Assessment of Knowledge, Attitude and Practice of Health Workers towards Safe Abortion Care Services at Asella Referral and Teaching Hospital, Central Ethiopia
According to World Health Organization safe abortion care include services that are provided by trained health workers, supported by policies, regulations and a functional health infrastructure, including equipment and supplies. Provision of safe abortion to the extent of the law, emergency treatment of abortion complications, provision of post abortion contraception, education and other lifesaving care services are inadequately given the presence of legal, social, cultural and economic impediments. Most of health care providers are not aware of the fact that termination of pregnancy is permitted under certain conditions leading to ranges of inappropriate attitudinal frameworks or mindset implying a major barrier to give the service. The aim of this research was to assess knowledge, attitude and practice of health workers towards safe abortion service at Asella Referral and teaching hospital, Asella town, Arsi Zone, Oromia region, Ethiopia. An institutional based descriptive cross-sectional study design was used to assess knowledge, attitude and practice of health workers towards safe abortion service at Asella Referral and teaching hospital from January 2017 to May 2017. Systematic random sampling technique was used to select 185 health workers. SPSS version 20 statistical software was employed for data entry and analysis. Of the selected subjects, 99(53.5%) were in the age group of 25-29 years with the mean age of 28.45 ± 3.7 years. In this study, 150(81.1%), 126(68.1%) and 127(68.1%) of health workers had good knowledge, positive attitude and good practice towards safe abortion care .Despite the present law is less restrictive and it was found a general positive KAP of health practitioners matching with the abortion law, some areas like antiabortion attitudes, lack of training and service offering facilities, confidentiality and consequences of misinterpreting the law might be still potentially problematic.
Introduction
According to World Health Organization (WHO) safe abortion care include services that are provided by trained health workers, supported by policies, regulations and a functional health infrastructure, including equipment and supplies [1]. Globally, each year an estimated 36 million to 53 million abortions are performed. Of this figure, around 20 million are considered unsafe [2]. In developing countries complications of unsafe abortion causes between 50,000 and 100,000 women's deaths annually [3].
Ethiopia has the fifth highest number of maternal deaths in the world: One in 27 women dies from complications of pregnancy or childbirth annually [4]. There are no universal abortion laws that protect a women´s life and provide the right to safe abortion care [5]. In Ethiopia unsafe abortion is exercised in different risky ways that range from the traditional remedies such as toxic chemicals, insertion of contaminated, unsterilized instruments in to the uterus and swallowing pills from traditional healers [6, 7, 8].
The Federal Ministry of Health (FMOH) has applied a multi-pronged approach to reduce maternal and newborn morbidity and mortality by improving access to and strengthening facility-based maternal and newborn services [9]. As a result, provision of safe abortion to the extent of the law, emergency treatment of abortion complications, provision of post abortion contraception, education and other life saving care services are in adequately given the presence of legal, social, cultural and economic impediments [10].
Methods and Materials
Study Setting
The study was conducted in Asella town which is about 175 KMs Southeast from Addis Ababa, Asella with a latitude and longitude of 7° 57’ N 39° 7’ E with an elevation of 2430 meters. According to figure from the Asella town health office annual reports 2016, this town have a total population of 97,652 of which 49,104(51%) are males and 48,548(49%) are females. The town has 8 urban and 4 rural kebeles [11]
Regarding health facilities of the town there is one referral and teaching hospital owned by the government of Ethiopia and one private owned hospital (Rehoboth), two health centres, 15 private clinics and pharmacies are found.
Asella Referral and teaching hospital had 264 academic staffs, 298 health workers and 695 supporting staffs. There are 71 physicians, 26 specialists, 201 nurses, 30 laboratory professionals and 33 pharmacists [12]. This study was conducted from January 2017 to May 2017 for duration of four months.
Study Design and Period
An institutional based descriptive cross-sectional study design was used to assess KAP of health workers towards safe abortion care services at Asella Referral and Teaching Hospital from January 2017 to May 2017 for duration of four months.
Sample Size Determination
The sample size was determined using a single population proportion formula considering the following assumptions: since there is no study conducted concerning KAP of health workers towards safe abortion care a proportion of 50% of the population was taken, 5% level of significance (α=0.05).
The following formula was used to determine sample size (Equation 1).
n = (Zα/2)²P (1-p) d² Where n= the required sample size Zα/2 = Critical value of z = 1.96 P = proportion of KAP towards safe abortion care service= assumed to be 50% (0.5) D=marginal error= (0.05).
= (1.96)2 x 0.5 x 0.5 = 384 (0.05)2 There are 298 health workers in Asella Referral and Teaching Hospital; since the total population is less than 10,000, we used correction formula to get the final sample size (Equation 2) nf= no
1+ no N
$$ = \frac {3 8 4}{1 + \frac {3 8 4}{2 9 8}} = 1 6 8 $$
Adding 10% for non-respondent, the final sample size
was 185
Data Collection Tool
The study was conducted using self-administered structured questionnaire that was designed by reviewing previous similar studies in such a way that consists all the variables that can meet the objectives of the study. It includes all questions related to knowledge, attitude and practice towards safe abortion. The data was collected by research team members during the regular working hours.
Data Analysis and Quality Control
The data was checked in the field to ensure that all the information if properly collected and recorded. Before and during data collection the information was checked for completeness. SPSS version 20 statistical software was employed for data entry and analysis. All data was coded in terms of numbers. The analysis included checking errors and describing the collected data by numerical summary measure tables, charts and figure. Pre-testing of the questionnaire was done on 19 (10%) of the sample size to ensure the data quality, its clarity, and completeness two weeks prior to the actual data collection, at Rehoboth private hospital in Asella town for individuals with the same inclusion criteria.
Results
Socio-Demographic Characteristics of Study Participants
All 185(100%) selected subjects responded to the prepared questionnaire. Of the selected subjects, 99(53.5%) were in the age group of 25-29 years with the mean age of 28.45 ± 3.7 years. Among study participants majority, 98(53.0%) were married while 83(44.9%) and 4(2.2%) were singles, separated and widowed Table 1.
Regarding their educational level, 133(71.89%) were degree graduates, while the remaining 52(28.1%) had Diploma. Among study participants, 47(25.4%) were BSc nurses, 44(23.8%) were Medical Doctors, while the rest 39(21.1%), 28(15.1%), 16(8.6%) and 11(5.9%) were Diploma nurses, BSc midwives, Specialists and Diploma midwives respectively Table 1.
| S/N | Variables | Frequency N=185 | Percentage |
| 1 | Age | ||
|---|---|---|---|
| 1 | 15-19 years | - | - |
| 1 | 20-24 years | 22 | 11.8 |
| 1 | 25-29 years | 99 | 53.5 |
| 1 | 30-34 years | 48 | 26 |
| 1 | 35-39 years | 15 | 8.1 |
| 1 | ≥40 years | 1 | 0.5 |
| 1 | Total | 185 | 100.0 |
| Mean 28.45 Median 28 Std. 3.776 | |||
| 2 | Marital status | ||
| 2 | Single | 83 | 44.9 |
| 2 | Married | 98 | 53 |
| 2 | Divorced | 2 | 1.1 |
| 2 | Separated | 2 | 1.1 |
| 2 | Total | 185 | 100 |
| 3 | Educational level | ||
| 3 | Diploma | 52 | 28.1 |
| 3 | Degree | 77 | 41.6 |
| 3 | Doctorate degree | 56 | 30.3 |
| 3 | Total | 185 | 100 |
| Occupation | |||
|---|---|---|---|
| 4 | Diploma nurse | 39 | 21.1 |
| 4 | Diploma midwives | 11 | 5.9 |
| 4 | Degree nurse | 47 | 25.4 |
| 4 | Degree midwives | 28 | 15.1 |
| 4 | Medical Doctor | 44 | 23.8 |
| 4 | Specialists | 16 | 8.6 |
| 4 | Total | 185 | 100 |
Table 2: Socio-demographic characteristics of health workers at Asella Referral Hospital, April 2017.
Knowledge of Health Workers towards SAC
In this study, health workers were asked to define abortion and 154(83.2%) were reported that abortion is the termination of pregnancy to be less than 28 weeks from LNMP`, while 27(14.6%) and 4(2.2%) were reported `Abortion is the termination of pregnancy to be less than 20 weeks from LNMP` and `It is termination of pregnancy to be less than 24 weeks from LNMP` respectively. Among study participants almost all, 180(97.3%) were reported places to terminate pregnancy should be equipped health facilities with trained health workers Table 2.
Study participants were also asked about what is required from a woman who request termination of pregnancy due to rape or incest and majority 104(56.2%) were reported those who don`t submit evidences of rape or incest, while the rest 81(43.8%) noticed for termination of pregnancy due to rape or incest should submit evidence of rape or incest Table 2.
Among study participants, 181(97.8%) of them were reported that the provider has to secure on informed consent for and also 174(94.1%) were reported that the health care institution and the health worker who provide the service has an ethical obligation not to disclose the information provided by the woman unless permitted by the women or ordered by a court of low. One hundred sixty four (88.6%) of health workers noticed that referral arrangements for social support and care are an integrated part of overall abortion care Table 2.
In this study, 98(53.0%) of health workers were reported that they provide SAC service to an eligible women within 3 days while, 56(30.3%) were reported 7 days, 18(9.7%) are reported 5 days and the rest 13(7.0%) were reported they don`t know Table 2.
Among respondents, 92(49.7%) of them indicated that woman should not be ill health at time of requesting SAC while, the rest 86(46.5%) reported that woman should be ill health at the time of requesting SAC and 7(3.8%) were reported they don`t know Table 2.
Regarding different method of terminating pregnancy, medical abortion was reported by 51(27.6%) of health workers, MVA was reported by 22(11.9%) and 20(10.8%) were reported they don`t know, while the rest 91(49.2%) were reported all (medical abortion and MVA) as a means of terminating pregnancy Table 2.
Health workers were also asked drugs that are provided for the woman to terminate a pregnancy and majority, 181(97.8%) were reported misoprostol and mifepristone, while the rest reported CAF and gentamycin (1.1%), ampicillin and chloroquine (0.5%), quinine and sulphamethaxazide (0.5%) Table 2.
Study participants were also asked about the preferred surgical method for termination of pregnancies with 12 weeks of gestation and 131(70.8%) MVA, 47(25.4%) were reported dilatation and curettage, while the rest 3(1.6%) reported they don`t know Table 2.
One hundred fifty three (82.7%) of respondents answered that all (Physicians, health officers and midwives) can perform the procedure of Manual vacuum aspiration and 20(10.8%) only Physicians/GPs, 10 (5.4) only midwives can perform the procedure Table 2.
For the enquiry who can perform the procedure of E & C (Sharp curettage) for pregnancy termination? The majority 165(89.2%) of respondents mentioned medical doctor or gynaecologist and 13(7%) of respondents said midwives are responsible to perform this procedure Table 2.
Generally, based on our operational definition a health worker is considered as knowledgably if he/she answered eight or more than eight questions out of the total of 13
questions. In this study, 150(81.1%) of health workers had good knowledge about SAC.
| Variables | Frequency N= 185 | Percentage | |
|---|---|---|---|
| 1 | What is abortion? | ||
| 1 | A. Termination of pregnancy less than 20 weeks | 27 | 14.6 |
| 1 | B. Termination of pregnancy less than 24 weeks | 4 | 2.2 |
| 1 | C. Termination of pregnancy less than 28 weeks | 154 | 83.2 |
| 1 | Total | 185 | 100 |
| 2 | Place to terminate pregnancy | ||
| 2 | A. Equipped health facilities with trained staffs | 180 | 97.3 |
| 2 | B. Non-equipped health facilities without trained staffs | 5 | 2.7 |
| 2 | Total | 185 | 100 |
| 3 | What is requested for woman who terminates pregnancy due to rape or incest? | ||
| 3 | A. Should submit evidence of rape or incest | 81 | 43.8 |
| 3 | B. Should not submit evidence of rape or incest | 104 | 56.2 |
| 3 | Total | 185 | 100 |
| 4 | The provider has to secured on informed consent for the procedure using standard consent form | ||
| 4 | A. Yes | 181 | 97.8 |
| 4 | B. No | 4 | 2.2 |
| 4 | Total | 185 | 100 |
| 5 | Ethical obligation not to disclose the information provided by women | ||
| 5 | A. Yes | 174 | 94.1 |
| 5 | B. No | 11 | 5.9 |
| 5 | Total | 185 | 100 |
| 6 | Referral arrangements for social support and care are an integrated part of abortion care | ||
| 6 | A. Yes | 164 | 88.6 |
| 6 | B. No | 21 | 11.4 |
| 6 | Total | 185 | 100 |
| 7 | Day for termination of pregnancy | ||
| 7 | A. Within 5 days | 18 | 9.7 |
| 7 | B. Within 7 days | 56 | 30.3 |
| 7 | C. Within 3 working days | 98 | 53 |
| 7 | D. I do not know | 13 | 7 |
| 7 | Total | 185 | 100 |
| 8 | Method of terminating pregnancy | ||
| 8 | A. Medical abortion | 51 | 27.6 |
| 8 | B. MVA | 22 | 11.9 |
| 8 | C. Sharp metallic curettage | 1 | 0.5 |
| 8 | D. All | 91 | 49.2 |
| 8 | E. I don’t know | 20 | 10.8 |
| 8 | Total | 185 | 100 |
| 9 | Drug for terminating pregnancy | ||
| 9 | Ampicillin + chloroquine | 1 | 0.5 |
| 9 | CAF + Gentamycin | 2 | 1.1 |
| 9 | Quinine + sulphamethexazide | 1 | 1.1 |
| 9 | Misoprostol + Mifepristone | 181 | 97.8 |
| 9 | Total | 185 | 100 |
| 10 | Preferred surgical method for termination of pregnancies with 12 weeks of gestation | ||
| 10 | A. Dilatation and curettage/D & C | 47 | 25.4 |
| 10 | B. Sharp metallic curettage/E & C | 4 | 2.2 |
| C. Manual vacuum aspiration | 131 | 70.8 | |
|---|---|---|---|
| D. I don’t know | 3 | 1.6 | |
| Total | 185 | 100 | |
| 11 | Who can perform the procedure of E & C (Sharp curettage) for pregnancy termination according the technical and procedural guide line? | ||
| A. Junior nurse or health assistant | 1 | 0.5 | |
| B. Medical doctor or gynecologist | 165 | 89.2 | |
| C. Health officer | 2 | 1.1 | |
| D. Nurse or midwife | 13 | 7 | |
| E. I don’t know | 4 | 2.2 | |
| Total | 185 | 100 | |
| 12 | Who can perform the procedure of Manual vacuum aspiration according the technical and procedural guide line? (more than one choice is possible) | ||
| A. Physicians/GPs | 20 | 10.8 | |
| B. Health officers | 1 | 0.5 | |
| C. Midwives | 10 | 5.4 | |
| D. All | 153 | 82.7 | |
| E. I don’t know | 1 | 0.5 | |
| Total | 185 | 100 | |
| 13 | Who should provide post abortion contraception? (more than one choice is possible) | ||
| A. Physicians/GPs | 11 | 5.9 | |
| B. Health officers | 3 | 2.6 | |
| C. Midwives | 12 | 6.5 | |
| D. Clinical nurses | 1 | 0.5 | |
| E. I don’t know | 158 | 85.4 | |
| Total | 185 | 100 |
Table 4: Knowledge of health workers towards SAC service at Asella Referral Hospital, April 2017.
Among respondents, 92(49.7%) of them indicated that woman should not be ill health at time of requesting SAC while, the rest 86(46.5%) reported that woman should be ill health at the time of requesting SAC and 7(3.8%) were reported they don`t know Table 3.
Health workers were also asked who they think can provide education about legal provision of abortion and 158(85.4%) were reported all (midwives and clinical nurses) can provide while the remaining 18(9.7%), 5(2.7%), and 2(1.1%) were reported physicians, midwives and clinical nurses respectively Table 3.
One hundred fifty (62.2%) of health workers reported that they support the pregnancy to be terminated for a woman with less than or equal to 12 weeks of gestational age following a rape, while 68(36.8%) were reported they don`t support the pregnancy to be terminate and the remaining 2(1.1%) noticed they don`t know Table 3.
One hundred five (56.8%) of health workers reported that they support the pregnancy to be terminated for a One hundred forty four (77.8%) of respondents support termination of pregnancy for women gestational age of <12 weeks if the pregnancy endangers the life of the woman, 37(20%) of the respondents did not support termination of the pregnancy even if the conception endangers the life of the women and 4(2.2%) of the respondents did not give any suggestion Table 3.
In this study, 117(63.2%) were reported they support the pregnancy to be terminated as a solution for a woman under 18 requesting termination of pregnancy for less than or equal to 12 weeks of gestational age at their health facility, while the remaining 64(34.6%) and 4(2.2%) were reported they don`t support the pregnancy to be terminated and they don`t know respectively Table 3.
Generally, based on our operational definition there were seven questions that were dealing with safe abortion care. Out of which four and more than four answers were considered as good attitude. Therefore; in this study, 126(68.1%) had good attitude.
| Variables | Frequency N=185 | Percentage | |
|---|---|---|---|
| 1 | If the continuation of pregnancy endangers the life of the women or child | ||
| 1 | Necessarily be in a state of ill health | 86 | 46.5 |
| 1 | Not necessarily be in a state of ill health | 92 | 49.7 |
| 1 | I don’t know | 7 | 3.8 |
| 1 | Total | 185 | 100 |
| 2 | Provide education of legal provision for abortion | ||
| 2 | Physicians/GPs | 18 | 9.7 |
| 2 | Midwives | 5 | 2.7 |
| 2 | Clinical nurses | 2 | 1.1 |
| 2 | All | 158 | 85.4 |
| 2 | I don’t know | 2 | 1.1 |
| 2 | Total | 185 | 100 |
| 3 | A woman ≤ 12 weeks of gestational age following a rape | ||
| 3 | I support the pregnancy to be terminated | 115 | 62.2 |
| 3 | I don’t support the pregnancy to be terminated | 68 | 36.8 |
| 3 | I don’t know | 2 | 1.1 |
| 3 | Total | 185 | 100 |
| 4 | What is your opinion as a solution for a woman with < 12 weeks gestational age following an incest requesting terminating pregnancy at your health facility? | ||
| 4 | A. I support the pregnancy to be terminated | 105 | 56.8 |
| 4 | B. I don’t support the pregnancy to be terminated | 71 | 38.4 |
| 4 | C.I don’t know | 9 | 4.9 |
| 4 | Total | 185 | 100 |
| 5 | A woman ≤ 12 weeks of gestational age if conception endangers life of woman | ||
| 5 | I support the pregnancy to be terminated | 144 | 77.8 |
| 5 | I don’t support the pregnancy to be terminated | 37 | 20 |
| 5 | I don’t know | 4 | 2.2 |
| 5 | Total | 185 | 100 |
| 6 | Woman under 18 requesting termination of pregnancy for less than or equal to 12 weeks of gestational age | ||
| 6 | I support the pregnancy to be terminated | 117 | 63.2 |
| 6 | I don’t support the pregnancy to be terminated | 64 | 34.6 |
| 6 | I don’t know | 4 | 2.2 |
| 6 | Total | 185 | 100 |
Table 5: Attitude of health workers towards SAC service at Asella Referral Hospital, April 2017.
Practice of Health Workers on SAC
Majority, 165(89.2%) of health workers were reported medical doctors or gynaecologists were responsible professionals to perform sharp metallic curettage, also 153(82.7%) of health workers were reported physicians (GPs), health officers and midwives were responsible person to perform MVA according to the procedure guideline Table 4.
Health professionals were also asked about who should provide post abortion contraception and majority, 158(85.4%) were reported physicians, health officers, midwives and clinical nurses. In this study, 99(53.5%) of health workers were reported that they were not trained for safe abortion or post abortion care, while the remaining 86(46.5%) reported they were trained. Among those health workers who were reported they were trained only 92(49.7%) were practicing it Figure 1.
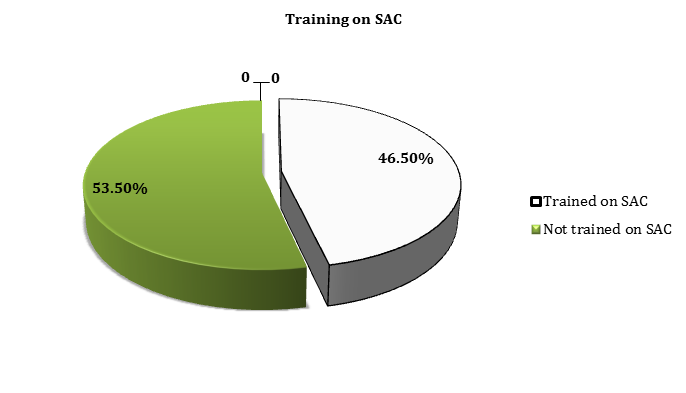
Figure 1: Training on SAC or post abortion care among health workers at Asella Referral Hospital, April 2017 Trained providers didn`t want to perform uterine evacuation service (55.9%), the facility did not offer uterine evacuation service (21.5%), any other reason (12.9%), non-availability of MVA and no women have sought this service (2.1%) were reported as reasons behind not to terminate pregnancy Table 4.
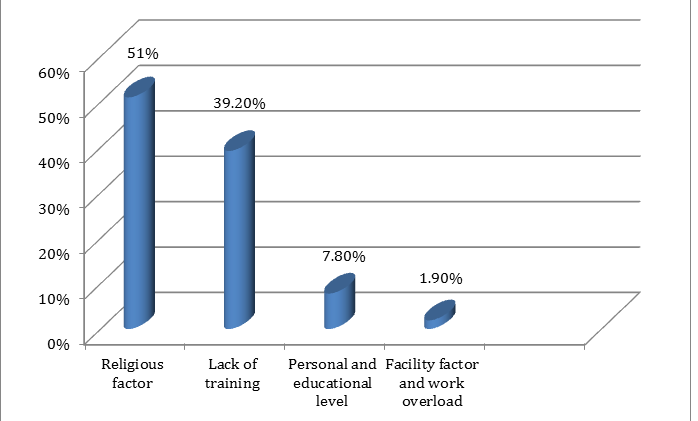
More than half, 102(55.1%) of study participants were reported they ever performed safe abortion care and the reasons behind not performing safe abortion were, due to religious factor (51%), lack of training (39.2%), due to personal and educational level (7.8%) due to facility factor and work overload (1.9%) Figure 2.
Generally, based on our operational definition there eight SAC related questions. A health worker who answered five and more than five questions was considered as good practice. Having been based on this definition 127(68.6%) of health workers had good practice on SAC.
Use of modern contraceptive (76.8%), health education on emergency contraceptive methods(11.4%), avoiding sex if unmarried (7.6%), use of safe abortion service (3.2%), use of traditional/ natural method (0.5%) and give birth once pregnant (0.5%) were information provided as a solution against abortion Table 4.
| S/N | Variables | Frequency N= 185 | Percentage | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Can perform sharp metallic curettage | ||||||||||
| Nurse or health assistant | 1 | 0.5 | |||||||||
| Medical doctor or Gynecologists | 165 | 89.2 | |||||||||
| Health officer | 2 | 1.1 | |||||||||
| Nurse or midwives | 13 | 7 | |||||||||
| I don`t know | 4 | 2.2 | |||||||||
| Total | 185 | 100 | |||||||||
| 2 | Can perform MVA according to the procedural guideline |
| Physicians/ GPs | 20 | 10.8 | |
|---|---|---|---|
| Health officers | 1 | 0.5 | |
| Midwives | 10 | 5.4 | |
| All | 153 | 82.7 | |
| I don`t know | 1 | 0.5 | |
| Total | 185 | 100 | |
| 3 | Training concerning SAC | ||
| Yes | 86 | 46.5 | |
| No | 99 | 53.5 | |
| Total | 185 | 100 | |
| If trained are you practicing it | |||
| Yes | 92 | 49.7 | |
| No | 93 | 50.3 | |
| Total | 185 | 100 | |
| If not practicing it why? (N=93) | |||
| The facility doesn`t offer uterine evacuation services | 20 | 10.8 | |
| No women have sought this service | 2 | 1.1 | |
| Non-availability of MVA instruments | 7 | 3.8 | |
| Trained providers don`t want to perform | 52 | 28.1 | |
| Any other reason | 12 | 6.5 | |
| Total | 93 | 100 | |
| 4 | Performing safe abortion service | ||
| Yes | 83 | 44.9 | |
| No | 102 | 55.1 | |
| Total | 185 | 100 | |
| If performing type of procedure? | |||
| MVA | 39 | 46.9 | |
| Sharp metallic curettage | 3 | 3.4 | |
| Dilatation and curettage | 2 | 2.5 | |
| All (MVA, E and C, and D and C) | 39 | 46.9 | |
| Total | 83 | 100 | |
| Reasons behind not performing SAC (N=102) | |||
| Due to religious factor | 52 | 28.1 | |
| Lack of training | 40 | 21.6 | |
| Due to personal and educational level | 8 | 4.3 | |
| Due to facility factor and work overload | 2 | 1.1 | |
| Total | 102 | 100 | |
| 5 | Is there any information or counseling provided by you about SAC | ||
| Yes | 160 | 86.5 | |
| No | 25 | 13.5 | |
| Total | 185 | 100 | |
| Information or counseling given by providers against abortion: | |||
| Use of modern contraceptive | 123 | 76.8 | |
| Health education emergency contraceptive methods | 18 | 11.4 | |
| Avoiding sex if unmarried | 12 | 7.6 | |
| Use of safe abortion service | 5 | 3.2 | |
| Use of traditional/ natural method | 1 | 0.5 | |
| Give birth once pregnant | 1 | 0.5 | |
| Total | 160 | 100 |
Table 7: Practice of health workers towards SAC service at Asella Referral Hospital, April 2017.
Discussion
Understanding of abortion may be described as a combination of viewpoints on morality, and beliefs on the responsibility, ethical and governmental authorities in public policy. According to the safe abortion care service technical guidelines, abortion is the termination of pregnancy before fetal viability, which is conventionally taken to be less than 28 weeks from the last normal menstrual period (LNMP). In this study, around 83.2%% of the respondents knew the national definition of abortion though around 14.6% of the respondents chose the WHO and other nations´ definition of ”termination of pregnancy in less than 20 weeks” (8). In a study conducted in Mekelle, when the participants were asked about what the definition of abortion was, around 63.3% of them defined it as “termination of pregnancy before fetal viability which is conventionally taken to be less than 28 weeks from the LNMP” (26) our result was higher than a result obtained from Mekelle it may be due to differences in study periods.
In this study more than 97.3% of these study participants knew the SAC guideline in which thought equipped facilities should be the place for termination of pregnancy. The law also required health facilities to have sufficient amounts of basic equipment’s, instruments, drugs and other equipment’s necessary for pre and post abortion related treatments (20). This consistency with the low can partly explained by the fact that most health workers have an access to abortion guide lines in the facilities library where they were working.
Around 56.2% of health workers noticed that SAC service providers would not necessarily require pregnant women to be in a state of ill health. The guideline does not require women to provide evidence for seeking safe abortion service as it is also mentioned in most of the countries that allow safe abortion care without restrictions. Those suggestions from the national and international guidelines strengthen the response of the participants of this study where most (97.8%) of them would provide abortion services without asking the service seeking woman to provide evidence for her claims (8).
The National guideline makes it clear that, provision of safe and high-quality abortion services with a well- functioning referral system is the responsibility of the health practitioners and it also has underlined that the service providers should send the SAC seeking woman to an appropriate service providing place at any time without preconditions. In this study, 88.6% of the participants knew the issue of referral to a woman and would send the woman to other places where she could find well equipped facilities and skilled professionals. The referral centre should also provide all required information to the receiving health facility for an immediate service (24).
According to the SAC guideline women who are eligible for pregnancy termination should obtain the service within three working days. This time is used for counselling and diagnostic measures necessary for the procedure. However; in this study among the health service providers, only 53% of them would offer SAC service within 3 working days.
In this study, 46.5% of health care providers revealed that they were trained for safe or post abortion care, while the rest majority 53.5% did not get the training. The national guideline under the subtitle of provider’s skills and performance” clearly underlines the importance of providing basic knowledge and skills to health providers on regular basis in order to maximize their effectiveness to provide the service and manage abortion and its complications.
In this study, even if 46.5% of health care providers were trained on safe and post abortion care half of them didn`t practicing it. The respondents had mentioned some reasons like absence of evacuation service, lack of MVA instruments, reluctance by providers and other reasons for not practicing SAC in their facility. The guideline also mentioned that the nature of the pregnancy, level of training, type of facility, and presence of essential equipment’s are among the critical requirements needed before the routine of abortion and treatment of its complication begins.
In this study, 70.8% of participants thought MVA were the method to be practiced followed by dilatation and curettage (25.4%) and sharp metallic curettage (2.2%). The national guideline and the Ministry of Health consider MVA as a relatively safer method compared to other methods even though medical abortion and sharp metallic curettage are also practiced.
Concerning the choice of drugs offered for abortion, 97.8% of the health practitioners reported mifepristone and misoprestone as the drug of choice. A study on KAP of health practitioners from Nepal showed a positive role of misopristone and mifepristone for the termination of abortion and introduction of medical abortion in the country (25). According to MoH, the combination mifepristone (200mg) first and misoprostol (800mg)
drugs following 36 to 48 hours after the first drug are used up to nine completed weeks since the LNMP. This is done following diagnosis of the clinical conditions before administrating them.
Conclusions
Knowledge, attitude and practice of health care providers towards SAC were good though there was miss matches of responses concerning the definition of abortion. Those miss defined abortion (16.8%) might need to take the proper training to understand safe abortion.
Even if training practitioners about SAC is mandatory and mentioned by the law in the guide line as a goal only 46.5% of heath care providers take the training, while the majority 53.5% didn`t take SAC training and among those trained, half of them didn`t practicing it.
Since abortion is against some religious and social norms, practitioners might need assurance and evidence to clean themselves from possible assumed consequences. In this study, 43.8% of health care provider’s revealed that they need evidence to practice SAC which was against the law and guideline. The overall observed positive KAP responses of health practitioners that match with abortion issues mentioned by law, some areas like antiabortion attitudes, lack of training and service offering facilities, lack of awareness about the issues of consent, confidentiality and consequences of misinterpreting the law are still potentially problematic for women´s health.
Acknowledgments
First and for most, our special appreciation go to Arsi University, College of Health Sciences, department of Midwifery for providing the chance to pass through this research. Secondly, our gratitude and appreciation goes to sr. Shume Teferi, Gelead Nigatu, Shibre Kasu and Sinafikish Girma for their commitment during data collection and providing suggestions throughout our work. Finally,our special appreciation also goes to Asella Referral and Teaching Hospital Specialists, Medical doctors, midwives and clinical nurses who willingly cooperated during the time of data collection.
References
-
WHO (2013) Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality. 5th (Edn), Geneva, World Health Organization.
-
Mesce D, Sines E (2012) Unsafe Abortion Facts and Figures. Population Reference Bureau.
-
WHO (2004) unsafe abortion: Global and regional estimates of incidence of unsafe abortion and associated mortality. 4th (Edn), Geneva.
-
Dabash R, Pena M, Kolaycz R, Carino G, Mejia M, et al. (2009) How provider attitudes towards abortion can impact the quality of and access to abortion services: An assessment of IPPF/WHR provider Knowledge, Attitude and practice in 6 Latin America and Caribbean countries.
-
Shotorbani S, Zimmerman FJ, Bell JF, Ward D, Assefi N (2008) Attitudes and Intentions of future health providers towards Abortion provision. Perspectives on Sexual and Reproductive Health 36(2): 58-63.
-
Gebreselassie H, Fetters T, Singh S, Abdella A, Gebrehiwot Y (2010) Caring for Women with abortion complications in Ethiopia: national estimates and future implications. Int Perspect Sex Reprod Health 36(1): 6-15.
-
(2010) Walter Leitner International. Ethiopia: US foreign policy and unsafe abortion in Africa.
-
FDRE (2010) Ministry of Health: technical and procedural guidelines for safe abortion services in Ethiopia. Addis Ababa, Federal Democratic Republic of Ethiopia, Ethiopia.
-
(2014) CSA, Ethiopia and orc macro: Ethiopia demographic and health survey. Addis ababa, Ethiopia and Calverton, Maryland, USA: central statistical agency and orc macro.
-
Alemayehu, Tibebu, Karen Otsea, Gebre Mikael A, Dagnew S, et al. Abortion care improvements in Tigray, Ethiopia: using the safe abortion care (SAC) approach to monitor the availability, utilization and quality of services. Chapel Hill, Ipas. NC, USA.
-
(2016) Asella town profile.
-
(2017) Arsi University College of Health Sciences information bulletin.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era