Factors Associated with Uptake of Emergency Contraception among Female Undergraduate Students in the University of Dar Es Salaam Main Campus, Tanzania
Background: Unwanted pregnancies among young women aged 18-24 remain global public health challenge despite the advancements of a variety of modern contraception methods. Emergency contraception (EC) is the only option available that can be used following an act of unprotected sex to prevent unwanted pregnancy. It reduces women’s risk of becoming pregnant by 99% depending on time taken. However, uptake of EC among young women in Tanzania is very low. The reasons for underutilization are not clear. None of the studies conducted in Tanzania have clearly delineated factors that influence uptake of EC among young women. Methodology: The study enrolled 384 female undergraduate students. A two-stage sampling technique was used; where four (4) departments were selected from the total of twenty-five (25) departments using a random lottery method. Then, the total sample size was allocated to each department proportional to the number of female students in the department. Secondly, study participants were selected from each department proportional to their year of study using simple random sampling technique. The number of study participants from the selected departments was determined using probability proportionate to population size allocation methods depending on the year of study. A structured questionnaire was used to collect data that was then coded and entered in the computer and analyzed using SPSS statistical computer software version 21.0. Exploratory factor analysis, descriptive statistical and logistic regressions analyses were conducted. Results: Exploratory factor analysis showed that sixteen of eighteen items met a minimum primary loading factor of ≥ 0.5 and were used for further analysis. A significant proportion of participants 30% (n=46) of those reported having vaginal intercourse (n=155) in the last six months had ever used EC. Multiple logistic regression analysis indicated that perceived behavioral control (AOR=3, 95% CI, 1.52-5.54; p= 0.001) and perceived self-benefit (AOR=2; 95%CI, 0.98-4.54; p=0.046) were factors associated with the intention to use EC. Conclusion: Perceived behavioral control and perceived self-benefits were positively associated with intention to use EC. However, the utilization of EC was reported to be very low. More complete understanding of the determinants of women’s actual EC behavior is vital to minimize use behaviors that lead to unwanted pregnancy.
Introduction
Unwanted pregnancies among young women aged 18- 24 remain global public health challenge despite the advancements of a variety of modern contraception methods. Approximately 71% pregnancies that occur annually among young women worldwide are unwanted [1]. More than 70% of the pregnancies in African University students are reported to be unwanted, mostly related to lack of contraceptive use, contraception method failure, and rape, as well as lack of knowledge on effective contraceptive methods [2, 3]. Unwanted pregnancies remain a significant problem for young women in Tanzania [4, 5].
In Tanzania, most young unmarried women are sexually active before the age of 15 years [6]. Thus, unwanted pregnancy becomes a major concern to them due to lack of contraceptive use, failure of contraceptive method, as well as lack of knowledge of effective contraceptives [2, 3]. In most cases, such pregnancies end the education of young girls prematurely and restrict them from pursuing rewarding opportunities; effectively perpetuates a life of poverty for them and their children. Additionally, early pregnancies often lead to long-lasting health problems including uterine rupture and vaginal fistula [7]. Induced abortion is a major consequence of unwanted pregnancy worldwide [8]. Unsafe abortion among young women is one of the most significant causes of maternal mortality, contributing22% of the total maternal mortality rate; thus posing a major medical and public health problem [9].
Despite availability of several strategies in Tanzania to reduce unwanted pregnancies among young women, the strategy of EC, defined as the use of any drug or device after an act of unprotected sex to prevent an unwanted pregnancy, is rarely mentioned in the literature [10, 11]. Emergency contraception pill (ECP) is the only method available in Tanzania, and is effective within 120 hours (5 days) after unprotected sex [12]. Emergency contraception reduces women’s risk of becoming pregnant from a single act of intercourse by 75-99%; depending on the timing. The sooner the EC is taken after an act of unprotected sex, the more effective it will be at preventing pregnancy [12], as ECP acts mainly through inhibition of ovulation [13].
Reports from several studies conducted among female University students on knowledge, attitude, perception and use of EC; show that almost 50 percent of young women have heard about EC with minimal accurate knowledge on how to correctly use it. The report also shows that EC use was very low and varied throughout other countries of sub-Saharan Africa, including Uganda (7.4%); Ethiopia (4.7%); and South Africa (21.2%) [3, 14, 15].
While, it remains vital to ensure availability and accessibility of EC to women of reproductive ages, there are non-structural factors reported to hinder their utilization. For instance, ignorance of users, cultural and religious beliefs were reported to be inhibitors of EC use [16, 17]. Another study showed that youth feared the possibility of infertility later in life with the utilization of EC, and the risk of delivering an abnormal baby if EC is taken after conception has already occurred [2].
The theory of planned behavior proposes a model that shows how human action is guided and it has three variables which the theory suggests predict the intention to perform a behavior. The variables are behavioral attitudes, subjective norms, and perceived behavior control (PBC); combination of the three variables will lead to the formation of a behavioral intention. The more favorable the attitude and subjective norm, and the greater the perceived behavioral control, the stronger should be the person’s intention to perform the behavior [18, 19]. The behavior in this study meant those female students who have ever or never used EC. Attitude was conceptualized as perceived self-benefits and harmful from using EC. Subjective norm was conceptualized as the influence of important people (husband, boyfriend, parents, sisters and close friends) with regard to EC use while PBC was conceptualized as individual’s perception of her ability or perception of how easy or difficult it is to use or obtain EC Figures 1& 2. Theoretical Framework of the Theory of Planned Behavior In Tanzania, unwanted pregnancies among young women account for 33% of all pregnancies [17], leading to high cases of unsafe abortion that end up with complications including excessive bleeding and death as a result of applying crude methods, given that abortion is illegal in Tanzania. The practice of terminating unwanted pregnancy among young women is increasing as more women continue to become pregnant despite the availability of the EC. Emergency contraception continues to be critically underutilized [13]; only 2.3% of young women surveyed reported using EC [17]. The reasons for this are not clear. None of the studies conducted in Tanzania have clearly delineated factors influencing uptake of EC among young women. The study aimed at understanding factors associated with low uptake of EC among female undergraduate students in the University of Dar es Salaam using theory of planned behavior (TPB).
The more we understand the factors associated with EC utilization, the more we can improve services and better meet the health care needs of this special population group.
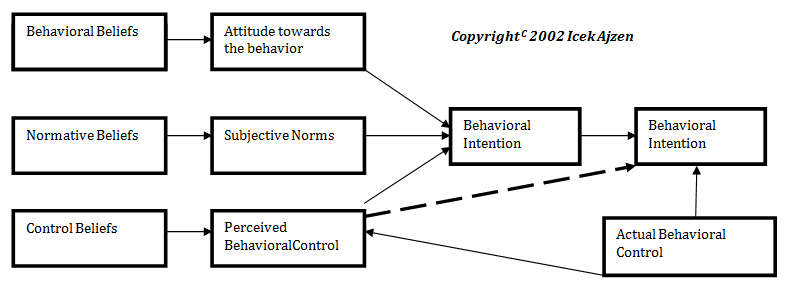
![Figure 2: Modified model showing framework of the Theory of Planned behavior [19].](/fulltextimages/2846/fig_2.png)
Methods
Study Design
This was a descriptive, cross sectional study design that was used to describe and document factors associated with uptake of EC.
Study Setting
The study setting was Main Campus University of Dar Es Salaam. The University has a total of 25 departments; four departments were included in the study (i.e., Political Science, Geography, Sociology and Accounting). Main Campus University had a total of 14,358 undergraduate students in the 2013/2014 academic year and female students constituted 36.7% (5270) of all undergraduate students [20].
Study Population
Study population was female undergraduate students at the University of Dar es Salaam. The enrollment criteria included young women aged 18-24 years, who were present during time of data collection, and consented to participate in the study. This population group was chosen because sexually active young people tend to have sex sporadically which makes contraceptive planning difficult, and they may experience higher rates of contraceptive failure than adults due to inexperience. Many young women have reported experiencing coerced sex; including rape [21]. Students who are new to university life often find themselves in a state of excitement and with more exposure to permissive attitudes toward sexual behavior amongst their peers as many have come from their village in rural area to a more liberal, urban environment. The majority of students live in hostels or other rented accommodations where they experience limited external control of their behavior and suddenly find themselves in a position to make their own decisions and regulate their own behaviors, including unprotected sexual acts with potential for unwanted pregnancies.
Sample Size and Power Calculation
Sample size was calculated using Kish Leslie formula [22]. No previous studies have been conducted among university students on EC in Tanzania. We assumed a 50% prevalence of EC uptake, with a 95% confidence interval and 5% degree error, resulting in an estimated sample size of 384 participants.
n = (Z) 2 P (1- P)
d2 Where: n = the desired sample size Z = Variate from normal distribution (Z 0.025= 1.96) P = Estimated proportional of EC use was 50% as no previous studies have been conducted among University students on EC in Tanzania d = the minimum acceptable errors, which was 5%= 0.05
Recruitment and Data Collection
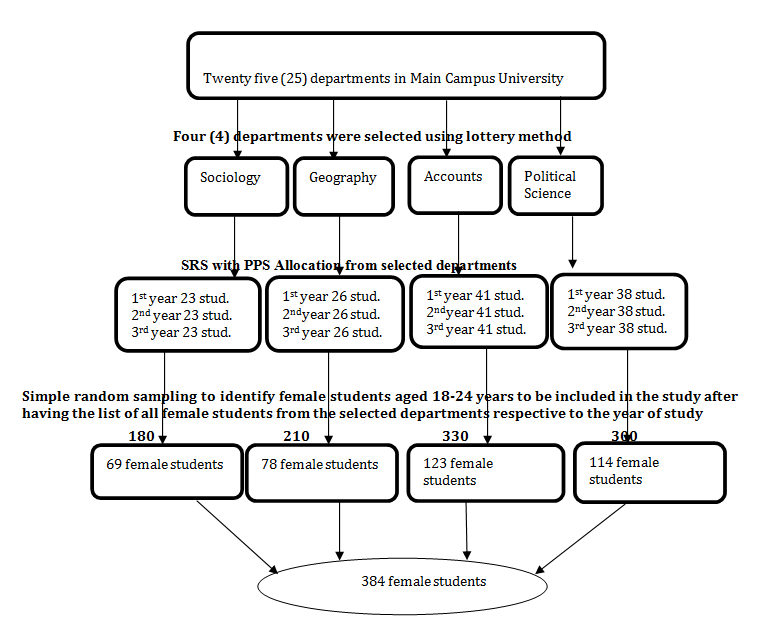
The study enrolled 384 female undergraduate students. A two-stage sampling technique was used; where four (4) departments were selected from the total of twenty-five (25) departments using a random lottery method. Then, the total sample size was allocated to each department proportional to the number of female students in the department. Secondly, study participants were selected from each department proportional to their year of study using simple random sampling technique. The number of study participants from the selected departments was determined using probability proportionate to population size allocation methods depending on the year of study.
Data was collected using a structured self- administered questionnaire with closed ended questions. The questionnaire was adapted to the local situations [2, 3, 23]. The questionnaire was prepared in English and translated to Kiswahili and translated back to English to check its consistency. The questionnaire collected information on behavioral attitude; subjective norms, perceived behavior control, socio-demographic information and behavior (ever/never used EC). Each construct of the independent variables had 6 items. The questionnaire was pre tested to 38 students from DUCE University in Dar es Salaam before using it for actual data collection to check reliability.
Four trained research assistants (registered nurse/midwives) from Muhimbili National hospital who had BSc were used to collect the data after a two days training on the study objectives and data collection instrument. Introduction and proper information about the purpose of the study and rationale for why University of Dar es Salaam was selected to participate was given to students. This was followed by reviewing selection criteria with potential participants, and those who consented to participate in the study were given a questionnaire to respond to the questions (Figure 3).
Data Analysis
Data was coded, entered in the computer by the Principle Investigator. It was then cleaned and analyzed using SPSS version 21.0 computer software package. Following this, factor analysis was first conducted followed by principal component analysis with Varimax rotation. Descriptive statistics were used to describe variables of socio-demographic characteristics, subjective norm, perceived behavioral control and perceived self- benefits. Mean and median were used for independent continuous variables; frequencies and proportions were used for independent categorical variables. Bivariate analysis was carried out to assess the relationship between independent categorical variables and outcome variable using logistic regression analysis. The significant factors in bivariate analysis were subjected to multiple logistic regressions to analyze for independent associations. For both bivariate and multivariate analyses, p-values ≤0.05 were considered to be statistically significant. Unadjusted odds ratios for bivariate and adjusted odds ratios for multivariate and their respective 95% confidence intervals were used.
Ethical Considerations
Ethical clearance was sought from Makerere University School of Health Sciences Institution Review Board. Ethical approval was also obtained from Muhimbili University of Health and Allied Sciences Institution Review Board. A permission letter from administrative office of University of Dar es Salaam was obtained to allow data collection from the University. Participants who agreed to participate in the study were requested to complete the written informed consent form; only those who provided written consent were given the questionnaire. Confidentiality and freedom to withdraw at any time during the study was assured.
Results
Demographic Information
Three hundred and eighty four (384) participants were enrolled, and the majority 272 (70.8%) of the students reported being sexually active. Among those students reporting sexual activity in the previous six months, (n=155), 46 students (30.0%) reported having utilized EC (Table 1).
| Characteristics | Frequency | Percentage (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Department | Geography | 78 | 20.3 | ||||||
| Sociology | 68 | 17.7 | |||||||
| Accounts | 124 | 32.3 | |||||||
| Political Science | 114 | 29.7 | |||||||
| Total | 384 | ||||||||
| Relationship status | In a relationship | 273 | 70.8 | ||||||
| Not in a relationship | 112 | 29.2 | |||||||
| Total | 384 | ||||||||
| Had vaginal intercourse | Yes | 272 | 70.8 | ||||||
| No | 112 | 29.2 | |||||||
| Total | 384 | ||||||||
| Had vaginal sex in the last six months | Yes | 115 | 40.4 | ||||||
| No | 229 | 59.6 | |||||||
| Total | 384 | ||||||||
| Ever used emergency contraception | Yes | 62 | 16.1 | ||||||
| No | 322 | 83.9 | |||||||
| Total | 384 | ||||||||
| Emergency contraception use among those reported to had vaginal sex in the last six months | Used | 46 | 30 | ||||||
| Never used | 109 | 70 | |||||||
| Total | 155 |
Table 1: Socio-demographic characteristics of study participants.
Factor Analysis
The Kaiser–Mayer-Olkin (KMO) that measures sampling adequacy was 0.85 above the commonly recommended value of 0.6, and Bartlett’s test of sphericity was significant (X2(153) =2583, p<0.001). These statistics indicated that correlation between the items were sufficiently large enough for principal component analysis. The results of principal component analysis (PCA) indicated that three scales; perceived self- benefit from EC use, subjective norms and perceived behavioral control had reliable scales and as such were considered for further analysis (Table 2).
- Component Scale
- Cronbach's Alpha
- Perceived self-benefits from EC use
- 0.7
- Will prevent unwanted pregnancy
- Helps prevent pregnancies that would disrupt my studies
- Subjective norms
- Male partner approves use of EC
- My parents approves use of EC
- Important people around me
- 0.88 approves use of EC
- Best most people important to me will themselves use EC
- Friends support my use of EC if necessary
- Perceived behavioral control
- Can always get EC from health facilities when need be
- Can always afford EC
- 0.78
- Can easily obtain EC when need be
- Easy for me to obtain EC
- Can always use if I want
Table 3: Reliability of the scale components from factor
Relationship between Independent Dichotomized Factors and Emergency Contraception Use
As demonstrated in Table 3, relationship status (X2=7.45, 0.006), perceived self-benefits from EC use (X2=7.66, p= 0.006) and perceived behavioral control (X2=15.51, p< 0.001) were significantly associated with uptake of EC.
| Ever used EC | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | X2 | p | -Valu | e | ||||||||||
| Yes n (%) | No n (%) | |||||||||||||
| Age of the participant | ||||||||||||||
| 19 - 20 | 15 (11.5) | 116 (88.5) | 3.24 | 0.072 | ||||||||||
| 21 - 24 | 47 (18.6) | 206 (81.4) | ||||||||||||
| Relationship status | ||||||||||||||
| In a relationship | 53 (19.4) | 220 (80.6) | 7.45 | 0.006 | ||||||||||
| Not in a relationship | 9 (8.1) | 102 (91.9) | ||||||||||||
| Perceived self-benefits from EC use | ||||||||||||||
| ≥ Median | 49 (20.1) | 195 (79.9) | 7.66 | 0.006 | ||||||||||
| < Median | 13 (9.3) | 127 (90.7) | ||||||||||||
| Subjective norms | ||||||||||||||
| ≥ Median | 37 (16.4) | 189 (83.6) | 0.02 | 0.886 | ||||||||||
| < Median | 25 (15.8) | 133 (84.2) | ||||||||||||
| Perceived behavioral control | ||||||||||||||
| ≥ Median | 46 (23.4) | 151 (76.6) | 15.5 | < 0.001 | ||||||||||
| < Median | 16 (8.6) | 171 (91.4) |
Table 2: Relationship between perceived self-benefit, perceived behavioral control, subjective norms, socio- demographic characte
Factors Associated with Uptake of Emergency Contraception
The results showed that variable of relationship status which was significantly associated with EC use in the bivariate analysis lost its statistical significance in multiple logistic regression analysis. The adjusted odds ratio for perceived self-benefit and perceived behavioral control didn’t change much; all remained significant after combining them together. This suggests that students who scored high on perceived self-benefit and perceived behavioral control were found to be more likely to report to have ever used EC (OR=2; 95%CI, 0.98-4.54; p=0.046 and OR=3; 95%CI, 1.52-5.54; p= 0.001) respectively.
Discussion
Results of this study showed that utilization of emergency contraception (EC) was low among students who reported to had vaginal sex in the last six months. This was different from the report of studies among University students in Adama, South Africa and Nigeria [3, 15, 24]. The possible reasons for a low utilization of EC observed in this study might be related to the low proportion of sexually active students in the last six months in the current study compared to (57%) at the University in South Africa and (63%) at the University in Nigeria.
Factors associated with the use of EC in the current study included perceived behavioral control and perceived self-benefit, of which perceived behavioral control (PBC) was the strongest factor associated with utilization of EC. This implies that students use EC if they exhibited strong self-efficacy and perceived ability to control the use of EC as well as if they perceived self- benefits for using EC to be high. Previous studies found similar findings that PBC was more important in predicting people’s intention than other components of theory of planned behavior [23, 25, 26, 27]. The important role that PBC played in this investigation as one of the factors associated with young women’s intention to use EC is likely related to the fact that items for both self- efficacy and controllability were included in the measurement scale. Self-efficacy refers to a person’s perception of the amount of difficulty she will experience when performing a behavior and the degree of confidence she possesses that she can do it. Controllability refers to whether performing the behavior is up to the person or whether factors beyond her control influence her ability to perform the behavior [28]. Measuring controllability was particularly important in this study because the use of EC is a behavior that is not completely under a woman’s volitional control. Study participants identified significant barriers to using EC, despite recent changes in health policies aimed at improving access to all of the family planning methods to all young people including men. Potential barriers include the unwillingness of some health professionals to provide the treatment and problems accessing the medication during the time frame when it is required. Given these barriers, it is logical that perceived self-efficacy and controllability plays a significant role in determining young women’s intention to use EC. This finding is inconsistent with the reports of other studies which showed PBC to be not a significant factor associated with intention to perform a behavior [29, 30, 31, 32].
Perceived self-benefit was another factor that showed significant association with intention to use EC in this study. This finding is similar to a study done among teenagers in the United Kingdom that investigated EC practice and found attitude towards EC use was primarily positive, and the main reason given was to avoid teenage pregnancy. The study further reported that EC use was more socially acceptable than teenage pregnancy [25]. This finding is dissimilar with a report from a study done in Iraq among married women which revealed that perceived benefit/positive belief towards use of contraceptives was not significantly associated with utilization of contraceptives [33]. A possible reason for this finding in the present study could be that study participants were undergraduate University students of whom the majority were in a relationship but not officially married. Most unmarried students know and fear the practical and social consequences of pregnancy during their university years, and therefore may have reported higher perceived benefits of ECuse.
Subjective norms (SN) in this study were not significantly associated with intention to use EC, which is inconsistent with a report of other studies done which showed SN to be the strongest predictor in intention to use contraceptives [27, 31]. Findings of the present study seem to be consistent with the Tanzanian culture as sexuality issues are not discussed openly in the public, making it difficult for parents to discuss issues of family planning with their unmarried daughters. On the other hand, these young women may not be influenced by others in contraceptive behavior because they view their sexual activity as private and confidential. These students practice sex occasionally, and at times their relationships are not stable so their male sexual partners may not be committed to prevention of unwanted pregnancies. This implies that these male partners don’t influence these young women in protecting themselves against unwanted pregnancy as they are not committed to them.
Conclusion and Recommendations
Results of the current study provide insight into the factors associated with intention to use EC among young women. The factors that were found to be significantly associated with intention to use EC were perceived behavioral control and perceived self-benefits, implying that those who reported to have high PBC and perceived self-benefits from EC use were more likely to use EC. However; practice of EC among female youth students was reported to be very low. The finding that PBC was the strongest predictor for intention to use EC in this study indicates that the individualized counseling of young women about effective use of EC may enhance their perceptions of personal ability to be successful. Therefore, public education would be an important step in evaluating whether EC users’ sense of being able to perform the behaviors appropriately increases and if that, in turn, leads to more effective use of EC and eventually reduction of the incidence of unwanted pregnancies occurring among young women. Replication of the study with a more diverse sample in terms of religion, place of residence, ever practiced unsafe sex, type of family planning used after having unprotected sex will be interesting to see how they affect study findings and the predictive capabilities of the Theory of Planned Behavior. We also recommend future cohort study to follow young women over a certain period of time to see if and how they are using EC is recommended as it will lead to the actual screening of behavior. Finally, mixed methods studies can be done utilizing qualitative methods including focus group discussion or in-depth interviews to get more detailed information on factors associated with uptake of EC.
Consent for Publication
Study participants were informed on the dissemination of the finds without disclosing their personal identity and they agreed.
Availability of Data and Materials
The dataset analyzed during the current study are available from the corresponding author on reasonable request.
Competing Interests
The authors declare that they have no competing interests.
Authors’ Contribution
The main author SEM developed the study design, planned and prepared data collection, supervised research assistants during data collection, carried out data analysis, drafted the manuscript. AFM assisted in conception and study design, offered critical comments in the reviewing of the study proposal, analysis, report and manuscript revision. RM assisted in conception and study design, offered critical comments in the reviewing of the study proposal, data collection, analysis, report, and manuscript revision. BJK assisted in conception and study design, offered critical comments in the reviewing of the study proposal and report revision as well as manuscript revision. All authors read and approved the final manuscript.
Acknowledgements
Thanks to Director of Research UDSM for allowing us to conduct this research in University of Dar es Salaam Main Campus. Thanks to all data collectors’ for their assistance for the entire period of data collection. Thanks to William John Walwa who helped us with the whole process of sampling study participants. Special thanks to all the respondents that agreed to participate in this study and may our almighty God bless you all. My sincere gratitude to NORAD’s Program for sponsorship and special thanks to all research assistants and respondents that agreed to participate in this study.
References
-
Guttmacher institute, Abortion reporting (2015) Promoting public health, Not Politics. Policy Review Spring, 18(02).
-
Byamugisha JK (2007) Emergency Contraception among young people in Uganda: User and provider perspectives. Kampala and Stockholm (PHD thesis), pp: 3-78.
-
Tilahu D, Assefa T, Belachew T (2010) Knowledge, attitude and practice of emergency contraceptives among adama University female students. Ethiop J Health Sci 20(3): 195-202.
-
Ministry of Health and Social Welfare. National Road Map Strategic plan (2008). To accelerate Reduction of Maternal, Newborn and Child Deaths in Tanzania, 2008-2015.
-
Tadesse E, Yoseph S, Gossa A (2004) Illegal abortion in five hospitals in Addis Ababa. Ethiopian Medical Journal 32(4): 283-284.
-
Tanzania Demographic and Health Survey (2010). National Bureau of Statistics. Tanzania: Dar es Salaam. ICF Macro Calverton, Maryland, USA.
-
United Nations (2010) Tanzania Delivery as One. Prevent adolescent pregnancies and keep girls in School.
-
WHO (2008) Unsafe abortion: Global and regional estimates of the incidence of unsafe abortion and associated mortality World Health Organization, pp: 56.
-
United Republic of Tanzania Ministry of Health and Social Welfare (2010). National Family Planning Costed Implementation Program: Reproductive and Child Health Section. Tanzania: Dar es Salaam, 2010- 2015.
-
Chandra Mouli V, Camacho AV, Michaud PA (2013) WHO guideline on preventing early pregnancy and poor reproductive outcomes among adolescents in developing countries. J Adolesc Health 52: 517-522
-
(2011) International Consortium for Emergency Contraception: How far have we come? What's new? What's next? 2011. Discussion Forum, held March 2nd-16th.
-
WHO (2018) Family Planning: A Global Handbook for providers. Revised update, World Health Organization, pp: 460.
-
Gemzell Danielsson K, Berger C (2013) Emergency Contraception: Mechanism of Action. Contraception 87(3): 300-308.
-
Byamugisha JK, Mirembe FM, Faxelid E, Gemzell Danielsson K (2006) Emergency contraception and fertility awareness among University students in Kampala, Uganda. Afr Health Sci 6(4): 194-200.
-
Hoque ME, Ghuman S (2012) Knowledge, practices, and attitudes of emergency contraception among female university students in KwaZulu-Natal. PLoS ONE 7(9): e46346.
-
Mamboleo N (2012) Unwanted pregnancy and Induced abortion among female youths: A case study of Temeke District Master’s thesis, Muhimbili University of Health and Allied Sciences.
-
Okonofua F (2006) Abortion and maternal mortality in developing world. J Obstet Gynaecol Can 28 (11): 974-979.
-
University of Dar es Salaam (2013) Office of the Director of Undergraduate studies.
-
Ajzen I (2002) Perceived Behavioral Control, Self- Efficacy, Locus of Control, and the Theory of Planned Behavior. Journal of Applied Social Psychology 32(4): 665-683.
-
University of Dar es Salaam (2013) Office of the Director of Undergraduate studies. Dar Es Salaam, Tanzania.
-
Family Health International. Adolescents and Emergency contraceptive in Developing Countries (2005) HI Working Paper Series No. WP05-01.
-
Kish, Leslie (1968) Survey Sampling. John Wiley & Sons, Inc., New York, London 1965, IX + 643 S, 31 Abb, 56 Tab, Preis 83 s 10(1): 88-89.
-
Wheatley MAM (2007) Young Women’s Attitude towards Emergency Contraception: Predicting Intended Use.
-
Oladapo OT, Adefuye PO, Odusoga OL, Okewole IA (2005) Emergency contraception among female undergraduates in Ogun state, Nigeria. Sexual Health Matters.
-
Bayley J, Brown K, Wallace L (2009) Teenagers and emergency contraception in the UK: a focus group study of salient beliefs using concepts from the Theory of Planned Behavior. European Journal of Contraception Reprod Health Care 14(3): 196-206.
-
Fazekas A, Senn CY, Ledgerwood DM (2001) Predictors of intention to use condoms among university women: An application and extension of the Theory of Planned Behavior. Canadian Journal of Behavioral Science 33(2): 103-117.
-
Fekadu Z, Kraft P (2000) Predicting intended contraception in a sample of Ethiopian female adolescents: The validity of the Theory of Planned Behavior. Psychology and Health 16(2): 207-222.
-
Francis JJ, Eccles MP, Johnston M, Walker A, Grimshaw J, et al. (2004) Constructing questionnaires based on the Theory of Planned Behavior: A manual for health services researchers. Newcastle upon Tyne: University of Newcastle, pp: 42.
-
Armitage CJ, Conner M (2001) Efficacy of the Theory of Planned behavior: A meta-analytic review. Br J Soc Psychol 40(4): 471-499.
-
Albarracín D, Johnson BT, Fishbein M, Muellerleile PA (2001) Theories of Reasoned Action and Planned Behavior as models of condom use: A meta-analysis. Psychol Bull 127(1): 142-161.
-
Trafimows D (2001) Condom use among US students: The importance of confidence in normative and attitudinal perceptions. J Soc Psychol 141(1): 49-59.
-
Craig DM, Wade KE, Allison KR, Irving HM, Williams JI, et al. (2000) Factors predictive of adolescents’ intentions to use birth control pills, condoms, and birth control pills in combination with condoms. Canadian Journal of Public Health 91(5): 361-365.
-
Peyman N, Oakley D (2008) Effective contraceptive use: an exploration of theory-based influences. Health Education Research 24(4): 575-585.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era