation between Insulin Resistance and Steroid Endometrial Receptors, KI-67 and BCL-2 after Menopause
Introduction: After menopause, the distribution of weight gain and fat deposits may be altered, with a predominance of abdominal fat. This fat has been correlated with the appearance of metabolic and neoplastic diseases. In the endometrium, proliferative lesions may be mediated by steroid endometrial receptors. The aim of this study was to evaluate the association between steroid receptors, proliferation and apoptotic factors and the presence of insulin resistance (IR) in women after menopause. Methods: The experimental design was an observational cross-sectional study of 85 postmenopausal women. The average age of the women was of 56.8 years (SD= 6.5) with an average menopause period of 81.5 months (SE = 6.39). An atrophic endometrial specimen was collected from asymptomatic, post-menopausal women. An endometrial sample was collected and the expression of estrogen (ER), progestogen (PR) and insulin growth factor-1 (IGF-1R) receptors, as well as Ki-67 and Bcl-2, was evaluated and their correlation with IR was assessed. Results: There was marked expression of ER (94.1%), PR (80%) and IGF-1R (78.8%) in endometrial glands. There was a correlation between the HOMA-IR index and stromal ER (p=0.378) and PR (p=0.0083) expression, as well as a correlation between ER and the expression of Ki-67 (p=0.253) and Bcl-2 (p
Introduction
Obesity and overweight are a public health problem with an elevated mortality rate and are associated with several diseases [1, 2]. After menopause, weight gain and the distribution of fat deposits may be altered, with a predominance of abdominal fat deposition [3]. Abdominal fat is related to the onset of metabolic and neoplastic diseases [4]. Among gynecological neoplasia the most frequent are breast and endometrial cancer [5, 6]. There is considerable controversy regarding the mechanisms involved in the association between obesity and the risk of cancer, although the most plausible links are related to endocrinal and metabolic alterations promoted by adipose tissue [7, 8]. Endocrinal alterations involve the conversion of androgens into estrogens in adipose tissue [9, 10, 11, 12, 13]. On the other hand, the metabolic effects are related to hyperinsulemia mediated by insulin growth factor 1 (IGF-1) [7]. Chronic hyperinsulinemia thereby increases the bioavailability of free IGF-1 [6]. IGF-1 exerts its action through the IGF-1 receptor (IGF-1R) [14]. Therefore, both the endocrine and hormonal factors have influence on the development of endometrial proliferative lesions. These lesions are characterized by high levels of ER and PR, however other factors are also related to cell proliferation. Among these factors we highlight the Ki 67, protein related to the tissue mitogenic activity [15] and Bcl-2 protein expressed in cellular apoptosis. In the endometrium, the Ki 67 presence suggests proliferative capacity [16]. Bcl-2 is also expressed in endometrium with proliferative activity and is related to cellular apoptosis [15, 17]. The pattern of Bcl-2 expression suggests that alterations in this protein occur in response to hormonal variations and this may have an important role in the surge of proliferative endometrial alterations [17]. The objective of this study was to evaluate the factors related to endometrial stimulation and cellular apoptosis, as well as the interaction of ER and IGF-1R with the metabolic state in postmenopausal women. We also examined the mechanisms involved in these interactions that may contribute to the risk of developing endometrial neoplasia.
Materials and Methods
The experimental design consisted of an observational cross-sectional study of atrophic endometrial specimens collected from 85 asymptomatic, postmenopausal women admitted for the removal of endometrial polyps. The study was approved by the institutional Committee for Ethics in Research. The ages of the women ranged from 40 to 75 years and informed consent was obtained from all participants. Patients who had received hormones in the last six months, those taking tamoxifen and those with hyperplastic changes or endometrial cancer were excluded from the study. Menopause was confirmed by quantifying serum follicle stimulating hormone (FSH >40 IU/L). An endometrial tissue sample measuring approximately 0.5 cm, was collected at the moment of surgery from a region without lesions on the other side of the polyp. The tissues samples were processed for immunohistochemistry using standard techniques. Monoclonal primary antibodies were used to detect ER (Dako® Denmark, code M7047, clone 1D5, dilution 1:250), PR (Dako® Denmark, code M3569, clone PgR 636, dilution 1:500), IGF-1R (Genetex® USA GTX24065, dilution 1:15), Bcl-2 (Biogen® USA, code M887, dilution 1:200) and Ki-67 (Dako® Denmark, code M7240, clone MIB 1, dilution 1:1000). The expression of ER, PR, IGF- 1R and Bcl-2 in the stroma and endometrial glands was assessed semi-quantitatively. For this, five sections from each patient were obtained, one for each receptor studied. Ten microscopic fields were read for each section obtained. The number of cells counted and the staining was evaluated in the glands and stroma. The final score was represented by the percentage and intensity of staining expressed, considering the total number of counted cells. Based on the percentage of stained endometrial cells the tissues were scored as zero (0) – no staining, 1 – positivity up to 25%, 2 – positivity from 26-50%, 3 – positivity from 51-75% and 4 – positivity >76%. The intensity of cell staining was scored as zero (0) – no staining, 1 – slightly positive staining, 2 – moderately positive staining and 3 – strongly positive staining. The final score for each tissue sample was based on a combination of the extent (or positivity) and intensity of staining in the stroma and gland cells and was defined as 0 (negative), 2 and 3 (weak), 4 and 5 (moderate) and 6 and 7 (intense). This combined score represented the overall level of expression for each receptor type. Staining for Ki-67 was done semi-quantitatively based only on the percentage of endometrial, stromal and glandular cells that were stained. We didn’t consider the intensity of receptor staining. All stained cells were considered, even though slight, because the Ki-67 rapidly disappeared from post-mitotic cells [18]. The sample size was calculated based on the number of cells that stained for ER in normal endometrial samples, with the level of significance set at 5% and a test power of 80%. The correlation between ER, PR, IGF-1R, Ki-67 and Bcl-2 expression with insulin resistance (IR) was evaluated using the HOMA-IR index and abdominal circumference (AC). Normal values for the HOMA-IR index and AC were <2.7 [19] and <88 cm [20], respectively.
Statistical analyses were done using Pearson’s correlation index for dependent variables and their correlations, and Spearman’s correlation index to determine the strength of the linear relation between the variables. The relationship between the HOMA-IR index and receptor expression was assessed using Fisher´s exact test. All statistical analyses were done using SAS software (SAS/STAT Release 8.2, SAS Institute Inc., Cary, NC, USA) with the level of significance set at 5%.
Results
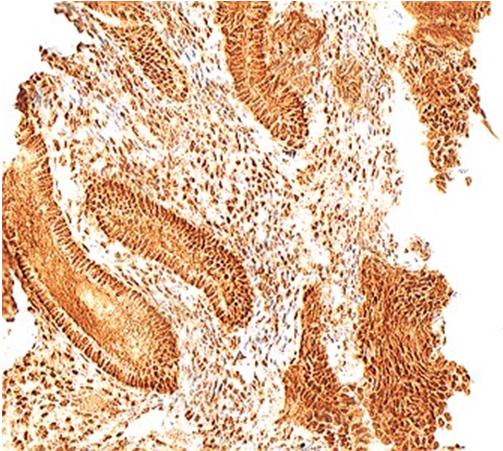
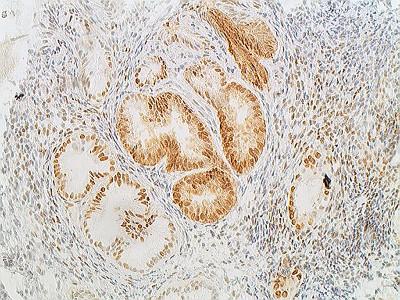
The average age of the women in this study was of 56.8 years (SD = 6.5), with an average menopause period of 81.5 months (SE = 6.39). Most of the women presented overweight and obesity. Mean BMI found was 29.2 kg/m2. No statistical difference was found in relation to body weight and endometrial receptors, probably due to the high BMI of the participants (data not shown). The average of serum estradiol level was 14.8 pg/ml (SD = 13.0). In the IR analysis, 31 women (36.5%) had an HOMA-IR index >2.7. The average HOMA-IR index was 3.6 (SE = 6.5). There was marked expression of the ER, PR, IGF-IR and Bcl-2 in endometrial stroma and gland cells. There was moderate/intense staining for ER in the stroma and gland cells of 78.8% and 94.1% of the samples, respectively (Figure 1). For PR, the corresponding percentages for moderate/intense staining were 61.2% and 80% (Figure 2). The expression of ER and PR was generally greater in women with an elevated HOMA-IR index, except for ER expression in gland cells (Table 1).
| HOMA-IR | p value | ||||
|---|---|---|---|---|---|
| < 2.7 ≥2.7 | |||||
| Stromal ER | n | % | n | % | 0.0378* |
| Negative/weak | 15 | 27.7 | 4 | 13 | |
| Moderate/intense | 39 | 72.3 | 27 | 87 | |
| Glandular ER | 0.1932 | ||||
| Negative/weak | 4 | 7.4 | 2 | 6.5 | |
| Moderate/intense | 50 | 92.6 | 29 | 94 | |
| Stromal PR | 0.0083* | ||||
| Negative/weak | 25 | 46.3 | 8 | 26 | |
| Moderate/intense | 29 | 53.7 | 23 | 74 | |
| Glandular PR | 0.0101* | ||||
| Negative/weak | 15 | 27.8 | 2 | 6.5 | |
| Moderate/intense | 39 | 72.2 | 29 | 94 | |
Table 1: Correlation between the HOMA-IR index and the expression of estrogen (ER) and progestogen.
Table 1: Correlation between the HOMA-IR index and the expression of estrogen (ER) and progestogen. (PR) receptors in endometrial stroma and gland cells. HOMA-IR = Homeostasis model assessment-insulin resistance index. *p value < 0.05. Moderate/intense staining for IGF-1R was observed in 57.6% of the stroma and 78.8% of the glands (Figure 3). The relationship between positivity for staining and the intensity of staining for IGF-1R in stromal and glandular cells was similar to that for ER, i.e., the greater the positivity, the greater the intensity of staining (data not shown).
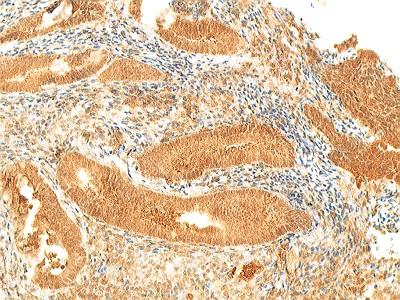
Figure 3: Endometrial tissue sample showing a strong IGF-1 receptor positivity 200x. There was a strong correlation between the levels of expression for IGF-1R and ER in the stroma (p = 0.025). There was no significant correlation between IGF-1R and the HOMA-IR index (p = 0.7932), but there was a correlation with AC (p = 0.0080) in gland cells. Staining for PR in gland cells also correlated with AC (p = 0.0261). Table 2 summarizes the correlations between PR, IGF-1R and AC. There was an inverse correlation between IGF-1R and the levels of serum estrogen (p = 0.0410; r = -0.224).
| AC (cm) | p value | ||||
|---|---|---|---|---|---|
| < 88 > 88 | |||||
| Stromal PR | n | % | n | % | 0.3518 |
| Negative/weak | 5 | 45.5 | 28 | 38 | |
| Moderate/intense | 6 | 54.5 | 46 | 62 | |
| Glandular PR | 0.0261* | ||||
| Negative/weak | 0 | 0 | 17 | 23 | |
| Moderate/intense | 11 | 100 | 57 | 77 | |
| Stromal IGF-1R | 0.7932 | ||||
| Negative/weak | 5 | 45.5 | 31 | 42 | |
| Moderate/intense | 6 | 54.5 | 43 | 58 | |
| Glandular IGF-1R | 0.0080* | ||||
| Negative/weak | 2 | 18.2 | 16 | 22 | |
| Moderate/intense | 9 | 81.8 | 58 | 78 | |
Table 2: Correlation between abdominal circumference (AC) and progestogen receptors (PR) and IGF-1R in endometrial stroma and gla
In 75.3% of the samples there was some expression of Ki-67 (Figure 4). However, even in positively stained cells, the percentage of mitotic cells was rarely >10%. The expression of Ki-67 was greater in gland cells than in the stroma (data not shown). There was no significant difference in the expression of Ki-67 between women with normal or abnormal HOMA-IR indices (p = 0.4986 and p = 0.4320 for stroma and gland cells, respectively). There was a significant positive correlation (r<0.5) between ER and Ki-67 (p = 0.0253) and Bcl-2 (p = 0.0354), but no correlation between Ki- 67 and IGF-1R (p = 0.420). There was moderate/intense expression of Bcl-2 in 44.7% and 65.9% of stromal and gland cells, respectively. However, there was no significant correlation between Bcl-2 and any other variable in this study (data not shown).
Discussion
In this study, postmenopausal women with IR showed greater endometrial expression of ER and PR and in the clinical evaluation based on AC, a correlation between the expression of glandular PR and IGF-1R also was observed, suggesting that IR may cause endometrial stimulation. We have also observed that samples from atrophied endometrium showed intense expression of ER, PR, IGF-1R and Bcl-2. However, the presence of receptors expression couldn’t be exclusively related to endometrium proliferative alterations. Analyzing atrophic endometrium samples of postmenopausal women, we wish to exclude the possibility that the formation of endometrial receptors found, may have been caused by an ovarian estrogen production. ERs are specific nuclear receptors and its formation is due to hormonal factors, however the formation of new ER and its concentration may be related to self- regulation not dependent on hormonal stimulus [21]. The high expression of ER observed in the present study was probably not related only to the serum estrogen levels since the women were hypoestrogenic. Perimenopause is accompanied by changes in the pattern of fat deposits, with an increase in abdominal adipose tissue [22, 23]. This abdominal fat which is evaluated clinically by measuring the AC, is associated with hyperinsulinemia and interferes with hormone production [13]. After menopause, there is persistent androgen production for a few years that is influenced by factors such as age and weight. These androgens undergo peripheral conversion to estrogen in adipose tissue [10]. Similarly, obesity and hyperinsulinemia increase free serum steroids by decreasing the levels of circulating SHBG [13] and SHBG levels correlate inversely with the levels of free estrogen circulating [3, 13]. Insulin resistance may therefore play a central role in the development of endometrial cancer [8]. Although the overweight and obesity was associated an endometrial activity after menopause we didn`t found statistic relationship between them, probably due to high BMD of women of these study. In addition to circulating estrogen levels, the length of time that the target tissue is exposed to estrogen can lead to the formation of new endometrial receptors [23, 24, 25]. As result, it is not uncommon to find weak proliferative activity in atrophied endometrium [15]. However, the low serum estrogen levels observed in the present study suggest that receptor expression was also related to other factors. The circulating insulin levels influences cellular proliferation indirectly from IGF-1R [8], however in an analysis of markers for IR, Papaxoinis, et al. (2007) found that no single marker was associated with enhanced IGF-1R expression [14]. IGF-1R expression is related to ER expression and the stimulation of IGF-1R induces cellular proliferation in neoplastic cells with ER [25]. In fact, IGF-1R expression in ER-positive tumors is greater than in ER-negative tumors. The observation in the present study that IGF- 1R and steroid receptors had similar levels of expression suggests that there is a common regulator for these receptors [26]. The lack of a significant correlation between ER and PR with AC and between IGF-IR and the HOMA-IR index in the present study probably reflects the high rates of overweight and obesity in the sample studied. Estrogens and IGF-1 have a combined and reciprocal action in stimulating mitogenesis [26]. This relationship suggests that IGF-1 may also be involved in cellular alterations, leading to endometrial proliferation that could be related to tumor formation. We have evaluated the mitogenic activity through the expression of Ki-67 and the apoptosis was assessed based on the expression of Bcl-2. Most of the samples analyzes (75.3%) showed a high expression of Ki-67 mainly in gland cells, however despite the high expression of Ki-67 only a small percentage of cells showed mitosis. The expression of Ki-67 and Bcl-2 correlated with that of ER, but not with IGF-1R suggesting that the expression of these proteins is modulated by estrogen and progesterone levels [27, 28, 29].
Atrophied endometrium has a larger number of apoptotic cells and lower expression of Bcl-2 than proliferative endometrium [30]. In the present study, we observed greater expression of Bcl-2 in gland cells, with more uniform positivity and intensity of staining. This observation suggests that Bcl-2 expression before menopause is influenced by cyclical hormonal alterations that do not occur after menopause. Bcl-2 expression in endometrial hyperplasia and endometrial carcinoma is greater than in proliferative endometrium [29, 31]. This finding probably reflects the fact that the binding of estradiol to ER stimulates proliferation and inhibits apoptosis by modulating Bcl-2 expression [31, 32]. Therefore, after menopause the atrophic endometrium may present ER and PR and there are factors that may contribute to the risk of the development of the proliferative lesions even in hypoestrogenic status. In those cases, the hyperinsulinemia may contribute to the occurrence of a diminished apoptosis and increased mitogenic action, increasing the risk for endometrial proliferative stimulus. Our findings show that insulin resistance is related to the levels of steroids endometrial receptors and may contribute to the appearance of proliferative lesions. Studies correlating overweight, obesity and insulin resistance in neoplastic endometrial lesions are needed in order to assess the changes in postmenopausal endometrium and may contribute to be establishing a prophylactic treatment for endometrial cancer. Acknowledgement: *Supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP). Conflict of Interest: The authors have not declared any conflict of interest.
References
-
Stein CJ, Coldiyz GA (2004) The epidemic of obesity. J Clin Endocrinol Metab 89(6): 2522-2525.
-
Raskin DBF, Pinto Neto AM, Paiva LHSC, Raskin A, Martinez Z (2000) Fatores associados à obesidade e ao padrão andróide de distribuição da gordura corporal em mulheres climatéricas. Rev Bras Ginecol Obstet 22(7).
-
Guthrie JR, Dennerstein L, Taffe JR, Ebeling PR, Randolph JF, et al. (2003) Central abdominal fat and endogenous hormones during the menopausal transition. Fertil Steril 79(6): 1335-1340.
-
Chen YL, Cheng WF, Lin MC, Huang CY, Hsieh CY, et al. (2009) Concurrent Endometrial Carcinoma in Patients with a Curettage Diagnosis of Endometrial Hyperplasia. Journal of the Formosan Medical Association 108(6): 502-507.
-
Linkov F, Edwards R, Balk J, Yurkovetsky Z, Stadterman B, Lokshin A, et al. (2008) Endometrial hyperplasia, endometrial cancer and prevention: Gaps in existing research of modifiable risk factors. Eur J Cancer 44(12): 1632-1644.
-
Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M (2008) Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371(9612): 569-578.
-
Calle EE, Kaaks R (2004) Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer 4(8): 579-591.
-
Mu N, Zhu Y, Wang Y, Zhang H, Xue F (2012) Insulin resistance: a significant risk factor of endometrial cancer. Gynecol Oncol 125(3): 751-757.
-
American Cancer Society (2010) Cancer Facts & Figures.
-
Grodin JM, Stiiteri PK, MacDonald PC (1973) Source of estrogen production in postmenopausal women. J Clin Endocrinol Metab 36(2): 207-218.
-
Parslov M, Lidegaard O, Klintorp S, Pedersen B, Jonsson L, et al. (2000) Risk factors among young women with endometrial cancer: a Danish case- control study. Am J Obstet Gynecol 182(1 Pt 1): 23- 29.
-
MacDonald PC, Edman CD, Hemsell DL, Porter JC, Siiteri PK (1978) Effect of obesity on conversion of plasma androstenedione to estrone in postmenopausal women with and without endometrial cancer. Am J Obstet Gynecol 130(4): 448-455.
-
Akin F, Bastemir M, Alkis E, Kaptanoglu B (2009) SHBG levels correlate with insulin resistance in postmenopausal women. Eur J Intern Med 20(2): 162-167.
-
Papaxoinis K, Patsouris E, Kittas C, Nicolopoulou- Stamati P (2007) Insulinlike growth factor I receptor and estrogen receptor beta expressions are inversely correlated in colorectal neoplasms and affected by the insulin resistance syndrome. Hum Pathol 38(7): 1037-1046.
-
Sivridis E, Giatromanolaki A (2004) Proliferative activity in postmenopausal endometrium: the lurking potential for giving rise to an endometrial adenocarcinoma. J Clin Pathol 57(8): 840-844.
-
Taylor LJ, Jackson TL, Reid JG, Duffy SRG (2003) The differential expression of oestrogen receptors, progesterone receptors, Bcl-2 and Ki67 in endometrial polyps. Int J Obstet Gynaecol 110(9): 794-798.
-
Gompel A, Sabourin JC, Martin A, Yaneva H, Audouin J, et al. (1994) Bcl-2 expression in normal endometrium during the menstrual cycle. Am J Pathol 144(6): 195-202.
-
Bruno S, Darzynkiewicz Z (1992) Cell cycle dependent expression and stability of the nuclear protein detected by Ki-67 antibody in HL-60 cells. Cell Prolif 25(1): 31-40.
-
Geloneze B, Vasques ACJ, Stabe CFC, Pareja JC, Rosado LEFPL, et al. (2009) HOMA1-IR and HOMA2-IR indexes in identifying insulin resistance and metabolic syndrome – Brazilian Metabolic Syndrome Study (BRAMS). Arq Bras Endocrinol Metab 53(2): 281-287.
-
Ross R, Freeman J, Hudson R, Janssen I (2002) Abdominal obesity, muscle composition, and insulin resistence in premenopausal women. J Clin Endocrinol Metab 87(11): 5044-5051.
-
Punyadeera C, Verbost P, Groothuis P (2003) Oestrogen and progestin responses in human endometrium. J Steroid Biochem Mol Biol 84(4): 393-410.
-
Austin H, Austin JM Jr, Partridge EE, Hatch KD, Shingleton HM (1991) Endometrial cancer, obesity, and body fat distribution. Cancer Res 51(2): 568- 572.
-
Svendsen OL, Hassager C, Christiansen (1995) Age- and menopause-associated variations in body composition and fat distribution in healthy women as measured by dual-energy X-ray absorptiometry. Metabolism 44(3): 369-373.
-
Lipsett MB. Hormônios esteróides (1999) In: Yen SSC, Jaffe RB. Endocrinologia reprodutiva – fisiologia, fisiopatologia e tratamento clínico. São Paulo, SP: Roca: 135-147.
-
Fogle RH, Chang L, Patel SK, Stanczyk FZ, Paulson RJ (2008) Increased insulin-like growth factor-1 after oophorectomy in postmenopausal women. Fertil Steril 90(4): 1236-1239.
-
Bartucci M, Morelli C, Mauro L, Ando S, Surmacz E (2001) Differential insulin-like growth factor I receptor signaling and function in estrogen receptor (ER)-positive MCF-7 and ER-negative MDA-MB-231 breast cancer cells. Cancer Res 61(18): 6747-6754.
-
Zubor P, Hatok J, Galo S, Dokus K, Klobusiakova D, et al. (2009) Anti-apoptotic and pro-apoptotic gene expression evaluated from eutopic endometrium in the proliferative phase of the menstrual cycle among women with endometriosis and healthy controls. Eur J Obstet Gynecol Reprod Biol 145(2): 172-176.
-
Castro A, Johnson MC, Anido M, Cortinez A, Glaber F, et al. (2002) Role of nitric oxide and bcl-2 family genes in the regulation of human endometrial apoptosis. Fertil Steril 78(3): 587-595.
-
Bozdogan O, Atasoy P, Erekul S, Bozdogan N, Bayran M (2002) Apoptosis-related proteins and steroid hormone receptors in normal, hyperplastic and neoplastic endometrium. Int J Gynecol Pathol 21(4): 375-382.
-
Vaskivuo TE, Stenbäck F, Tapanainen JS (2002) Apoptosis and apoptosis-related factors Bcl-2, Bax, tumor necrosis factor-alpha, and NF-kappaB in human endometrial hyperplasia and carcinoma. Cancer 95(7): 1463-1471.
-
Kokawa K, Shikone T, Otani T, Nishiyama R, Ishii Y, et al. (2001) Apoptosis and the expression of Bax and Bcl-2 in hyperplasia and adenocarcinoma of the uterine endometrium. Hum Reprod 16(10): 2211- 2218.
-
Zhang R, He Y, Zhang X, Xing B, Sheng Y, et al. (2012) Estrogen receptor-regulated microRNAs contribute to the BCL2/BAX imbalance in endometrial adenocarcinoma and precancerous lesions. Cancer Lett 314(2): 155-165..
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era