Postmenopausal Osteoporosis Awareness & Management in Women-An Indian Perspective
Postmenopausal osteoporosis affects millions of women each year jeopardising their healthcare and quality of life. Initial treatment is based on many factors including T-score, fracture risk assessment tool score, and risk factors for fractures. The most recent additions to treatment are aimed at those who are considered to be at higher fracture risk. The newest FDA-approved medications, abaloparatide and Romosozumab that work to increase bone formation in 18 and 12 months, respectively. Due to lack of awareness in Indian women and with the increase in life expectancy as proved by recent studies, it’s important to find out new medications and better lifestyle options for better management of Postmenopausal osteoporosis to help avoid fragility fractures and improve the quality of life of the Indian women.
Background
Menopause is the time of cessation of the menstrual cycle in women. The development of ovaries decrease and a natural decline is observed in the sex hormones. This period may be related to an expansive assortment of indications influencing the urogenital and circulatory frameworks, as well as hair, bone and skin. The sum of Bone cells amassed by the conclusion of the moment decade and remains more or less consistent up to the time of menopause. The lack of sex hormones like estrogens, results in too quickened bone resorption and replacement, a negative adjust and micro- architectural weakening, which compromises with bone quality, as a result of that bone fragility increases, that leads to risk of fracture.
Currently, it is estimated that over 200 million people worldwide suffer from this disease [1]. By the age of 80, it is computed that half of trabecular bone will have been lost. Normal menopause happens between the ages of ‘45 and 54’ years everywhere on the world. This age doesn’t seem to have changed fundamentally throughout the long term. Interestingly, since the center of the nineteenth century, future, especially in ladies, has expanded impressively, with most ladies living to the age of 80 years or more in numerous locales of the world. This implies that at 50 years old years, a lady will live for over 30 years without bone assurance by sex hormones. This speaks to more than 33% of a lady’s life. At 50 years old years, the lifetime danger to encounter a crack is about half (i.e., one out of two ladies will have a break during this period. In India, the prevalence of osteoporosis in postmenopausal women in various studies varies between 25% and 62% [2]. In 2008, it was assessed that in excess of 700 million ladies were more seasoned than 50 on the planet. This number should arrive at 1.2 billion by 2030.
Osteoporosis is the most common metabolic bone disease in humans. According to the 1993 International
consensus, osteoporosis is defined as a systemic skeletal disease characterized by low bone mass and micro- architectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture [3]. Osteoporotic cracks, for the most part, incorporate vertebrae, proximal femur, lower arm and proximal homers. The quantity of breaks of the proximal femur is relied upon to increment fourfold by 2030. In the book “Bone Formation and Repair”, published in ‘1994’, W.C. Hayes declared: “If the prevalence of hip fracture continues to rise at current rates, it may well be that in the next few decades, orthopaedists will do little else but treat this problem”. This explains, how much osteoporosis threatens the well – being and quality of life for women with postmenopausal osteoporosis. There are a variety of factors involved in osteoporosis that can be classified into variable and constant factors, such as genetic factors and environmental factors. They could make a major contribution to the loss of bone mass contributing to osteoporosis, either individually or in synergy. Latest research studies suggest that factors associated with unhealthy living habits are also one of the most significant factors leading to postmenopausal women’s rapid loss of bone mineral density.
Menopause results from a gradual decrease in ovarian function, resulting in low levels of ovarian-generated estradiol and other hormones. Some women develop moderate to severe symptoms at mid-life due to these hormonal changes. Many variables, such as menopausal status, lifestyle, geographic variation, and attitude towards menopause, can affect the frequency and severity of symptoms encountered by an individual woman.
Studies show that, general knowledge about bone health, daily dietary calcium intake, etc. is very low among Indian women. There was a study designed to find out about how much knowledge of osteoporosis is contained or known by educated women, and the researchers found out that, in general, the knowledge about osteoporosis was insufficient among women. So there arose a basic want or idea, for increased involvement of healthcare professionals like doctors, nurses, pharmacists, in education about bone health. Hence, calcium in low levels in the body, with existence of nutrient D insufficiency, in together have put a very deranged, sad information about osteoporosis, and drastically increasing cases of osteoporosis in India are a portion of the reasons that have brought about osteoporosis turning, into a significant general medical issue in India, particularly among the Indian women. As the incidence of bone fractures is increasing drastically in postmenopausal women affecting their health and quality of life, there is a need to create an environment of awareness in not only Indian women but also healthcare practitioners. Could there be better management of postmenopausal osteoporosis in India? How can a cost-effective treatment be devised for women suffering from postmenopausal osteoporosis? Is there a possibility that lifestyle changes in early years can help avoid this? In this review article we aim to explore the various factors that put Indian women at risk for postmenopausal osteoporosis. We also aim to draw attention towards the lack of awareness related to this disease in India and different ways in which there can be better management of post-menopausal osteoporosis.
Epidemiology & Diagnosis of Postmenopausal Osteoporosis
Studies have now proven that there has been a rise in the life span of Indians. Also a disturbing rise of clinical osteoporosis has been noted in the number of women in India. While the information on the predominance of osteoporosis among ladies in India originates from examines directed in little gatherings spread the nation over, gauges propose that of the 230 million Indians expected to be beyond 50 2015 years old in 2015, 20% are osteoporotic ladies [4]. The lifetime risk of any fracture occurring in women from the age of 50 years is more than 40%. Refer to Figure 1.
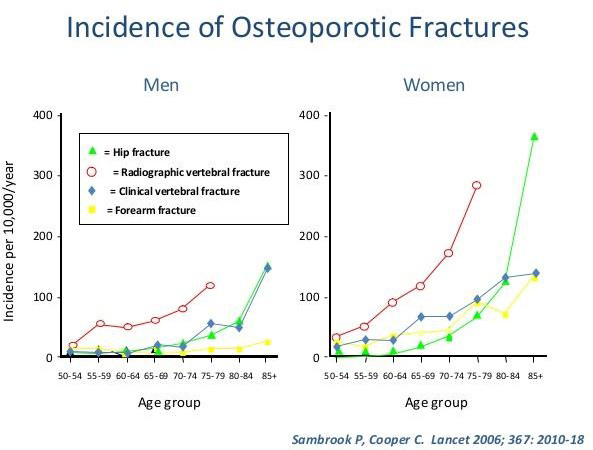
There is variety among people in the danger of crack at various locales at 50 years old. In ladies the leftover lifetime danger of any break at 50 years old years was 46.4% contrasted and only 22.4% for men. In ladies, the danger of hip crack was the most elevated, trailed by the lower arm, vertebral and proximal humerus breaks. In men, the example is comparative; however, there are more vertebral breaks than lower arm cracks.
If you conclude the studies conducted in India related to osteoporosis in women you’ll find out that about 62% Indian women out of the whole population have shown signs and symptoms of postmenopausal osteoporosis. The table below is a compilation of such different articles (Table 1).
| The Main Study | Main Findings / Results | |
|---|---|---|
| AS Babu [5] | N = 609(538 females, 71 males) Average age =52 yrs.[QUS] | Normal = 7.2 % Osteopenia = 40.6 %Osteoporosis =42.2 % |
| Paul TV [6] | N = 150(ambulatory postmenopausal women) Age = ≥ 50 yrs.[DXA] | Osteoporosis at: spine = 48 %,femoral neck = 16.7 %, at any site = 50 % |
| Sharma S [7] | N = 158 women Calcaneal [QUS] | b/w. 55-64 yrs.: Ope = 36.79 %; Opo = 20.25 % after 65 yrs:100% |
| Shatrugna V | N = 289women Age = 30 to 60 yrs [DXA] | Normal = 19 % Osteopenia = 52 % Osteoporosis = 29 % |
| Gandhi AB | N = 200 women Age = >40 yrs [DXA] | Age 40-65 yrs: Osteopenia = 34 %; Osteoporosis = 8 % Age > 60 yrs: Osteopenia & Osteoporosis = ~ 100 % |
| Aggrawal N | N = 500 postmenopausal women Mean age = 57 yrs [DXA] | Osteoporosis at hip = 15.8 %; Osteoporosis At spine = 28.6 % Age above 81 yrs: Osteoporosis in 66.7 % |
| Pande KC | N = 261 women Age = 50 to 79 yrs [Digital x-ray radiogrammetry] | Low bone mass = 50 % |
| Meeta [8] | N = 376 postmenopausal women [DXA] | Osteoporosis at Total hip = 4.2%; at spine = 22.07% Osteopenia at Total hip =17.82%; at spine = 35.11 |
| Nikose | N = 3532 Mean age = 29.32 ± 9.8 [QUS] | Normal= 32.07% Osteopenic = 35.78% Osteoporotic =32,13% |
| Kaur | N = 250 post-menopausal women Age range = 45 to 80 yrs [DXA] | Osteoporosis = 26.4% |
| Shaki | N = 1400 peri- and post-menopausal women Age range= 23 to 50 yrs [QUS] | Osteoporosis in 81% Osteopenia in 19% |
Table 1: Indian Studies on prevalence of osteoporosis. “QUS”Quantitative Ultrasound,” DXA” Dual energy X-ray absorptiometry, “Ope
Postmenopausal osteoporosis is likewise possible to emerge as an extra common within side the many years in advance because of the lifestyles expectancy of the populace increases. The private and financial freight of post-menopausal osteoporosis effects from osteoporotic fractures, which might be a large public health problem, ensuing in considerable morbidity and mortality.
Osteoporosis can expand, if undetected, till a fracture occurs. Any bone may be affected, however fractures of the hip and backbone are of unique concern; hip fractures due to the fact they almost usually bring about hospitalization and most important surgery, main to impaired mobility that may be extended or permanent, and might even bring about death, whilst vertebral fractures can cause lack of height, intense backache, and deformity and also are related to increased mortality in Indian osteoporotic patients and have been accounted for to happen a whole lot sooner in Indians contrasted with individuals in the West (Figure 2). The Delhi Vertebral Osteoporosis Study (DeVOS) revealed a predominance of 17.1% of vertebral breaks among the 415 females subjects (age >50 years) joined up with the study [9]. Hip crack rates were accounted for to be 159/100,000 ladies beyond 50 years old years in Rohtak region, North India [10].
Pathogenesis
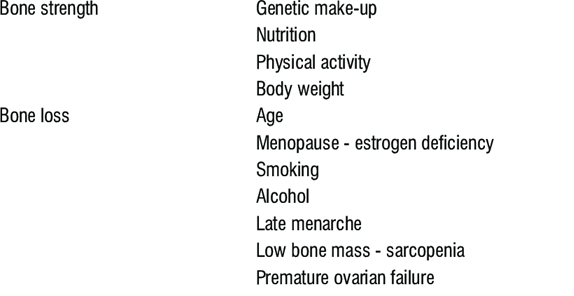
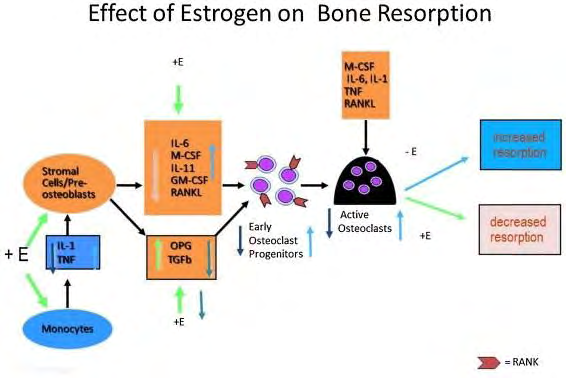
Some of the main reasons for a fragile skeletal system can be because: a. When the body fails to form a skeleton that contains the right amount of mass and strength during growth b. When there is a gradual decrease in bone mass leading to deterioration of the skeletal system mainly due to excessive bone resorption c. Due to inadequacy in formation of bones cause of drastic bone resorption phenomena during bone remodeling Estrogen deficiency to begin with, proposed to be the only mechanism via way of means of which bone mass decreases in postmenopausal women and aged men. The pathways worried in this encompass the differential consequences of estrogen on osteoblast/ osteoclast apoptosis, inflammatory cytokine-mediated growth in osteoclast, and hobby and absence of estrogen-brought on suppression of hypoxia- inducible element 1 alpha protein, main to osteoclast activation [11]. However, current research display that growth in follicle-stimulating hormone ranges additionally contributes to the imbalance among bone formation and resorption via way of means of messenger RNA expression of genes consisting of receptor activator of nuclear element kappa B (RANK), tartrate-resistant acid phosphatase, matrix metalloproteinase-9, and cathepsin K in a dose-dependent manner, thereby growing osteoclastic hobby [12]. Figure 3 below depicts the pathogenesis of postmenopausal osteoporosis [13].
Risk Factors and Causes of Postmenopausal Osteoporosis
Various elements are worried within side the etiology of osteoporosis amongst Indian women. The non-modifiable elements consist of – “sex, advancing age, ethnicity, and genetic elements”. Women whose body frame are smaller in size, are much more expected to have decreased quantities of calcium-wealthy ingredients and for socio-cultural motives are possibly to have terrible daylight publicity. Further, estrogen being crucial for the development & growth of bone in ladies, reduced intervals of exposure to estrogen all through a woman’s lifetime might also additionally make contributions in a first-rate manner to the improvement of osteoporosis [14]. Though the common age at menarche in Indian ladies is 12.5 years, age at menopause is frequently in advance than that visible in Caucasian ladies [15]. This has been mentioned to be a big threat thing for the improvement of osteoporosis in Indian women [16]. Numerous research have mentioned the growing occurrence of osteoporosis with advancing age, and this fashion was discovered to a terrific quantity amongst Indian ladies than men.
Genetic elements, race, ðnicity additionally have completely sturdy impact on height bone mass. Asian Indian ladies were proven to have decreased BMD than their Caucasian and Black counterparts [17].
Evaluation for Osteoporosis
Assessment of osteoporosis includes evaluation of risk factors that may adversely affect bone health, biochemical assessment, radiological imaging, and fracture risk assessment tools. The dangerous elements that result in bone loss were defined already.
Biochemical Assessment
Biochemical assessment includes albumin-corrected overall serum calcium, phosphate, alkaline phosphatase, creatinine, 25 -hydroxyl vitamin D (now no longer mandatory), and parathyroid hormone (PTH) (in decided on cases). In
addition, in decided on cases, secondary reasons along with Cushing syndrome, number one hyperparathyroidism, and a couple of myelomas want to be dominated out.
Bone Turnover Markers
Bone turnover markers (BTMs) are biochemical markers used for the assessment in addition to the tracking of remedy for osteoporosis. They are dependable and cost-powerful in maximum scientific settings. Bone remodelling is maintained with the help of a process, in which there is coupling of formation of the bone and resorption at diverse timelines, which leads to non-stop transforming of bone. Studies related to this topic show the dynamics of bone remodelling in lots of metabolic bone problems primarily based totally at the growth or lower within side the bone formation/resorption markers. They are beneficial within side the estimation of fracture danger and tracking the adherence and reaction to therapy. However, the BTMs are subjected to diverse pre- analytical and analytical versions of strict pattern series and assay strategies at the side of utilizing ethnicity-primarily based totally reference requirements for unique populations [18]. Biochemical markers of bone metabolism are widely divided into markers of bone formation and markers of resorption.
Dual-Energy X-Ray Absorptiometry Scan
BMD evaluation via way of means of (DXA) i.e. Dual- energy X-ray absorptiometry experiment (Figure 4) is the gold standard, for analysis of osteoporosis. It offers an estimate of the amount of bone gift at numerous websites and is the usual degree for osteoporosis. It is an exceedingly correct X-ray method used for the dimension of BMD at skeletal web sites which includes lumbar spine, hip, and wrist. Bone BMD measured via way of means of DXA is expressed as g/cm2. However, via way of means of the convention, the rating then is transformed to a T-rating and a Z-rating. • T-rating: Refers to the number of popular deviations below or more than the Bone Mineral Density of matched controls, according to their age.
• Z-rating: Refers to the number of popular statistics above or below the basic Bone Mineral Density of the younger everyday geometric mean.
According to World Health Organization criteria, osteoporosis is defined as T-score ≤−2.5 (Table 2). Z-score of ≤−2 is defined as low bone mass or bone mass below the expected range for age (this term is used in women.
| Definition | Score |
| Normal | T-score above (i.e., better than) —1.0 |
| Osteopenia or low bone mass | T-score between —1.0 and —2.5 |
| Osteoporosis | T-score below (i.e., worse than) or equal to —2.5 |
| Severe osteoporosis | T-score below —2.5 with fragility fracture |
Table 2: Low bone mass or bone mass below the expected range for age.

Limitations of Dual-Energy X-Ray Absorptiometry Scan
Although BMD is presently the gold well-known degree of osteoporosis, many sufferers with fractures are discovered to have BMD in the osteopenia/ordinary range [19]. Thus, an ordinary BMD cannot rule out the opportunity of osteoporotic fracture. In addition, notwithstanding BMD getting used as a degree of assessment of remedy efficacy in medical practice, research has proven that there’s a terrible correlation between the growth in BMD with antiresorptive remedy and the volume to which the remedy decreases fracture risk [20]. In India, the quantity of DXA scanning facilities is constrained and a maximum of them are positioned in city areas.
Fracture Risk Assessment Tool (FRAX)
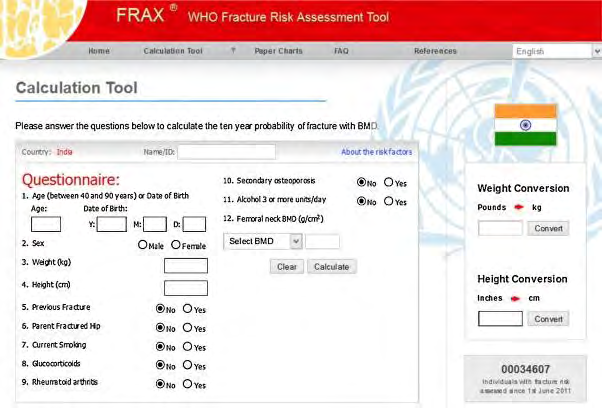
FRAX is the most broadly used fracture risk evaluation device that takes under consideration 9 elements, specifically age, BMD, body mass index (BMI), earlier fragility fracture, use of oral glucocorticoids, parental records of HF, modern smoking, alcohol intake, and rheumatoid arthritis (Figure 5). It predicts the 10-yr probability of HF and major osteoporotic fracture (MOF) [21]. A threshold of >20% for MOF and >3% for HF is taken into consideration the intervention threshold for beginning for osteoporosis.
The major goal of the usage of the FRAX device is to permit scientific experts to become aware of the ones sufferers who could gain from pharmacological remedy in lowering fracture danger. However, like another medical device, FRAX has few limitations. It does now no longer embody all of the crucial elements which can expect fracture danger in a given person consisting of bodily activity, Vitamin D deficiency, chances of all evaluation, BTMs, or the price of bone loss on sequential BMDs. FRAX additionally wishes validation for determining thresholds (of MOF and HF) primarily based totally on ethnicities [22].
Who to Screen for Osteoporosis?
The following patients want to be screened for osteoporosis via way of means of DXA primarily based totally on the advice via way of means of the Indian Menopause Society (IMS) [23]
- All postmenopausal girls more than five years of menopause
- Postmenopausal girls <5 years of menopause with risk factors (Low BMI, glucocorticoid use, alcohol, smoking, rheumatoid arthritis, previous records of fragility fracture, and parental records of HF)
- Menopausal women that are transitioning with secondary reasons
- When a proof as per radiology for - osteopenia and/or presence of - vertebral compression fracture is noticed
- Women suffering with fragility break or fracture
- Earlier ideally, before beginning pharmacotherapy for women detected with osteoporosis.
Who to Treat for Osteoporosis?
According to the IMS, the remedy of osteoporosis is indicated within side the following situations:
- Presenting with fragility fractures
- On the diagnosis of osteoporosis that is mainly based on results after DXA scan, i.e., T- score ≤-2.5 for areas of hip, spine along with other reasons & more risk of fractures
- In the absence of Bone Mineral Density measurements via way of means of DXA, for treating postmenopausal women, intervention is individualized, knowledge and thinking about the value gain and chance gain results of the intervention.
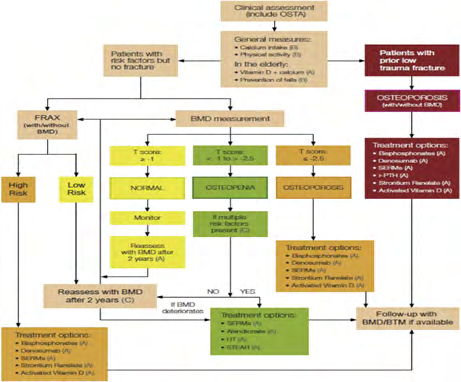
This flowchart below is an algorithm devised to detect and treat post-menopausal osteoporosis.
Awareness About Post-Menopausal Osteoporosis Among Women
Osteoporosis reasons the bones to be fragile and will increase susceptibility to fracture in spite of trivial trauma. Prevalence of osteoporosis in apparently healthy adults above 40 years of age in Pune City, India [42] after attainment of menopause in women, the manner of osteoporosis is elevated with the aid of using estrogen deficiency. Estrogen facilitates in retaining (Figure 6) nice calcium stability and in osteogenesis.
Menopause speeds up the fee of bone loss with the aid of using 2%–5% in line with year, and this could keep for the subsequent 10 years. In a current study, the superiority of osteoporosis in ambulatory postmenopausal girls becomes proven to be 50% at any site. The 1-12 month’s mortality after osteoporotic hip fractures is envisioned to be approximately 20% [6]. The fundamental requirement for coping with any persistent fitness disease begins off evolved with assessment of the notice approximately the ailment a few of the goal subjects.
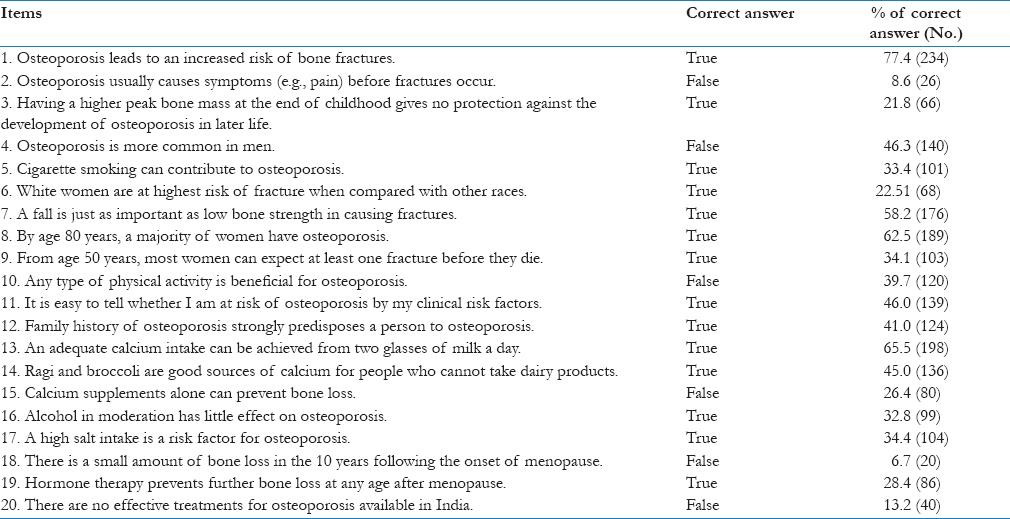
Although an awesome expertise of the ailment won’t be enough to result in modifications in fitness-associated behaviour, good enough know-how is a prerequisite for the fulfillment of preventive efforts. There is proof suggesting that know-how approximately osteoporosis is a contributor to osteoporosis preventive behaviour, even though this isn’t always a clear-reduce relationship. In India, attention of osteoporosis is low, seeing that there was surprisingly little attempt to publicize the ailment. Although few surveys indicate that recognition approximately the disorder within side the city populace is inadequate, there aren’t any large-scale surveys undertaken to evaluate the intensity of recognition and expertise of osteoporosis in postmenopausal girls. Since osteoporosis is a giant hassle in Indian postmenopausal girls with giant growth in morbidity and mortality following fragility fractures, it’s far in reality vital that they be screened pre-emptively for the presence of osteoporosis. Very often, screening efforts are hampered via way of means of the lack of knowledge of this circumstance amongst rural postmenopausal subjects. To sell expertise and higher fitness searching for conduct amongst postmenopausal girls, it’s far important to evaluate their present day country of recognition and paintings in the direction of decreasing the diagnosed gaps in expertise. The effects of this look at are applicable for own circle of relatives and number one care physicians in addition to for coverage makers to behaviour applications periodically to initiate the notice amongst postmenopausal girls concerning osteoporosis. Hence, this look at became achieved to evaluate the notice of osteoporosis amongst postmenopausal girls, attending a coaching sanatorium in southern India. The look at achieved the use of a formerly confirmed questionnaire- primarily based totally tool (Figure 7) Osteoporosis knowledge assessment tool (OKAT).
The reason for the study was to evaluate the extent of awareness of osteoporosis amongst postmenopausal women attending a coaching health center in southern India, specifically in regards to danger elements, remedy options, and results. The reason for choosing postmenopausal women as observe individuals changed into that they’re at the best danger for osteoporosis and fragility fractures, and this warrants early and pre-emptive screening on this group. In this observation, the implied age of attainment of menopause changed into forty-six years. This is regular with the observations carried out with the aid of using Ahuja, et al. [24] wherein the common age of menopause of an Indian girl changed into forty six.2 years [25]. The median age at menopause amongst white ladies from industrialized international locations stages among 50 and 52 years [26, 27, 28, 29]. Earlier menopause is related to an accelerated danger of osteoporosis and fragility fractures. This underscores the want for the well-timed screening of postmenopausal ladies and early initiation of remedy to save you the prevalence of fractures.
To the quality of our understanding, that is the primary observation from south India to evaluate recognition concerning osteoporosis, amongst a cohort of postmenopausal ladies referred for DXA scan. Overall, it changed into discovered that the knowledge approximately osteoporosis, its danger elements, and remedy changed into bad on this cohort. In a comparable observe achieved in one hundred postmenopausal ladies, there has been an amazing deficit in understanding concerning osteoporosis and its prevention [29, 30, 31, 32, 33].
The grossly insufficient country of recognition in regards to osteoporosis mandates that remedial measures be followed to bridge this hole in understanding [33, 34, 35]. The individuals of our observation had a bad understanding approximately the danger elements and the results of osteoporosis and simplest 13% have been conscious that powerful remedies for osteoporosis existed in India.
This unluckily displays the large lacunae in the knowledge of the disabling results of osteoporosis, its danger elements, and remedy. On evaluating the overall performance of individuals stratified in step wFith their academic status, no large distinction changed into determined among illiterate/ number one stage knowledgeable and the relaxation of the individuals in regards to osteoporosis recognition [36, 37, 38, 39, 40]. A small survey carried out in western India has proven media to be the maximum not unusual place supply of facts on osteoporosis and simplest 1 / 4 of the topics recognized medical doctors as a supply of facts. This well-known shows the truth that with the contemporary gadget of schooling, the burden of significance given to osteoporosis and its results might be suboptimal.
This requires the initiation of tutorial ventures as a way to decorate recognition approximately osteoporosis and its remedy. Family physicians who offer number one care to the aged have to talk approximately osteoporosis in the course of health facility visits for control of continual illnesses consisting of diabetes or hypertension.
Conducting osteoporosis recognition applications in faculties and faculties will help in enhancing their understanding on this regard [41]. Utilizing mass media consisting of print, broadcast, and virtual media to enhance recognition will assist in achieving out to a majority of the overall public. Individuals susceptible to osteoporotic fractures that attend hospitals for different illnesses maybe supplied with facts leaflets approximately osteoporosis and fall prevention. Primary care physicians need to prioritize on designing suitable fitness schooling techniques for people at accelerated danger of osteoporosis primarily based totally on their stage of literacy.
Osteoporosis recognition applications at the mass media in nearby languages could attain a massive share of people.
Management of Postmenopausal Osteoporosis
Lifestyle Modifications
A. Dietary calcium: Calcium enables preserving the strength and shape of bones. Calcium is available in the maximum of the dairy products. The recommended day by day allowance of calcium is 1000-1500 mg. Much Indian research has proven that our nutritional calcium consumption is properly beneath the advocated amount. In a cross-sectional look from South India, 74.5% of the postmenopausal girls have been ingesting much less than the advocated day by day allowance of calcium.
B. Physical activity: Reduced physical activity is a major risk factor for the development of osteoporosis and fractures. Moderately increased physical activity, which is done regularly for long-term periods, helps in improving the mechanical competence of the skeletal system considerably. C. Fall prevention: Elderly people are more prone to fall because of poor eye sight, loss of coordination, and development of neuropathy. They should be aware of the fall preventive measures such as, using hand rails for going up and down the steps, avoid walking in slippery surfaces and using a walking stick if needed. D. Calcium and cholecalciferol: Calcium and Vitamin D supplements are considered a first-line treatment in osteoporosis. Various calcium preparations are available in our country. Calcium carbonate needs acid for its absorption. In patients who are taking drugs which reduce gastric acid secretion, it is advised to give calcium citrate maleate. Vitamin D supplementation in the form of cholecalciferol is considered one of the early treatments in osteoporosis (Table 3). Vitamin D deficiency is prevalent in 70% of the general population in our country [8, 42]. Cholecalciferol 60,000 U once in every 1–2 months is recommended in all postmenopausal women with or without osteoporosis. Active Vitamin D (calcitriol) is not indicated in the usual management of osteoporosis unless patients have renal dysfunction. The table below is a collection of Indian foods that have rich calcium content (Table 4).
| S.No | Dietary Product | Serving | Calcium(Mg) |
|---|---|---|---|
| 1 | (Buffalo) Milk, Curd | 250ml | 520 |
| 2 | Milk, Curd(Cow) | 250ml | 300 |
| 3 | Milk, Curd(Low Fat) | 250ml | 300 |
| 4 | Khoa | 100gms | 600 |
| 5 | Paneer | 100gms | 320 |
| 6 | Cheese Slice | 20gms | 160 |
| 7 | Ragi | 100gms | 360 |
| 8 | Horse Gram Whole | 100gms | 270 |
| 9 | Soyabean | 100gms | 240 |
| 10 | Moth Bean/Bengal Gram | 100gms | 200 |
| 11 | Rajma | 100gms | 260 |
| 12 | Red/Green/Black Gram (Whole) | 100gms | 100 |
| 13 | Chickpea/Kabuli Chana | 100gms | 120 |
| 14 | Drum Stick Leaves/Parsly | 100gms | 300 |
| 15 | Radish Leaves/Methi Leaves | 100gms | 270 |
Table 3: Indian Foods with Calcium (Ca) Rich Content.
| Ca In Mg | |
|---|---|
| Adult Women | 600 |
| Pregnant women | 1200 |
| Women during Lactation | 1200 |
| Postmenopausal | 800 |
Table 4: Recommended Dietary Allowance of Ca (Calcium).
Pharmacotherapy
Drugs used for the treatment of osteoporosis are widely divided into antiresorptive and anabolic agents.
Antiresorptive Agents
The classification of anti-osteoporotic drugs is shown in Figure 8.
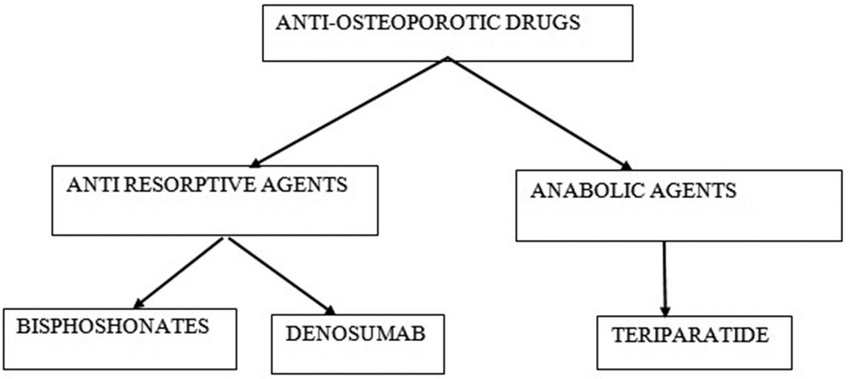
Bisphosphonates
Bisphosphonates are the class of drugs that have been used in the treatment of osteoporosis in a lot of cases.
Various bisphosphonates are listed below: 1. Zoledronic acid 4 mg intravenous (IV) once a year.
2. Alendronate 70 mg weekly.
3. Ibandronate 150 mg monthly
4. Risedronate 35 mg weekly.
In a study by Sooragonda, et al. from South India, it was found that yearly administration of zoledronic acid for 2 years showed significant improvement in BMD at lumbar spine and preserved BMD at the neck of femur. They are antiresorptive agents i.e. they target osteoclast-mediated bone resorption processes. This medication slows the breakdown and removal of bone. They have shown effective results in increasing bone mineral density (BMD) in the lumbar spine and hip bone. BPs is available as oral as well as intravenous dosage forms. The oral BPs may cause some minor gastrointestinal irritation, which can be reduced by adhering to dosing instructions. Apart from these, there are some infrequent adverse effects such as mild hypocalcaemia and muscle pain and also very rare but serious effects, such as atypical fractures and osteonecrosis of the jaw. These effects may be observed if BP treatment prolongs for more than 5 years, hence BP therapy adherence is still one of the key challenges in osteoporosis treatment, and some papers have indicated that vertebral fractures could be increased in patients who do not obey their medications properly [43].
Inadequate adherence to dose administration guidelines and early termination of medicaments has a detrimental effect on bone resorption and replacement process. Most used BPs is alendronate, risedronate, zoledronic acid, and ibandronate. But ibandronate has limitations to its use; it is not recommended in case of non-vertebral risks or risk of hip fractures.
| First line medications | Effect on vertebral fracture risk | Effect on non-vertebral fracture risk | ||
|---|---|---|---|---|
| Osteoporosis | Established osteoporosis* | Osteoporosis | Established osteoporosis* | |
| Alendronate | + | + | NA | +(including hip) |
| Risedronate | + | + | NA | +(including hip) |
| Zoledronate | + | + | + | + |
| Ibandronate | NA | + | NA | +^ |
Table 5: Efficacy of Anti-fracture first line bisphosphonates for PMO, when administered with vitamin D and calcium supplements.
Effective care of patients at elevated fracture risks includes appropriate examination and a well-planned and developed treatment procedure, keeping in compliance with the dosing protocols.
Data suggest that osteoporosis patients with successful long term compliance with treatment experience notably lower chances of fracture. Persistent care also correlates to improved BMD and improved bone resorption and replacement marker suppression. While bisphosphonates are the most effective anti-resorptive agents currently approved, they have Unique dosing problems that can have contradictory effects on long term persistence (Table 5). The difficulty of certain dosing requirements; the potential for adverse effects, particularly when the instructed doses are not followed; and very low absorption rates all lead to poor results, even under ideal conditions. The expansion of the dosage period from a once per day to a once in a week regimen is associated with comparable effectiveness, can potentially increase the protection of the gastrointestinal tract, and also associates with a major upgradation in therapy persistence.
Contraindications for Bisphosphonates
- Chronic kidney disease (estimated glomerular filtration rate).
- Suppressed bone turnover beta cross-Laps (CTX) Severe allergic reaction to previous bisphosphonate therapy.
Side Effects of Bisphosphonates
- Gastrointestinal toxicity, related to oral bisphosphonates.
- Acute-phase reaction – Fever, chills, and body pain, related to IV bisphosphonate.
- Atrial fibrillation.
- Electrolyte imbalance – Hypocalcaemia, hypomagnesaemia, hypokalemia, and hypophosphatemia.
- Related to long-term therapy -
- Excessive suppression of bone remodelling leading to increased bone fragility
- Atypical fractures – Low-energy subtrochanteric femoral fractures. These are often preceded by prodromal thigh pain
- Osteonecrosis of the jaw. Some examples are-
- Risedronate (Actonel)
- Alendronate (Fosamax)
- Ibandronate (Boniva)
- Zoledronic Acid (Reclast)
Denosumab
Denosumab is another potent antiresorptive agent which acts by inhibiting RANK ligand, thus preventing proliferation and maturation of pro-osteoclasts. It is given as subcutaneous injections once in every 6 months. This drug can be used even in patients with chronic kidney disease Stage 3 or above. It is a monoclonal antibody for osteoporosis, recently approved in India. It is given as subcutaneous injections, 60mg, once in every 6 months. It increases the cortical and cancellous bone strength, and also increases BMD, more effectively than bisphosphonates. It has good patient compliance and also is cost effective. This medication is recommended in cases of high risks of osteoporotic fractures. This drug can be prescribed even in cases of chronic renal disorders as it is finely tolerated in patients with creatinine clearance <30 ml/min [8]. The outcomes of this therapy can rebound after 6 months if the dose is not taken on time, and so any interruption or delay or termination in treatment is not recommended, especially without a subsequent antiresorptive. Thus, considering the rebound activity and to prevent it, the Swiss association guidelines have made the subsequent administration of alendronate or zoledronic acid for 2 years compulsory, initiating it 6 months from the last administration of denosumab.
ADE-Skin rash or eczema, hypocalcaemia, and over suppression of bone turnover are some of the side effects of denosumab therapy.
Example
Prolia: Contrasted and week after week organization of alendronate (Fosamax), denosumab essentially
Expands bone mineral thickness in postmenopausal patients with low bone mass. Three among post-menopausal women who had taken alendronate for at least half year, those changed to denosumab altogether expanded bone mineral thickness at one year versus the individuals who kept accepting alendronate. But, the principle motivation behind why Prolia is being dodged on the market grounds is, that it costs $1,980, i.e. 145878.58 in rupees, for one year of treatment, in addition to doctor’s or medical staff’s expenses for organization, in order to observe calcium, phosphorus, (Figure 9) and magnesium levels. All this factors makes Prolia more costly than oral or intravenous bisphosphonates.
Selective Oestrogen Receptor Modulators (SERMs)
Although the Hormone Replacement Therapy (HRT) did provide protection and relief to women dealing with postmenopausal osteoporosis, but along with that, it also brought some undesirable complications in the form of breast and endometrium cancer. Hence, the need for such a treatment that avoids these undesirable effects on other organs resulted in the development of Selective Estrogen Receptor Modulators (SERMs). SERMs are a class of drugs that inhibit bone resorption without any side effects on the endometrium and breast.
They are non- steroidal, chemically synthetic in nature. SERMs wield an anti-estrogen effect in the breast and endometrium of the uterus, whereas in the bone, they exert an estrogen agonist effect. SERMs (eg. Raloxifene) processes small surge in the BMD in comparison to other treatments but, lessens the chance of vertebral fractures by 36%. However, there is insufficient evidence for its effect on hip and no vertebral fractures, and its efficacy is lower than that of other antiresorptives. This treatment is preferably given to patients who have low risk of deep vein thrombosis; otherwise a condition of venous thromboembolic can persist. Also the ones who are at a high risk of breast cancer are prescribed SERMs (Table 6). The most frequently used drugs for SERMs, at present, are bazedoxifene and raloxifene. SERMs has proved to be a great help in lowering new vertebral fracture risk by 69% in postmenopausal women with osteoporosis over 3 years, which parallel has shown decrement by 76% in the risk of invasive breast cancer [8].
| Drug | Endometrium | Breast | Bone | Lipids |
|---|---|---|---|---|
| Toremifene | + | - | + | + |
| Tamoxifen | + | - | + | + |
| Raloxifene | - | - | + | + |
| Estradiol | + | + | + | + |
Table 6: Effects Of FDA approved SERMs on specific tissues
Calcitonin
Calcitonin acts by inhibiting bone resorption by increasing osteoblast activity. To date, data on the effect of calcitonin on BMD of other skeletal sites are conflicting, as shown in recent studies. Hence, it is not recommended for the treatment of osteoporosis.
Anabolic Agent
• Teriparatide: Teriparatide is a recombinant human PTH (1–34) which is administered as subcutaneous injections daily (20 µg/day). The total duration of treatment ranges from 18 to 24 months. Cost is a major concern in PTH therapy. As teriparatide increases both bone formation and resorption, it is advised to give bisphosphonates after completing the course of PTH therapy.
Indications for teriparatide
- Multiple vertebral fractures (clinical or radiographic)
- Very low BMD (T-score <-3)
- Suboptimal response to antiresorptive therapy (incident fractures or active bone loss during therapy Newer drugs in anti-osteoporotic therapy
- Abaloparatide
- Romosozumab.
Using anabolic and antiresorptive agents in combination or in succession improve bone density and bone strength more than either agent alone due to their synergistic action. (Table 7) this is called combination/sequential therapy and is useful in selected cases.
| Drug | Dosa Ge | Route | Position In Therapy | Vertebral* | Hip* | Non- Vertebral* | Precautions | Advantages | Disadvantag Es | Contra- Indications | Adverse Effects |
|---|---|---|---|---|---|---|---|---|---|---|---|
| CALCITONIN | 200 IU daily | Nasal Therapy | line 2nd | Yes, 21 % | No | No | Serious hypersensit ivity reactions, including fatal anaphylaxis | Ease of administrat ion | Circulating antibodies to calcitonin- salmon may develop, and may cause loss of response to treatment | Hypersensitiv ity to calcitonin- salmon | Rhinitis, Epistaxis, and Allergic reactions, |
| TIBOLONE | 2.5 mg daily | Oral | 1st line | Yes, 50 % | Yes, 26 % | Yes, 26 % | drug interaction with Warfarin | Increases BMD, decreases cholesterol and triglyceride s | Reduction of HDL levels and its high cost | Pregnancy and lactation, Breast cancer, Oestrogen dependent malignant tumours, Hypersensitiv ity to the active substances, Porphyri | Vaginal discharge, Endometrial wall thickening, Postmenopausal haemorrhage, Breast tenderness, Genital pruritus, Vaginal candidiasis, Vaginal haemorrhage, Abnormal hair growth, Lower abdominal pain |
| RALOXIFENE | 60 mg every daily | Oral | At risk of breast cancer, < 10 yrs menopause | Yes, 40 % | No | No | With a low risk of deep vein thrombosis , in case bisphospho nates or denosumab are not appropriat e, or with a high risk of breast cancer. | reduced incidence of invasive estrogen receptor positive breast cancer | Daily oral administration | Pregnancy, lactation, Active history of thromboemb olic disorders | Venous thromboembolism, Stroke, Myocardial infarction, Cancer (breast, endometrial, ovary), Dementia, Gallbladderdisease, and Urinary incontinence |
| DENOSUMAB | 60 mg every 6 month s | SC | 1st line | Yes, 68 % | Yes, 40 % | Yes, 20 % | Hypocalce mia, Vit D status, , Pregnancy, Lactation, Pediatric | 1st line drug, can be used in patients in eGFR 15-30 ml/min | Loss of effect after discontinuati on | Hypocalcemi a, Hypersensitiv ity | Dermatitis, Rash, Mild bone/Muscle pain, UTIs |
| TERIPARATIDE | 20 mcg daily SC | SC | For severe osteoporosis | Yes, 65 % | Insufficient data | Yes, 53 % | Hypocalcae mia, Vit D status, Hypersensit ivity, Local tissue damage, Pregnancy, Lactation, Pediatric | Potent bone forming activity, Large increase in spine BMD over 2 years | Reserved line drug, 2 years usage, daily injections required | Hypocalcemi a, Hypersensitiv ity | Headache, Hypercalcemia, Hypercalciuria, Renal adverse effects, Nausea, Rhinitis, Arthralgia |
| RISEDRONATE | 5 mg daily; 35 mg weekl y; 150 mg month ly | Oral | 1st line | Yes, 41-49 % | Yes, 30 % | Yes, 36 % | should not be used in patients with eGFR below 30 ml/min, Pregnancy, Lactation, Paediatric | Inconvenient administratio n- stay uptight for 30 mins on intake, no food before drug consumption, drug holiday may be needed 3-5 years | Hypocalcaem ia, Hypersensitiv ity, Compromise d renal function, Upper GI disease, patients at increased risk of aspiration | Rash, Abdominal pain, Dyspepsia, Diarrhoea, Arthralgia | |
| ALENDRONATE | 5/10mg daily; 35/70mg weekl y; 150mg month ly | Oral | 1st line | Yes, 50 % | Yes, 51-56 % | Yes, 49% | should not be used in patients with eGFR below 30 ml/min, Pregnancy, Lactation, Paediatric | Most commonly used drug | Inconvenient administratio n-stay uptight for 30 mins on intake, no food before drug consumption, drug holiday may be needed 3-5 years | Hypocalcaem ia, Hypersensitiv ity, Compromise d renal function, Upper GI disease, patients at increased risk of aspiration | Dyspepsia, Esophagitis abdominal pain, Musculoskeletal |
Table 7: Common medications used in Osteoporosis Therapy.
Monitoring and Follow-up
Those who are on anti-osteoporotic treatment should be monitored for side effects of the drugs. It is very important to decide the frequency and duration of the treatment for each patient according to their response to therapy. BTMs (if available) can be monitored once in every 3–6 months, BMD by DXA once in every 1–2 years, and X-ray spine and hip – if clinically indicated. It is important to screen for atypical femur fracture in any patient on bisphosphonate therapy who presents with thigh pain. Drug holiday – in patients who are on antiresorptive therapy, it is advisable to withhold treatment if the bone turnover is suppressed.
Conclusion
As per the various studies conducted over the last few years it’s now clear that there is a gradual increase of postmenopausal osteoporosis in women all across the globe especially India. Hormone Replacement Therapy (HRT) cannot be taken as a permanent or definitive solution to this crippling disease due to higher risk/benefit ratio making it unfavourable. A lot of patients with even fragility fractures aren’t tested properly these days leading to disability or even death. Therefore it’s highly important that with the help of global organizations and country based ones multipronged approach involving education intervention, lifestyle modification, fall prevention, appropriate pharmacotherapy for the patients, campaigns and awareness be spread regarding the prevention and treatment of PMO among people especially women. If this issue is addressed soon it can help avoid the threat imposed on the quality of life of a women suffering from postmenopausal osteoporosis and also remove a major burden on the economy.
References
-
Cooper C, Campion G, Melton LJ (1992) Hip fractures in the elderly: A world-wide projection. Osteoporos Int 2(6): 285-289.
-
Kadam N, Chiplonkar S, Khadilkar A, Divate U, Khadilkar V (2010) Low bone mass in urban Indian women above 40 years of age: Prevalence and risk factors. Gynecol Endocrinol 26(12): 909-917.
-
Silverman BK (1979) NIH consensus development conferences. Clin Pediatr (Phila) 18: 454-462.
-
Malhotra N, Mithal A (2015) Osteoporosis in Indians. Indian J Med Res 127(3): 263-268.
-
Babu AS, Ikbal FM, Noone MS, Joseph AN, Samuel P (2009) Letters To Editor Osteoporosis And Osteopenia In India : A Few More Observatons 63(2): 76-78.
-
Paul TV, Thomas N, Seshadri MS, Oommen R, Jose A, et al. (2008) Prevalence of Osteoporosis in Ambulatory Postmenopausal Women from a semiurban Region In Southern India : relationship to calcium nutrition and vitamin D Status. Endocr Pract 14(6): 665-671.
-
Tandon V, Sharma S, Mahajan S, Raina K, Mahajan A, et al. (2014) Prevalence of vitamin d deficiency among Indian menopausal women and its correlation with diabetes: A first Indian cross sectional data. J Midlife Health 5(3): 121-125.
-
Meeta, Harinarayan CV, Marwah R, Sahay R, Kalra S, et al. (2013) Clinical practice guidelines on postmenopausal osteoporosis: An executive summary and recommendations. J Midlife Health 4(2): 107-126.
-
Marwaha RK, Tandon N, Gupta Y, Bhadra K, Narang A, et al. (2012) The prevalence of and risk factors for radiographic vertebral fractures in older Indian women and men: Delhi Vertebral Osteoporosis Study (DeVOS ). Arch Osteoporos 7: 201-207.
-
Dhanwal DK, Siwach R, Dixit V, Mithal A, Jameson K, et al. (2013) Incidence of hip fracture in Rohtak district, North India. Arch Osteoporos 8(0): 135.
-
Kanis JA, Johnell O, De Laet C, Johansson H, Oden A, et al. (2004) A meta-analysis of previous fracture and subsequent fracture risk. Bone 35(2): 375-382.
-
Cuddihy M, Gabriel SE, Crowson CS, Fallon WMO, Melton LJ (1999) International Original Article Forearm Fractures as Predictors of Subsequent Osteoporotic Fractures 9(6): 469-475.
-
Feng X, Mc donald JM (2011) Disorders of Bone Remodeling. Annu Rev Pathol 6: 121-145.
-
Parker SE (2014) the Incidence of Osteoporosis : The Influence of Prenatal Exposure to Diethylstilbestrol. 99: 594-601.
-
Palacios S, Henderson VW, Siseles N, Tan D, Villaseca P (2010) Age of menopause and impact of climacteric symptoms by geographical region. Climacteric 13(5): 419-428.
-
Keramat A, Patwardhan B, Larijani B, Chopra A, Mithal A, et al. (2008) The assessment of osteoporosis risk factors in Iranian women compared with Indian women. BMC Musculoskelet Disord 9: 28.
-
Pothiwala P, Evans EM, Chapman-Novakofski KM (2006) Ethnic variation in risk for osteoporosis among women: A review of biological and behavioral factors. J Women’s Heal 15(6): 709-719.
-
Shetty S, Kapoor N, Bondu J, Thomas N, Paul T (2016) Bone turnover markers: Emerging tool in the management of osteoporosis. Indian J Endocrinol Metab 20(6): 846-852.
-
Siris ES, Chen YT, Abbott TA, Barrett-Connor E, Miller PD, et al. (2004) Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch Intern Med 164(10): 1108-1112.
-
Watts NB, Cooper C, Lindsay R, Eastell R, Manhart MD, et al. (2004) Relationship between Changes in Bone Mineral Density and Vertebral Fracture Risk Associated with risedronate: greater increases in bone mineral density do not relate to greater decreases in fracture risk J Clin Densitom 7(3): 255-261.
-
Kanis JA, Johansson H, Harvey NC, McCloskey EV (2018) A brief history of FRAX. Arch Osteoporos 13(1): 118.
-
Faizi N, Kazmi S (2017) Universal health coverage ‑ There is more to it than meets the eye. J Fam Med Prim Care 6(1): 169-170.
-
Cherian KE, Kapoor N, Asha HS, Thomas N, Paul TV (2018) Influence of Different Reference Databases on Categorization of Bone Mineral Density : A Study on Rural Postmenopausal Women from Southern India. Indian J Endocrinol Metab 22(5): 579-583.
-
Ahuja M (2016) Age of menopause and determinants of menopause age : A PAN India survey by IMS. J Midlife Health 7(3): 126-131.
-
Luoto R, Kaprio J, Uutela A (1994) Age at Natural Menopause and sociodemographic Status in Finland. 139(1): 64-76.
-
Seth A, Marwaha RK, Singla B, Aneja S, Mehrotra P, et al. (2009) Vitamin D nutritional status of exclusively breast fed infants and their mothers. J Pediatr Endocrinol Metab 22(3): 241-246.
-
Kemenkes RI (2011) Dietary Guidelines for Indians. Acta Univ Agric Silvic Mendelianae Brun 16: 39-55.
-
Ritu, G Gupta A (2014) Vitamin D deficiency in India: prevalence, causalities and interventions. Nutrients 6(2): 729-775.
-
Subramaniam R (1996) Gender-bias in India: The importance of household fixed-effects. Oxf Econ Pap 48(2): 280-299.
-
Sanwalka NJ, Khadilkar AV, Mughal MZ, Sayyad MG, Khadilkar VV, et al. (2010) A study of calcium intake and sources of calcium in adolescent boys and girls from two socioeconomic strata, in Pune, India. Asia Pac J Clin Nutr 19(3): 24-329.
-
Shetty S, Kapoor N, Dukhabandhu N, Asha HS, Thomas N, et al. (2014) The impact of the Hologic vs the ICMR database in diagnosis of osteoporosis among south Indian subjects. Clin Endocrinol (Oxf) 81(4): 519-522.
-
Sharma R, Sandhu JK, Sharda P, Sharma R, Kaur K (2018) Screening for bone mineral density using distal radius ultrasound (quantitative ultrasound scan) Physiotherapy 12(1): 16-21.
-
Hiremath MRN, LtCol Yadav AK, Ghodke MS, Yadavd J, Lat MS, et al. (2016) Osteoporosis among household women : A growing but neglected phenomenon. Med J Armed Forces India 74(1): 5-10.
-
Marwaha RK, Tandon N, Garg MK, Kanwar R, Narang A, et al. (2011) Bone health in healthy Indian population aged 50 years and above. Osteoporos Int 22(11): 2829- 2836.
-
Unni J, Garg R, Pawar R (2020) Bone mineral density in women above 40 years. J Midlife Health 1(1): 19-22.
-
Chhibber G, Roy R, Eunice M, Srivastava M Ammini AC (2007) Prevalence of osteoporosis among elderly women living in Delhi and rural Haryana. International journal of Endocrinology and metabolism 11(1): 11-14.
-
Gupta R, Mahajan S, Dewan D, Gupta R (2017) Screening of osteoporosis using calcaneal quantitative ultrasound in a rural population of Jammu , Jammu and Kashmir, India. IJCMPH 4(4): 940-943.
-
Gallagher JC, Harsha ST (2014) Prevention and treatment of postmenopausal osteoporosis. J Steroid Biochem Mol Biol 142: 155-170.
-
Patel S (2015) Osteoporosis : From concepts to T scores and now absolute fracture risk. Indian J Rheumatol 10(4): 216-220.
-
Younger DS (2016) D S Health Care in India. Neurol Clin NA 34(4): 1103-1114.
-
Ved RR, Gupta G, Singh S (2019) India’s health and wellness centres : realizing universal health coverage through comprehensive primary health care. WHO South East Asia J Public Health 8(1): 18-20.
-
Raina SK (2019) Letter to Editor Need for a novel health care delivery model focusing on primary care 2019- 2020.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era