Menstrual Problems among Adolescent Girls and Female Youth in Tamil Nadu
Menstruation, or period, is normal vaginal bleeding that happens as a part of a woman’s monthly cycle. The menstrual cycle is that the hormonal process a woman’s body goes through monthly to get ready for a possible pregnancy. Regular menstrual periods within the years between puberty and menopause are usually a sign that the body is functioning normally. Irregular or heavy, painful periods are not normal. Many women get premenstrual syndrome (PMS) symptoms. It encompasses the foremost common issues, like mild cramping and fatigue, but the symptoms usually get away when the period begins. Menstruation that is too heavy or too light, or the entire absence of a cycle, may suggest that other issues are contributing to an abnormal menstrual cycle. Menstrual hygiene plays an important role in the health of young women. This study focuses on menstrual problems among adolescent girls. The main objectives of the present study are; to find out the awareness regarding menstrual problems among adolescent girls, and to investigate the problems about menstruation among adolescent girls.
Introduction
Menstrual Problems among Adolescent Girls and Female Youth in Tamil Nadu
Menstruation, or period, is normal vaginal bleeding that happens as a part of a woman’s monthly cycle. The menstrual cycle is that the hormonal process a woman’s body goes through monthly to get ready for a possible pregnancy. Regular menstrual periods within the years between puberty and menopause are usually a sign that the body is functioning normally. Irregular or heavy, painful periods are not normal.
Many adolescent girls get premenstrual syndrome (PMS) symptoms [1]. It encompasses the foremost common issues, like mild cramping and fatigue, but the symptoms usually get away when the period begins. Menstruation that is too heavy or too light, or the entire absence of a cycle, may suggest that other issues are contributing to an abnormal menstrual cycle. Menstrual hygiene plays an important role in the health of young women [2, 3].
Girls and women have very less or no knowledge about reproductive tract infections caused due to ignorance of personal hygiene during menstruation time. So, there should be a need to educate and make them aware about the environmental pollution and health hazards associated with them [4]. Girls were unaware and unprepared about the menarche. If knowledge circulates to girls with a systematic way, it would lead towards an effective initiative in order to address menstruation taboos and menstrual malpractices among women in rural areas [5]. Adolescent girls did not change their pads or cloths more than two times during menstruation, and low hygiene practice during menstruation [6]. Menstrual hygiene is essential to decrease susceptibility of urinary and reproductive tract infection and promotes better health of women and health education strategies and awareness programme on menstruation and menstrual hygiene should be framed to promote better health of adolescent girl [7, 8, 9]. Millions of women face significant barriers in menstrual hygiene management due to inadequate awareness, misconceptions and erroneous practices [10].
Menstruation influences every girl, but the experience can differ among them. Medically, menstruation termed as the period or bleeding, is the process in a female youth of discharging blood through the vagina and other materials from the covering of the uterus at about monthly interval from puberty until menopause (stopping of regular menstrual cycles), with the exception of during pregnancy. This discharging process lasts about 3-5 days. Menstruations come regularly; this is known as the menstrual cycle. Having ordinary menstrual cycle is an indication that important parts of our body are functioning normally [11]. The menstrual cycle gives important body chemical substances, called hormones, to keep us healthy. It additionally prepares our body for pregnancy every month. A cycle is checked from the first day of 1 period to the first day of the following period. The normal menstrual cycle is 28 days in length. Cycles can range from 21 to 35 days in adults and 21 to 45 days in young girls. The rise and fall of levels of hormones during the month control the menstrual cycle. The menstrual cycle is a marker of physiologic and reproductive health; its regularity is affected by hormones, stress, and environmental factors. Regular menstrual cycles take 2–5 years to be established in the majority of adolescent girls due to maturation of the hypothalamic-pituitary-ovarian (HPO) axis. After this initialization, disorders of the HPO axis and endocrine system can affect regularity [12, 13]. Teenage girls with menstrual pain regularly present to physicians. The experience of pain with menstruation is common for 70–91% of teenagers. Also, there are a number of physical, psychological and emotional symptoms that occur premenstrual and during menstruation, which are reported by 96% of teenagers [14]. Majority of the girls would seek advice from family members before considering seeking medical advice. Without the support from their family, the girls may be helpless and avoid seeing doctors [15].
The World Health Organization (WHO) defines “adolescents as individuals between 10-19 year age group and “youth” between 15-24 year age group. These two overlapping age groups are combined in the group “young people”, covering the age range of 10-24 years” [16].
In these age groups, some adolescent girls get symptoms leading up to and during menstruation, for example, cramps or pains low in the abdomen, bloating or swelling in the abdomen, constipation before period, diarrhea when the period starts, ache, tiredness and mood changes. Better hygienic practices can be adopted by making sanitary pads accessible at reasonable cost [17]. Mood swings/irritability, water retention/weight gain, lack of energy/mood swings and lack of energy/irritability were common symptoms that frequently co-occurred [18]. The temporal exposure to air pollution in the adolescent and early adulthood window may be especially important, given its association with phenotypes of menstrual irregularity [13]. The knowledge, effective management of menstrual pain and symptoms could reduce menstrual morbidity considerably [14]. In spite of, many studies have examined menstrual cycle, menstrual management, systems, cramps and management periods. Hence, present study carries out following objectives are: (1) find out the awareness regarding menstrual problems among adolescent girls and female youth in Tamil Nadu, and (2) investigate the problems about menstruation among adolescent girls and female youth in Tamil Nadu.
The United Nations understands adolescents to include persons aged 10-19 years and youth as those between 15- 24 years for statistical purposes without prejudice to other definitions by Member States. Together, adolescents and youths are referred to as ‘young people’, encompassing the ages 10-24 years (UNFPA). Table 1 shows that percentage of the adolescent and youth population by social classification in Tamil Nadu districts. The percentage of Adolescent girl’s population is less (8.3 %) than the national average (9.9 %). Among 32 districts of Tamil Nadu, 22 districts are more than the state average (8.3) and 10 districts are less than the state average. The Krishnagiri and Nagapattinam districts are tops with 9.1 % and Erode district is low level (7.3). The percentage of adolescent girls SCs population is less (9.4%) than the national average (10.4%). Among the 32 district of Tamil Nadu, Nagapattinam district (10.5%) is more than the national average and followed by 13 districts are more than the state average. The percentage of adolescent girls STs Population is less (9.4%) than the national average (10.9%). Among the 32 districts of Tamil Nadu, 21 districts are more than the state average (9.4%) and 11 districts are less than the state average. Perambalur district (10.8%) is almost equal to national average. The proportion of adolescent population ranges from 7.3% in Erode to 9.1% in Krishnagiri and Nagapattinam, whereas it variation between these two districts is 1.8%.
The percentage of female youth population is less (8.7 %) than the national average (9.1 %). Among the 32 districts of Tamil Nadu, 14 districts are more than state average and 18 districts are less than state average. Among the 32 districts of Tamil Nadu, Vellore district is more (9.5) than the national and state average. The percentage of female youth SCs population is more (9.6 %) than the national average (9.4 %). Among 32 district of Tamil Nadu, 15 districts are more than state average and 17 districts are less than stage average. Erode district (8.2%) is less than national and state average and four districts (Vellore, Tiruvannamalai, Tiruvarur, and Krishnagiri) are more (10.2%) than national and state average. The percentage of female youth STs Population is less (9.1 %) than the national average (9.5 %). It is observed that percentage of the female youth SC population is more than the national average.
The percentage of Adolescent girl’s population is more (8.4 %) than the state average (8.3 %) in Sivagangai district. The percentage of Adolescent girls SCs/STs population is less (9.1 & 8.7 %) than the state average (9.4 % & 9.4%) in Sivagangai district. The percentage of female youth population is less (8.4 %) than the state average (8.7 %) in Sivagangai district. The percentage of female youth SCs population is less (9.0 %) than the state average (9.6 %) in Sivagangai district. The percentage of female youth STs Population is more (9.5 %) than the state average (9.1 %) and it is equal to national average (9.5%) in Sivagangai district (Adolescent and Youth Demographics: A Brief Overview, UNFPA, A/36/215 annex) (Table A1) [19].
Methods
Participants and Setting
Before carried out the survey, we have decided to conduct a survey about awareness on menstrual problems among adolescent girls and female youth. Hence we discussed with few researchers about where the survey will be done. Some of our friends were recommended that literate people more aware than illiterate people and conduct a survey in educational institutions. Finally, we decided to conduct a survey in the literate community, in this circumstance, higher education institution (Alagappa University, India) has been selected for this survey. The researchers have asked participants about their willingness and those who are willing to participate they have been included in this survey. The researchers have approached more than 250 respondents, but only 70 respondents were accepted. Finally, 50 respondents actively involved in this survey. On an average 1-2 respondents were interviewed in a day.
Interview Schedule
The menstrual problems among adolescent girls interview schedule were designed specifically for this study. The interview schedule was prepared in the Tamil language. The interview schedule took more than 1 hour, sometimes it took 2 hours. A structured interview schedule was chosen.
Face to face interview was conducted in Tamil Language. Nearly 50 questions were asked to respondents, if they do not understand question, the researcher explained questions in a proper manner and also researcher carried a diary to write further information. The interview schedule includes the details of the respondents, demographic details, nutritional food, the pain experienced with menstruation, menstrual cycle, usage of products, sleeping time, and so on. A mixture of question types was used, including single and multiple responses, true/false statements regarding aspects and perceptions on menstruation, open-ended questions were asked. A consent form was given to respondents to take part in this research. The pilot study was conducted among 20 adolescent girls and final interview schedule were modified and finalized with concerned with Head of the Department, Women’s Studies, Alagappa University, India.
Procedure
One day before, researchers have visited and asked respondents about their reliability. After confirmation of the reliability of respondents, the interview time was fixed. Respondents were given appointment to conduct a survey. At that particular time, the researcher could go to meet the respondents. During interview time, both respondents and researchers have switched off their mobile phones. Each and every interview schedule was assigned an identification number.
Data Analysis
After collection of data from adolescent girls and female youth, data were uploaded into A Statistical Package for Social Sciences (SPSS) 20.0 database. Simple frequency data were analyzed. Pie charts were represented in this study and pie charts are represented as self-explanatory.
Ethical Approval
Before carried out survey, the study was approved by the Head of the Department, Department of Women’s Studies, Alagappa University, Tamil Nadu, India, and RUSA.
Results and Discussion
This part discusses results, findings, and observations with menstrual problems among adolescent girls. Demographic data collected from 50 adolescent girls and female youth aged 17-24 years through menstrual problems interview schedule. Table A2 shows that demographic details of respondents and demographic details includes age, location, level of education, type of family, Total number of the family members, and family’s annual income. 48 percent of the respondent comes under the age of 18. The majority of the respondents are living in rural (52%). The majority of the respondents studied up to under graduate (84%). The majority of the respondents live in nuclear family (84%) and 46 percent of the respondents have four members in a family. Nearly 86 percent of the respondents earning income below one lacks as a family’s annual income (Table A2).
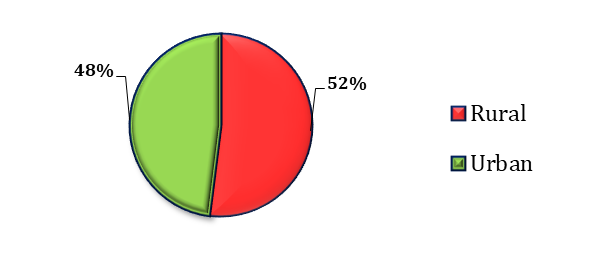
In this study, the respondents have almost equally participated in the location of the rural and urban areas. The above Figure 1 shows that the majority (52%) of the respondents is in rural area and the remaining (48%) of the respondents are in urban areas. In the rural area, respondents are willing to participate in this study on awareness about menstrual problems rather than the urban area respondents. Urban area respondents are educated they have awareness about their health-related issues.
A study said that majority of menstrual practices were significantly better in urban girls are compared to rural girls (P<0.05) and majority of the girls (71.83%) had at least one problem related to menstrual cycles. Thus the study found that there was a significant difference in proportion of menstrual problems in rural and urban girls (P<0.01) [20].
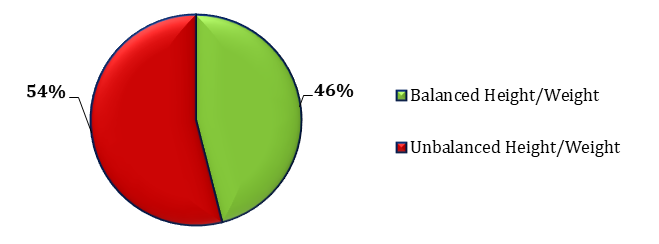
The above Figure 2 shows that the majority (54%) of the respondents are neglecting their meals. Some of the adolescent girls are skipping breakfast at home is prevalent; the likelihood of purchasing food from a restaurant will be high. More importantly, eating too many fast foods and an excessive amount of food intake can also lead to weight gain.
Remaining (46%) of the respondents are having enough height and weight with a balanced diet Most of the girls are conscious about their weight and appearance and tend to reduce their calorie intake to maintain their weight. While some girls enjoy eating varieties of foods, others restrict themselves to just a few sort of food for weight loss or to realize a slimmer figure.
Dietary reference intakes (DRIs) developed by the National Health and Medical Research Council of Australia (NHMRC) provide “current quantitative estimates of nutrient intakes to be used for planning and assessing diets for healthy people, including adolescents”. The important nutrients that need to increase during adolescent period include energy, protein, calcium, and iron. Thus, adolescent girls need a complete diet that gives them the nutrition they need to grow into healthy and strong young women.
Premenstrual symptoms were significantly more common among girls who were overweight, in girls who were eating junk food regularly, in girls who were eating less food (dieting) in order to lose weight and in those who were not doing regular physical activity. Dysmenorrhea was significantly more common in the girls who were dieting to lose weight. Passage of clots was also significantly high in the girls who were dieting [21].
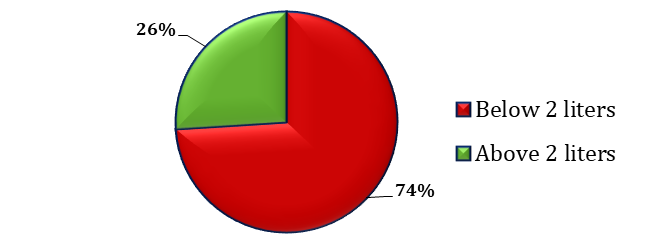
The above Figure 3 shows that the majority (74%) of the respondents is drinking below 2 liters of water daily and remaining (26%) of the respondents are drinking more than 2 liters of water every day.
According to the US Center for Disease Control and Prevention (CDC) [22], “Getting enough water every day is important for our health. Healthy people meet their fluid needs by drinking when thirsty and drinking with meals. Substituting water for one 20-ounce sugar-sweetened soda will save us about 240 calories” [23].
Water is beneficial for menstrual periods. Every human being shall be taken half of the water based on their own body weight in ounces. Therefore, we should drink 60 ounces i.e., 1.77 liters of water a day. It is vital to drink the right amount of water. This will help reduce stress, moody, abdominal pain, and tiredness. Drinking water keeps our body from retaining water and helps to avoid painful bloating during menstruation. Thus, warm or hot water is usually better for cramps, as hot liquids increase blood flow to our skin and may relax cramped muscles during menstrual periods.
Take a warm water bath twice a day during the menses or at least once a day to stay fresh and healthy. Also, rest, exercise, eat healthy foods, eat lots of fruits and vegetables, limit the caffeinated fluids, and drink at least 8-10 glasses of water [24].
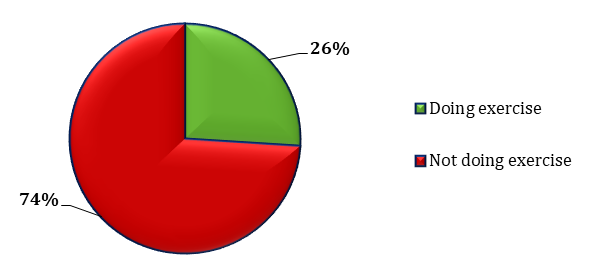
According to the American College of Obstetricians and Gynecologists, “Exercise can help to reduce feelings of depression. So, exercising may help to lift the mood when a person has feelings of sadness, irritability, or anger during their period”. It also provides a range of further health benefits. These benefits mean people should attempt to incorporate exercise into their routine, whether it is during their period or not. There are physical and chemical changes during menstruation that occur in a woman’s body which will be alleviated by exercise. Exercise itself can affect our bodies physically and chemically. Though exercise, we can increase the production of endorphins (“feel-good hormones”) and reduce anxiety, depression, pain, thus improving our mood [25].
Premenstrual symptoms were significantly more common among girls who were overweight, and did not do regular physical activity. There were some studies recognized that there is positive correlation between BMI & PMS. Almost 75% of their subject indicated having physical symptoms, such as breast tenderness, headaches, joint/ muscle pain, bloating and weight gain and overall, 91% had at least one symptom of any degree of severity. In addition, 6.4% reported severe interference of at least one symptom [26, 27].
Exercise is commonly promoted as a therapy for menstrual cramps; it may intervene through increased blood flow, improved metabolism, stimulation of beta-endorphins, and stress reduction [28]. Suggested exercise activities include regular aerobic exercise, nonaerobic exercise, yoga stretching and relaxation, exercise modification across the menstrual cycle [29].
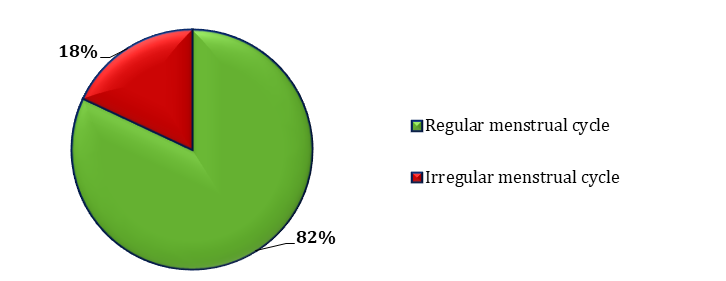
The above Figure 5 reveals that the majority (82%) of the respondents have a regular menstrual cycle. Menstrual flow might occur every 21 to 35 days and lasts two to seven days. For the first few years when menstruation begins, long cycles are commonly occurred. For many girls, bleeding lasts from 4 to 8 days. At that time, hormone levels are very low. The sudden variation in the level of hormone estrogen can make us weak. So, we feel depressed or irritated during the menstrual period.
The remaining (18%) of the respondents have irregular menstrual periods in this study. Their menstrual cycle is shorter or longer than average. This means that the duration from the first day of our first menstrual cycle to the first day of our next menstrual cycle may be less than 24 days or more than 38 days. The following factors are causing irregularities in the menstrual cycle: eating disorders, extreme weight loss, polycystic ovary syndrome (PCOS), premature ovarian failure, Pelvic inflammatory disease (PID) and uterine fibroids. Thus, period problems may also lead to other health problems. Our body transition affects hormonal imbalance, which may increase or decrease the risk for chronic diseases.
A cycle that occurs every 21-35 days in which the flow lasts for 27 days, with an average flow of not more than 80 ml and lot less than 30 ml, is taken to be a normal cycle. A
normal cycle is one which is regular, with an average amount of flow and that which lasts for an average duration of 2-7 days. Any two cycles with duration of more than three months, is labeled as one missed cycle [30].
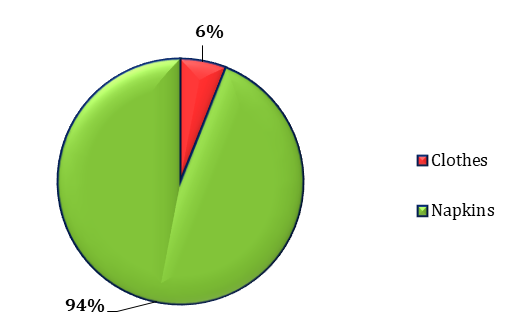
The above Figure 6 shows that the majority (94%) of the respondents is often used napkins during menstruation. They can easily get napkins at many stores, chemist shops, or online. They are expensive, compared to cloth pads, non- reusable, and non-bio-degradable. The cotton which is used in the production of the napkin is not 100% natural and harmful to health. The remaining (6%) of the respondents are using clothes during periods. Generally, rural girls are used menstrual cloths for avoiding irritation and these cloths are reusable, cheaper, easily available, and eco-friendly. However, there is more possibility of getting the infection in the vagina and easily transmitted to the urinary tract and hence hygiene is always important to them. The clothes must be well washed for regular use. Moreover, there is no awareness among the respondents about the tampons and menstrual cups. Tampons are a kind of plug of soft material (cotton) that is inserted into the vagina to absorb the menstrual flow before it leaves the body. It is very expensive, not easily degradable, and not environmentally friendly. On the other hand, menstrual cups may be a new technology for poor women and girls and an alternative to napkins and tampons. It can be worn up to 6-12 hours depending upon the amount of menstrual flow. So, need not be removed and emptied frequently. They are reusable and eco-friendly. Menstruation cups play a vital role when sanitation condition is not good.
The study revealed that the majority of the girls in the rural areas focused on the studies used old cloths as protection, and many reported suffering from various reproductive health problems [31]. Another study reported low use of sanitary napkins from two north Indian villages with only 0.4% of women using market-pads (ready-made sanitary napkins) during menstruation. In West Bengal (India), this study reported involving school going adolescent girls that more than half of the respondents (51.25%) were ignorant about the use of sanitary pads during menstruation. Only 11.25% of girls used sanitary pads during menstruation, 42.5% of girls used old cloth pieces and 6.25% of girls used new cloth pieces. Almost 40% of girls used both cloth pieces and sanitary pads during menstruation and 73.75% of girls reused cloth pieces. Similar findings were observed in Nepal where 66% of respondents used re-usable cloths to absorb menstrual flow during menstruation, the use being significantly higher among rural than urban school girls [32].
Women’s hygiene using a hygienic method of menstrual protection is important for women’s health and personal hygiene. In NFHS-4, young women age 15-24 were asked what method or methods they use for menstrual protection, if anything. In Tamil Nadu, 65 percent use sanitary napkins, 32 percent use locally prepared napkins, 16 percent use cloth, and 1 percent use tampons. Overall, 91 percent of women age 15-24 use a hygienic method of menstrual protection. Women with at least 10 years of schooling are more likely to be using a hygienic method than women with no schooling or less than five years of schooling (International Institute for Population Sciences (IIPS) & ICF) [33].
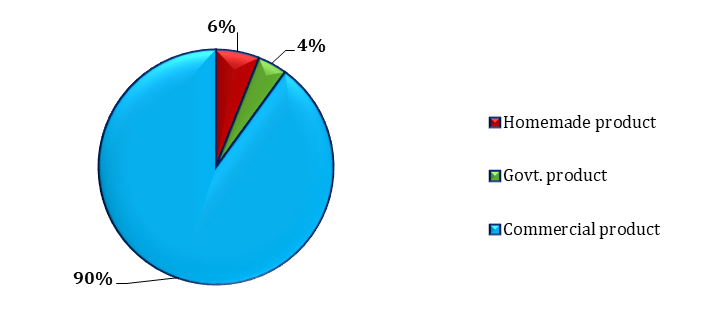
The above Figure 7 reveals that the majority (90%) of the respondents are getting synthetic sanitary napkin from shops that are very harmful to health. These products have evolved from cotton layers held together by a fiber sheet with a waterproof plastic layer at the bottom to prevent staining. A new technique and designs came up, it transformed into ultra-thin sanitary napkins with gel core, to absorb more and provide safety against leaks. Synthetic sanitary napkins are combined with odor neutralizers and artificial fragrances. These cheap chemical components can cause serious irritations, allergy, complications in reproduction, and to the extent of infertility. The effects it can have on the human body are much more serious than just superficial irritation and allergy. It leads to disrupt in hormonal regulatory mechanism and cause cancers like cervical cancer and ovarian cancer. Nowadays, adolescent girls enjoy the ease that comes with the use of synthetic sanitary pads, little do they suspect the impending health treatment that they are being exposed to, is affecting their reproductive health.
The remaining (6%) of the respondents are using the homemade sanitary product, whereas 4% of the respondents are using sanitary napkins produced by Government. These products are fully bio-degradable and chemical-free sanitary pads. It’s a great way to save our bodies and the world. These sanitary pads are made up of sustainable and natural components with minimal or no chemicals.
The study found that significantly more (60.6%) urban girls were using sanitary pad as compared to rural (30.8%) girls (P=0.001) [20]. In this study it was seen that 44.1% used sanitary pad and 21.2% used both cloth and sanitary pad. The use of sanitary pad was higher which was probably due to the fact that the availability was high in these areas and also due to influence of television which has increased their awareness regarding the availability and use of sanitary pads [34].
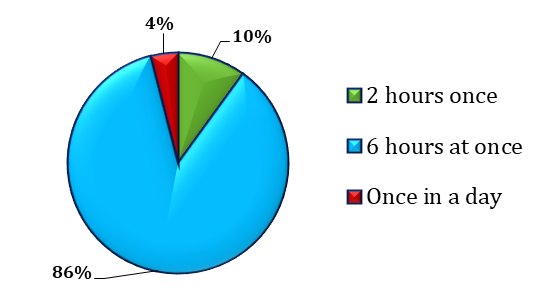
The above Figure 8 indicates that majority (86%) of the respondents are changing their napkins at 6 hours once, followed by 10% of the respondents are changing their napkins at once in 2 hours, and remaining (4%) of the respondents are changing their napkins at once in a day. The standard time for changing the sanitary pad is once in every six hours. But this changing of time cannot be generalized, as it depends on the quality of sanitary napkin products and the need of the individual also.
Therefore, cleanliness of the genital area and access to safe menstrual hygiene products can reduce the incidents of infection by up to 97%. The proper use of sanitary napkins for periods is important to reduce the risks associated with periods. Changing sanitary napkins in every 4 hours and washing hands every time whenever the sanitary napkin is changed, this is such a significant step to ensure good hygiene during periods. Without any discomfort and pain associated with infections, girls can enjoy stress-free periods and continue.
The practice of changing pads during night was mentioned by 79.1% while changing in school or college was less common (20.6%). Majority (78.3%) of the girls changed napkins 2-3 times a day and 16.6% mentioned to change once a day. The hygienic practices were different in girls aged 19 years and above as compared to younger ages [35].
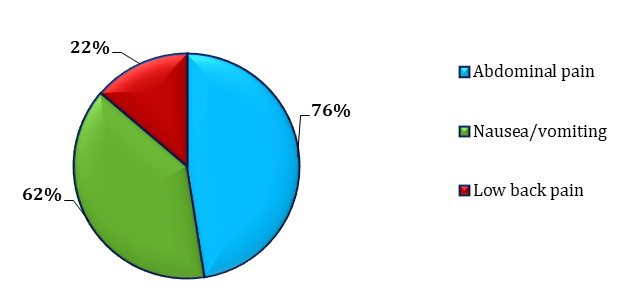
The above Figure 9 shows that the majority (76%) of the respondents is facing the problems of abdominal pain, 62% of the respondents are nausea/vomiting and the remaining (22%) of the respondents are having low back pain.
During menstruation, pain occurs in the lower abdomen and lower back. It usually begins 1 to 2 days before menstruation and lasts from 2 to 4 days. Menstrual cramps can be categorized into two: Primary dysmenorrhea - pain is only associated with the process of menstruation and secondary dysmenorrhea – if the cramping pain is due to certain medical problem such as endometriosis, uterine fibroids, or pelvic inflammatory disease.
The pain can range from light to severe. Emotional stress can raise the chance of experiencing menstrual cramps. Other symptoms contain nausea, vomiting, sweating, dizziness, headaches, and diarrhea. Menstrual cramps can be treated with some home remedies1.
Dysmenorrhea was moderate in 42%, severe in 58%, associated with nausea in 55%, and vomiting in 24%. Of those attending school (n = 66), 46% reported missing one or more days monthly due to dysmenorrhea. Nearly all discussed
1 Applying heat to lower abdomen, massaging with essential oils, drinking herbal drinks such as fennel seeds extract, cinnamon extract, and ginger tea. Most importantly, warm water bathing which will give relief from menstrual cramps and backaches.
their pain with someone; however, a minority sought formal medical care. All used non-pharmacological remedies such as sleeping and heat application. Nearly all used at least one medication, 31% reported using two, and 15% used three medications (not concurrently). Many participants reported using medication at sub-therapeutic doses for pain [36].
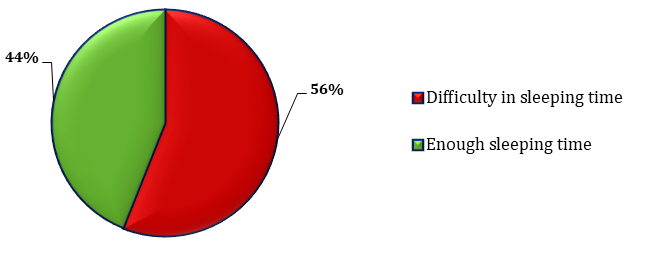
The above Figure 10 reveals that the majority (56%) of the respondents is facing difficulty in sleeping time during the menstrual period and the remaining (44%) of the respondents are having enough sleep. Menstrual problems – cramps, bloating, headaches, heavy bleeding, and pain – can lead to sleep problems like insomnia.
According to therapist Pat Duckworth, “the causes of many problems are down to hormone levels. The levels of estrogen and progesterone vary during the menstrual cycle. Estrogen levels peak around ovulation and then decline before the start of the periods. Progesterone, which can make us feel sleepy, also drops before period – which is the time when women generally have sleep issues” (Catriona Harvey- Jenner, Cosmopolitan UK’s features editor) [37].
Throughout our menstrual cycle, various hormones like estrogen and progesterone fluctuate, which affects our quality of sleep. Estrogen peaks during the follicular phase. This is linked with physical well-being. Progesterone rises after ovulation, some women realize to feel sleepy. Most of the women may feel anxious or depressed before/during their period. Mind-body and relaxation techniques such as deep breathing, yoga, and exercise may help to sleep during the menstrual period. Thus getting adequate sleep helps to promote overall health and to manage monthly symptoms associated with the menstrual cycle.
The study reported long resting hours (29.5%) i.e., bed rest other than normal sleeping hours per cycle attributed to physical discomfort and decreased appetite (22.4%) during menstruation were considered to be disabling and distressing symptoms associated with menstrual cycles [38].
Based on the Observation
Every girl has a different menstrual cycle. If our body is working normally, then it would be regular periods. Female youth are facing irregular, painful, or heavy periods then it becomes a serious health problem. Menstrual cycle is shorter or longer than average, then it is considered as irregular periods. Irregular periods are caused by eating disorders, thyroid problems, high amount of bleeding, polycystic ovary syndrome (PCOS), obesity and chronic stress. In this situation, adolescent girls are not taken proper nutritional food. It can make it harder to get pregnant. Many adolescent girls have painful periods. Pain is the most common problem in their menstrual periods. More than half of the girls who have periods get some pain around their periods. Some girls may get just a feeling of heaviness in the abdomen or tugging in the pelvic area. Other girls experience severe cramps different from premenstrual syndrome (PMS) pain. Few girls may affect heavy periods or heavy bleeding due to thyroid problems, uterine fibroids, bleeding disorders, obesity etc. It may be so painful and heavy that they find it hard to do normal activities. They may experience a range of symptoms that can include fatigue or tiredness that does not get better with rest and sleep, muscle and joint pain.
The most frequently reported problem associated with menstruation was dysmenorrhoea (72.4%) followed by back pain (40.6%) [39, 40, 41, 42]. The other problems reported were fatigue (36.1%), pain in the arms and legs (28.1%) and loss of appetite (18.1%). Headache was reported by 13.9%, vomiting by 6.4% and other minor problems. Only 12.1% of the girls reported that they had no problems/symptoms during menstruation [43, 44, 45, 46].
Case 1: Home Remedies and Reduce Menstrual Pain Suganthi (name changed) aged 34, and she has two daughters. She has been experiencing a period’s pain from the very beginning of her first period at the age of 17. Even though she has a proper menstrual cycle, she cannot control the pain during those days. She has severe mood swings before two days on her period literally. Legs and abdomen scrambling like her bones are going to get out of her skin. She prefers to take home remedies rather than medical treatment and it helps her lot to reduce menstrual pain.
Conclusion
The study found that majority (82%) of the respondents have regular menstrual cycle, 74% of the respondents are not interested to do exercise because they belong to rural communities and engaged in household management like cooking, cleaning utensils, sweeping the house, washing clothes, fetching water from well and carrying to home, caring for animals, etc. and these are related to physical exercises, 90% of the respondents are getting synthetic sanitary napkin from shops which are very harmful to health, 14% of the respondents did not change their napkins at 6 hours once, 76% of the respondents are facing the problems of abdominal pain because they are not willing to take the home remedies for reducing the pain for every month, 56% of the respondents are facing difficulty in sleeping time because they are suffering severe abdominal pain during menstrual period [47, 48, 49, 50]. Hence, it is indicated that women lack awareness about menstruation and have poor hygiene practices during menstrual periods.
Present study focuses on unbalanced diet system, irregular menstrual cycle, lack of awareness on usage of the sanitary napkin, menstrual problems related to physical and emotional well-being and sleeping disorder during menstruation [51, 52, 53]. Few respondents have poor knowledge of menstruation and hygiene practice in the rural areas. This study highlights that there is a need for adolescent girls to have accurate and adequate knowledge about menstruation and its appropriate hygiene practices.
This study is conducted to ascertain the level of awareness on menstrual period among adolescent girls and female youth [54, 55]. The study reveals that knowledge should be developed on menstrual hygiene and protect from harmful diseases among adolescents girls and female youth. Lack of adequate information and awareness among adolescent girls and female youth with respect to menstruation can be due to low level of education among themselves and their parents. Mothers of adolescent girls and female youth were ignorant about informing daughters about menstrual period prior to menarche. Further, they feel shame and it is ugly to talk about periods. All mothers should be taught about discussing with their daughters with regards to menstruation before period of menarche. Better hygienic practices can be embraced by using sanitary napkins.
Moreover, the study observes that school and college teachers have also lack knowledge about sex education and reproductive health. Hence teachers should be educated and trained to impart knowledge about menstruation among students [56, 57]. It is highly recommend that sex education should be incorporated to the school and college curriculum, with the help of Secretary of Health and Family Welfare Department, Secretary of Higher Education Department, Director of School Education, and Experts from various universities. Adolescent girls also gain basic knowledge regarding sex education and reproductive rights. Without this knowledge, most of the adolescent girls either directly or indirectly affected, and they face physical and mental health problems. Knowledge on sex education and reproductive rights can increase the knowledge and to make positive health related decisions. Sexual violence in society can be reduced when they have access to reproductive health services and education. They are less likely to have poor health, and more likely to stay at school and to participate in society. Therefore, there is an urgent need to encourage girls and women to practice safe and hygienic behaviors. The study found that home remedies can be reducing menstrual pain; hence study recommends everyone shall be followed home remedies and avoid medical treatment.
Disclosure Statement
The authors have no conflicts of interest to declare.
Acknowledgement
We acknowledge that RUSA 2.0, Alagappa University for providing financial assistance.
Supporting Information
The following supplementary materials are available for this article: Appendix A: Table A1: Percentage of the Adolescent and Youth Population by Social Classification in India, Tamil Nadu, Districts, 2011 Table A2: Demographic Details of Respondents
References
-
U.S. Department of Health & Human Services (2018) Menstrual Cycle, office on Women’s Health.
-
Raypole C, Nwadike VR (2019) How to Deal with an Unplanned Pregnancy If Abortion Isn’t for You, Parenthood.
-
Ouyang F, Perry MJ, Venners SA, Chen C, Wang B, et al. (2005) Serum DDT, age at menarche, and abnormal menstrual cycle length. Occup Environ Med 62(12): 878- 884.
-
Kaur R, Kaur K, Kaur R (2018) Menstrual hygiene, management, and waste disposal: Practices and challenges faced by girls/women of developing countries. J Environ Public Health 1730964.
-
Pali J, Ahmed A, Mariam T (2019) Discourse of Menstrual Wellbeing in Socio-Cultural Perspective among Adolescent Girls in Rural Rajasthan. International Journal of Social Science and Economic Research 4(2): 801-818.
-
Amgoth D, Reddy RG (2019) A Study on Menstruation and Personal Hygiene among Adolescent Girls. Int J Curr Microbiol App Sci 8(2): 29-34.
-
Johnson J (1988) Level of knowledge among adolescent girls regarding effective treatment for dysmenorrhea. J Adolesc Health Care 9(5): 398-412.
-
Klein JR, Litt IF (1981) Epidemiology of adolescent dysmenorrhea. Pediatrics 68(5): 661-664.
-
Parle J, Khatoon Z (2019) Knowledge, attitude, practice and perception about menstruation and menstrual hygiene among adolescent school girls in rural areas of Raigad district. International Journal of Community Medicine and Public Health 6(6): 2490-2497.
-
Srinivasan D, Agrawal T, Attokaran T, Fathima FN, Johnson AR (2019) Awareness, perceptions and practices regarding menstruation and menstrual hygiene among students of a college in Bengaluru Urban district, South India: a cross sectional study. International Journal of Community Medicine and Public Health 6(3): 1126- 1132.
-
(2019) Menstruation (Menstrual Cycle, Period) MedicineNet.
-
Wang CF, Lasley BL, Lein A, Yen SS (1976) The functional changes of the pituitary gonadotrophs during the menstrual cycle. J Clin Endocrinal Me tab 42(4): 718- 728.
-
Mahalingaiah S, Missmer SE, Cheng JJ, Chavarro J, Laden F, et al. (2018) Perimenarchal air pollution exposure and menstrual disorders. Human Reproduction 33(3): 512- 519.
-
Parker MA, Sneddon AE, Arbon P (2010) The menstrual disorder of teenagers (MDOT) study: determining typical menstrual patterns and menstrual disturbance in a large population‐based study of Australian teenagers. BJOG 117(2): 185-192.
-
Chan SS, Yiu KW, Yuen PM, Sahota DS, Chung TK (2009) Menstrual problems and health-seeking behaviour in Hong Kong Chinese girls. Hong Kong Med J 15(1): 18-23.
-
WHO (1989) Document A42/Technical Discussions/2, World Health Organization, Geneva: The Health of Youth.
-
Devi RU, Sivagurunathan C, Kumar PM (2016) Awareness about menstrual hygiene among adolescent girls in rural area of Kancheepuram District-Tamil Nadu. Int J Pharm Biol Sci 7(1): 267-269.
-
Lete I, Häusler G, Pintiaux A, Jamin C, Nappi RE, et al. (2017) The inconvenience due to women’s monthly bleeding (ISY) survey: a study of premenstrual symptoms among 5728 women in Europe. The European Journal of Contraception & Reproductive Health Care 22(5): 354- 359.
-
Adolescent and Youth Demographics: A Brief Overview, UNFPA - Report of the Advisory Committee for the International Youth Year (A/36/215 annex), pp: 2.
-
Thakre SB, Thakre SS, Ughade S, Thakre AD (2012) Urban-rural differences in menstrual problems and practices of girl students in Nagpur, India. Indian pediatr 49(9): 733-736.
-
Rupa Vani K, Veena KS, Subitha L, Hemanth Kumar VR, Bupathy A (2013) Menstrual Abnormalities in School Going Girls–Are They Related to Dietary and Exercise Pattern? Journal of clinical and diagnostic research: JCDR 7(11): 2537-2540.
-
Centers for Disease Control and Prevention (CDC) (2011) Beverage consumption among high school students--- United States, 2010. MMWR. Morbidity and mortality weekly report 60(23): 778-780.
-
Markus MacGill, Judith Marcin MD (2018) Water: Do we really need 8 glasses a day? Medically reviewed.
-
Aboushady RMN, El-saidy TMK (2016) Effect of home based stretching exercises and menstrual care on primary dysmenorrhea and premenstrual symptoms among adolescent girls. IOSR Journal of Nursing and Health Science 5(2): 10-17.
-
Clennell B (2016) The Woman’s Yoga Book: Asana and Pranayama for All Phases of the Menstrual Cycle. Shambhala Publications.
-
Shivakumar G, Brandon AR, Snell PG, Santiago‐Muñoz P, Johnson NL, et al. (2011) Antenatal depression: a rationale for studying exercise. Depression and Anxiety 28(3): 234-242.
-
Abdella NH, Abd-Elhalim EHN, Attia AMF (2016) The body mass index and menstrual problems among adolescent students. IOSR Journal of Nursing and Health Science 5(4): 13-21.
-
Golomb L, Solidum A, Warren M (1998) Primary dysmenorrhea and physical activity. Medicine & Science in sports & exercise 30(6): 906-909.
-
Sharp BAC, Taylor DL, Thomas KK, Killeen MB, Dawood MY (2002) Cyclic perimenstrual pain and discomfort: the scientific basis for practice. Journal of Obstetric Gynecologic Neonatal Nursing 31(6): 637-649.
-
Patil SN, Wasnik V, Wadke R (2009) Health problems amongst adolescent girls in rural areas of Ratnagiri district of Maharashtra, India. J Clin Diagn Res (3): 1784- 1790.
-
Rajagopal S, Mathur K (2017) Breaking the silence around menstruation: experiences of adolescent girls in an urban setting in India. Gender & Development 25(2): 303-317.
-
Garg R, Goyal S, Gupta S (2012) India moves towards menstrual hygiene: subsidized sanitary napkins for rural adolescent girls—issues and challenges. Maternal and child health journal 16(4): 767-774.
-
International Institute for Population Sciences (IIPS) and ICF (2017) National Family Health Survey (NFHS-4), 2015-16: India. Mumbai, pp: 1-637.
-
Shanbhag D, Shilpa R, D’Souza N, Josephine P, Singh J, et al. (2012) Perceptions regarding menstruation and practices during menstrual cycles among high school going adolescent girls in resource limited settings around Bangalore city, Karnataka, India. International Journal of Collaborative Research on Internal Medicine & Public Health 4(7): 1353-1362.
-
Omidvar S, Begum K (2010) Factors influencing hygienic practices during menses among girls from south India-A cross sectional study. International Journal of Collaborative Research on Internal Medicine & Public Health 2(12): 411-423.
-
O’Connell K, Davis AR, Westhoff C (2006) Self- treatment patterns among adolescent girls with dysmenorrhea. Journal of pediatric and adolescent gynecology 19(4): 285-289.
-
Jenner CH (2017) This is why your period affects your quality of sleep. Cosmopolitan UK’s features editor.
-
Sharma P, Malhotra C, Taneja DK, Saha R (2008) Problems related to menstruation amongst adolescent girls. The Indian Journal of Pediatrics 75(2): 125-129.
-
Pennington VM (1957) Meprobamate (Miltown) in premenstrual tension. J Am Med Assoc 164(6): 638-640.
-
Banikarum C, Chako MR, Kelder SH (2000) Prevalence and impact of dysmenorrhoea on hispanic female adolescents. Arch Pediatr Adolesc 154(12): 1226-1229.
-
Hillen TI, Grbavac SL, Johnston PJ, Straton JA, Keogh JM (1999) Primary dysmenorrhea in young Western Australian women: prevalence, impact, and knowledge of treatment. J Adolesc Health 25(1): 40-45.
-
Ju H, Jones M, Mishra GD (2016) Smoking and trajectories of dysmenorrhoea among young Australian women. Tobacco control 25(2): 195-202.
-
Nair MKC, Chacko DS, Darwin MR, Padma K, George B, et al. (2012) Menstrual disorders and menstrual hygiene practices in higher secondary school girls. The Indian Journal of Pediatrics 79(1): 74-78.
-
Chung FF, Yao CC, Wan GH (2005) The associations between menstrual function and life style/working conditions among nurses in Taiwan. J Occup Health 47(2): 149-156.
-
Fisher M, Trieller K, Napolitano B (1989) Premenstrual symptoms in adolescents. J Adolesc Health Care 10(5): 369-375.
-
Legro RS, Lin HM, Demers LM, Lloyd T (2000) Rapid maturation of the reproductive axis during perimenarche independent of body composition. J Clin Endocrinol Metab 85(3): 1021-1025.
-
Andersch B, Milsom I (1982) An epidemiologic study of young women with dysmenorhea. Am J Obstet Gynecol 144(6): 655-660.
-
Nwadike VR, Raypole C (2019) Why Do I Get Night Sweats During My Period? Healthline.
-
Miyauchi F, Nanjo K, Otsuka K (1992) Effects of night shift on plasma concentrations of melatonin, LH, FSH and prolactin, and menstrual irregularity. Sangyo Igaku 34(6): 545-550.
-
Prior JC (2016) Adolescents’ Use of Combined Hormonal Contraceptives for Menstrual Cycle–Related Problem Treatment and Contraception: Evidence of Potential Lifelong Negative Reproductive and Bone Effects. Women’s Reproductive Health 3(2): 73-92.
-
Wilson CA, Keye WR (1989) A survey of adolescent dysmenorrhea and premenstrual symptom frequency: a model program for prevention, detection, and treatment. J Adolesc Health Care 10(4): 317-322.
-
Manimekalai K (2020) A Mental Health Status of Women at Higher Education Institutions: Evidence from Tamil Nadu. International Journal of Advanced Education and Research 5(6): 47-52.
-
Manimekalai K, Ranjithkumar A (2020) Reproductive Health Status of Indian Women: A Critical Appraisal. International Journal of Science Technology and Society 8(6): 148-153.
-
Sivakumar I, Manimekalai K, Ranjithkumar A (2020) Accessing Public Health Facilities: Rural and Urban Disparities. Journal of Critical Reviews 7(3): 382-388.
-
Sivakumar I, Manimekalai K, Ranjithkumar A (2020) Income and Food Habits on Health Issues among Rural Women in Tamil Nadu. International Journal of Advanced Science and Technology 29(9): 1536-1541.
-
Ranjithkumar A (2018) Inclusive Policy and Women Development: An Indian Experience. Desh Vikas 4(4): 161-168.
-
Manimekalai K, Punitha PS, Veeramani P (2020) Infertility: An Alarming Situation In India. International Journal of Scientific & Technology Research 9(2): 2606- 2609.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era