Evaluation of Sperm Selection Technique Using Hyaluronic Acid Binding During ICSI; A Randomized Controlled Trial
Objective: To compare between Hyaluronan binding system for sperm selection for ICSI procedures (PICSI) and conventional morphology sperm selection. In vitro sperm selection for ICSI is important as it has a direct influence on the paternal contribution of preimplantation embryogenesis. Various laboratory tests were developed to assess the functions of the spermatozoa. Among them, only the tests for sperm DNA fragmentation, hyperactivation of the spermatozoa and the hyaluronan-binding ability are simple and fast. Study Design: A randomized controlled trial where three-hundred cases with male infertility were divided into 3 equal groups according to semen abnormality (oligo, astheno and teratozoospermia) then each group was randomly divided into 2 equal subgroups one underwent PICSI and the other underwent conventional ICSI. The outcomes were fertilization,high quality embryos and clinical pregnancy rate. Results: A significant difference was found in favor of PICSI as regards both high-quality embryos and clinical pregnancy rate in all 3 groups. A significant difference was also found in fertilization rate in favor of PICSI group in both oligozoospermia and teratozoospermia groups but not in asthenozoospermia group. Conclusion: PICSI technique provides better high-quality embryos, fertilization, and clinical pregnancy rates in cases with male factor infertility; however, further studies are needed to define specific criteria for performing PICSI taking into consideration both the expenses and time of the technique.
Introduction
In-vitro sperm selection for intracytoplasmic sperm injection (Physiological ICSI or PICSI) is crucial as it has a direct influence on the paternal contribution of preimplantation embryogenesis. Men with oligozoospermia who require ICSI often demonstrate compromised DNA integrity and increased chromosomal aberrations of the sperms in their semen. Studies have shown that embryos resulting from ICSI in those men have higher risk of sex chromosome disomies, chromosomal aneuploidies, de novo numerical chromosomal aberrations and cytogenetically detectable structural chromosomal aberrations. Although the primary candidates for ICSI are oligozoospermic men, there is an increase in the use of ICSI; therefore, more couples are potentially exposed to those potential risks [1, 2, 3, 4].
Various laboratory tests were developed to assess the functions of the spermatozoa. Among them, only the tests for sperm DNA fragmentation (Halosperm), hyperactivation of the spermatozoa, and the hyaluronan-binding ability are fast and straightforward enough to allow the semen sample to be used for oocytes’ insemination. Spermatozoa that fail to bind to hyaluronan have many aspects of immaturity. They retain histones in the sperm nucleus, cytoplasm on the sperm neck, and have higher aberrant sperm head morphology, in addition to lower genomic integrity [5, 6]. It has also been shown that sperm DNA fragmentation is associated with male factor of infertility, correlating with the morphology and motility of spermatozoa [7, 8, 9, 10].
In the systematic review and meta-analysis by Beck- Fruchter R, et al. [11], the authors addressed the clinical benefit from using the hyaluronic acid binding system in ICSI. They included only seven studies with 1437 ICSI cycles. They conclude that the usage of hyaluronic acid binding system led to no improvement in both fertilization rate and pregnancy rate. However, they found an improvement in the embryo quality. The techniques for hyaluronic acid binding were not identical and semen quality was not detailed in all studies [11, 12]. Therefore, the evidence for the use of hyaluronic acid binding in (ICSI) cycles to improve the clinical outcomes is not conclusive as none of studies addressed the issue had sufficient statistical power. Also, the results of these studies are contradictory. Thus, the present study aimed to carry out a comparative analysis of the ICSI- ET outcomes between two groups: The hyaluronan binding system for sperm selection for ICSI procedures [Hyaluronic acid (HA) group] and another group of conventional morphology sperm selection [polyvinyl pyrolidone (PVP) group], both in cycles with only male factor infertility.
Methods
This prospective randomized controlled parallel double- blinded study was conducted at the International Islamic Institute for Population Studies and Research, assisted reproductive unit, Al-Azhar University, Cairo, Egypt, during the period from January 2019 to August 2020. This study conformed to the Medical Research Involving Human Subjects Act and the principles of the declaration of Helsinki. In addition, the local ethical committee approved it under the registration number (His_12Med.Research_0000012). The purpose of this study was explained to all participants before their enrollment to the study, and an informed consent form was signed by all participants.
We recruited all couples with male factor infertility that met the inclusion and exclusion criteria and were eligible for participation in this study. For inclusion in the study, all the following criteria were to be fulfilled: couples who were willing to do ICSE-ET, male age 18-55 years able to produce freshly ejaculated sperm for the treatment cycle. Female age 18-43 years, body mass index (BMI) 19.0- 35.0 kg/m2, with regular menstrual cycle, normal hormonal profile (FSH, LH, PRL), normal ovarian ultrasound and normal pelvic ultrasound. Exclusion criteria included: women with known medical disease (e.g., sever hypertension or hepatic disease), history of altered karyotype in one or both partners, history of chronic, autoimmune, or metabolic diseases, and presence of endocrinopathies. Women were subjected to full history taking, general examination and pelvic examination. Full Investigations were made for them: AMH, LH, FSH, E2, prolactin, and TSH using ELFA technique (Enzyme linked Fluorescent Assay, Vidas Biomerieux). Routine preoperative investigations (HB%, fasting blood sugar, 2 hours postprandial blood sugar, liver, and kidney function tests, HBS Ag, HCV Ab). Premedication US were made to evaluate the ovaries & endometrium. E2 levels monitoring to ensure pituitary down-regulation and for follow-up during folliculometry using ELFA technique.
Randomization and Blinding
For allocation of the participants, stratification of couples according to semen analysis into three groups (oligozoospermia, asthenozoospermia & teratozoospermia) according to the World Health Organization (WHO) criteria, 2010. Each stratum included 100 males. Oligozoospermia defined as sperm concentration: 5-10 million/ml. Asthenozoospermia defined as progressive motility (PR) < 32%. Teratozoospermia defined as normal sperm morphology < 4% [13]. Then, randomization was made within each stratum using a computer-generated list of random numbers. Block randomization with a block size of four was used with a 1:1 ratio of the HA group and the PVP group. The study was a double-blinded study, as the couples did not know which groups they are assigned for, and the assessor was blinded.
Technical Approach
Before randomization, for all men enrolled to the study, semen analysis and sperm preparation were made. Semen samples were collected by masturbation after a 3to7 days period of sexual abstinence. Physical examination including volume, color, odor, and liquefaction were done. Microscopic examination (Olympus, C 21, Japan) was done to evaluate sperm concentration, motility, morphology, and the presence of another cellular element. Sperms were classified into progressive motile, non-progressive and Immotile. After randomization, sperm samples for ICSI were processed after microscopic examination, 1 ml of sperm gradient medium (Pure sperm, Nidacon, Sweden ) were added on fresh sample and centrifuged at 1800 rpm for 10 minutes (Heraeus 300, Osterode, Germany), supernatant was removed, and then we add 2 ml of sperm washing medium (Sage, Denmark) to sperms in the resulting pellet and centrifuged at 1800 rpm for 10 minutes to reach to a number of motile and morphologically normal sperm cells needed for assisted reproduction. Posterior morphology ICSI (PICSI) was made for the HA group only.
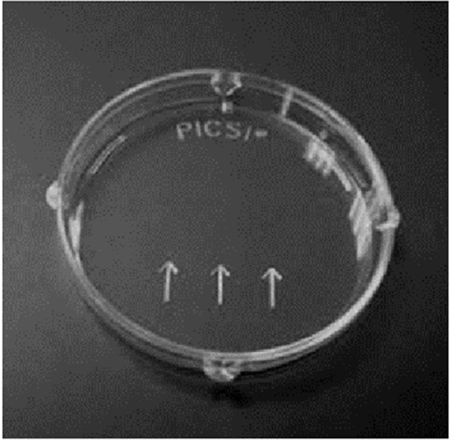
PICSI dishes (ORIGIO, Cooper Surgical Company, Denmark) are conventional plastic culture dishes pre- prepared with 3 microdots of powder. The powdered HA is re-hydrated by adding 5 μL droplets of fresh culture medium to each of the three microdots. A 2 μL droplet with suspension of treated spermatozoa is then connected with a pipette tip to these culture medium droplets. The PICSI dish is incubated under oil; within 5 minutes the bound spermatozoa are attached by their head to the surface of the HA-microdots and are spinning around their head. An ICSI injecting pipette (Vitrolife, Sweden) is used to pick the best motile HA-bound sperm up and inject them one by one into an oocyte. The ICSI injecting pipette can be previously loaded with viscous medium PVP or Sperm Slow (Irvine, USA) to facilitate sperm micromanipulation Figure 1.
Controlled Ovarian Hyperstimulation
Controlled ovarian hyper stimulation (COS) was performed using long GnRH agonist protocol. In this protocol, the patients started administration of GnRH agonist, triptorelin 0.1 mg (Decapeptyl 0.1, Ferring, Egypt) on the 21 days of the cycle IM once. After 14 days of GnRH-agonist treatment, ovarian down-regulation was confirmed by measurement of serum E2 level. If the level of E2 50 pg/mL or less, gonadotrophins was started using recombinant FSH (Gonal-F, EMD Serono Inc., USA) or urinary HMG (Merional 75, IBSA Inc., Switzerland), commonly with a starting dose of 150-225 IU injected SC daily. FSH dose was adjusted according to the ovarian response, and serial E2 and transvaginal US (SONOACE X4 –MEDISON Korea.) were performed every 2-3 days from day 6 of FSH stimulation onward. When three or more follicles had reached a size 18 mm, final oocyte maturation was induced using intramuscular injection of 10,000 IU of HCG (Choriomon, IBSA Inc., Switzerland).
For collection of human cumulus cells, oocytes were aspirated under general anesthesia using transvaginal US, approximately 34-36 hours after the HCG administration (Labotect aspiration pump, Germany). Follicles were aspirated with a negative pressure of 115-120 mm Hg using a single lumen 17-gauge oocyte pick-up needle (Reproline Medical, Germany). Follicular fluid was aspirated into sterile tubes 14 ml (Falcon, Boen Healthcare Co., China). The Oocyte –cumulus cells complexes were isolated under a dissecting microscope (Zeiss Stemi 2000-C Stereo Microscope,) and washed in Gamete Buffer media (Cook, Limerick, Ireland) then washed and placed into four dishes containing fertilization medium (Cook, Limerick, Ireland) and incubated at 37ºC in 6% CO2 for approximately 1/2 hour (C60, Labotect, Germany). For denudation, the oocyte was placed in a 100μl drop of buffered containing hyaluronidase enzyme 80 IU/ml (Life Global, Europe) 30-45 seconds, and then the oocyte was removed and placed in 100 μl drop of Gamete Buffer media, then the corona cells were removed by gentle aspiration of the oocyte in and out of a sterile drawn pipette. When denudation was completed, the oocyte was washed in Gamete Buffer (Cook, Limerick, Ireland) and was then placed in 10 μl micro drops of the fertilization medium (Cook, Limerick, Ireland) in injection dishes, covered with 3ml of sterile equilibrated mineral oil. For the oocyte grading, the oocyte was assessed quickly for maturity & quality according to grading system using an inverted microscope with Hoffman optics (Olympus 1x71, Japan), hot stage and automatic manipulators (Narishige, japan). Maturation stages were recorded as prophase I, metaphase I (MI), metaphase II (MII) and post mature. The naked oocytes were incubated in a culture medium at 37 ºC in 6% Co2 until the ICSI procedure [14].
ICSI Procedure
Following sperm preparation as described before, samples were incubated until time of injection. Each oocyte was injected with a single morphologically abnormal and immobilized in polyvinyl pyrolidone (PVP) (Irvine, USA) spermatozoon. Individual sperm subjected to ICSI was examined and evaluated. The injection procedure was carried out in a sterilized dish using holding pipette and injection needle. Intra cytoplasmic sperm injection was performed according to the protocol of Van Steirteghem [15].
Assessment of fertilization and embryo’s quality was made 17± h after microinjection. The injected oocytes were observed for any sign of damage and for the presence of pronuclei. Oocytes were named fertilized if two pronuclei (2PN) were present and the second polar body had been extruded [16]. For embryo grading and transfere, approximately 72 h after injection, the cell number and morphology of each embryo were scored according to equality of blastomeric size and proportion of nucleate fragments. Then, best day-3 embryos (Grade1) were transferred to the uterus in 30μl of Global medium (Life Global, Europe) containing 10% HSA using ET catheter (Labotect, Germany) 48–72 h after oocyte retrieval [17]. Beta hCG titter was done for the detection of pregnancy and then was confirmed by transvaginal US examination 10-15 days after.
Statistical Analysis
The primary outcome measured was clinical pregnancy, defined as the presence of at least one intrauterine fetus with heartbeat. The secondary outcomes were the number of collected total and MII oocytes; fertilization rate, number of G1 embryos and the number of embryos transferred.
Sample size was calculated setting the power at 80% and the two-sided confidence level at 95%. A minimal sample size of 45 couples in each group was needed. We considered a total sample size of 300 to allow for subgroup analysis according to semen analysis and to compensate for any dropouts.
The statistical analysis was made on the intent-to-treat (ITT) population. All statistical tests were made using a significance level of 95%. A p-value < 0.05 was considered statistically significant. SPSS software (Statistical Package for the Social Sciences, version 20.0, SSPS Inc., Chicago, IL, USA) was used. Data were presented as (mean ± SD) or median (range) for continuous variables and as frequency & percent for categorical variables. Comparisons between groups were made using Chi-square test for categorical variable and the independent t-test for the continuous variables.
Results
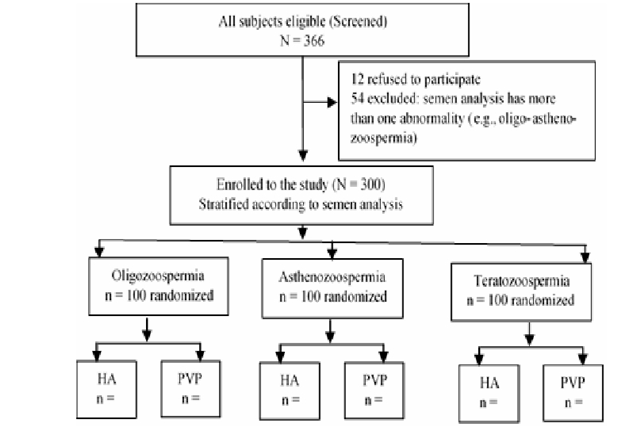
A total of 366 couples were asked to participate in the study. Twelve refused to participate, and 54 were excluded before randomization. Three hundred participants (100 with oligozoospermia, 100 with asthenozoospermia & 100 with teratozoospermia) were enrolled. Randomization was done within each semen category with 50 assigned to the HA group and 50 to the PVP group Figure 2.
Both groups were comparable with regard their baseline characteristics either overall dataset or in oligozoospermia, asthenozoospermia and teratozoospermia subsets. There was no statistically significant difference (p > 0.05) between the two groups regarding the female age, female BMI, and the duration of infertility Table 1.
| Parameter | HA group (n.=150) Mean (SD) | PVP group (n.=150) | P-Value |
|---|---|---|---|
| Mean (SD) | |||
| Female age, years | 27.02 (5.71) | 28.17 (5.5) | 0.078 |
| Female BMI, Kg/m2 | 26.86 (4.66) | 27.1 (4.51) | 0.652 |
| Duration of infertility, years | 7.32 (2.03) | 7.54 (2.05) | 0.335 |
Table 1: Basal characteristics for HA and PVP groups.
The controlled ovarian and the ICSI outcomes were comparable (p-values > 0.05) between the HA and PVP groups either in the overall dataset or in oligozoospermia, asthenozoospermia and teratozoospermia subsets, except for the number of fertilized oocytes, the cleavage rate, and the number of G1 embryos (p-values < 0.05).
Overall, the number of the collected oocytes was comparable (p-value 0.612) between the HA and PVP groups; [mean± (SD), was 6.85 (1.84) & 6.97 (2.23)] for the HA group and the PVP group, respectively. Also, overall, the number of the MII injected oocytes was comparable (p-value 0.300) between the HA and PVP groups; it was 6.29 (1.87) & 6.49 (1.44) for the HA group and the PVP group, respectively. However, overall, the number of fertilized oocytes was higher (p-value < 0.001) in the HA group 5.36 (2.08) than in the PVP group 4.63 (1.47). Also, Overall, the cleavage rate was higher (p-value < 0.001) in the HA group 755/804 (93.91%) than in the PVP group 538/694 (77.52%). Overall, G1 embryos was higher (p-value < 0.001) in the HA group with mean (SD), 3.97 (0.99) than in the PVP group 2.95 (0.83).
Moreover, in each of the oligozoospermia and teratozoospermia subsets, the number of fertilized oocytes and the fertilization rate were higher (p-values < 0.001) in the HA group than in the PVP group as shown in Table 2. However, in the asthenozoospermia subset, the number of fertilized oocytes and the fertilization rate were comparable between both groups (p-values > 0.05), Table 2.
| Parameter | HA group Mean (SD) (n.= 50) | PVP group Mean (SD) (n.= 50) | P-value | |
|---|---|---|---|---|
| Oligozoospermia (n.=100) | Female age, years | 26.36 (6.07) | 26.94 (5.29) | 0.61 |
| Oligozoospermia (n.=100) | Female BMI, Kg/m2 | 27.03 (4.42) | 28.23 (4.28) | 0.171 |
| Oligozoospermia (n.=100) | Duration of infertility, years | 7 (2.02) | 7.73 (2.13) | 0.081 |
| Asthenozoospermia (n.=100) | Female age, years | 28.22 (5.42) | 28.98 (4.94) | 0.465 |
| Asthenozoospermia (n.=100) | Female BMI, Kg/m2 | 26.71 (4.58) | 26.33 (4.23) | 0.664 |
| Asthenozoospermia (n.=100) | Duration of infertility, years | 7.57 (2.06) | 7.57 (2.07) | 0.993 |
| Teratozoospermia (n.=100) | Female age, years | 26.49 (5.55) | 28.59 (6.11) | 0.076 |
| Teratozoospermia (n.=100) | Female BMI, Kg/m2 | 26.85 (5.06) | 26.75 (4.85) | 0.92 |
| Teratozoospermia (n.=100) | Duration of infertility, years | 7.38 (2.02) | 7.33 (1.96) | 0.91 |
Table 2: Basal characteristics for the subgroups.
Moreover, in each of the oligozoospermia, asthenozoospermia and teratozoospermia subsets, the cleavage rate, and the number of G1 embryos were higher (p-values < 0.001) in the HA group than in the PVP group as shown in Table 2.
Overall, the number of transferred embryos was comparable (p-value 0.448) between the HA and PVP groups; it was 2.02 (0.56) & 2.07 (0.58) for the HA group and the PVP group, respectively. Moreover, in each of the oligozoospermia, asthenozoospermia and teratozoospermia subsets, the number of transferred embryos were comparable (p-values > 0.05) between the HA group and the PVP group as shown in Table 2.
Clinical Pregnancy
Overall, the clinical pregnancy rate, was significantly higher (p-value < 0.001) in the HA group than in the PVP group. It was 99 (66%) in the HA group and 61 (40.67%) in the PVP group, OR 2.83 (CI, 1.77-4.53), ARR 25% (14-36%) and NNT 4 (3-7).
Moreover, in each of the oligozoospermia, asthenozoospermia and teratozoospermia subsets, the clinical pregnancy rate, was significantly (p-values < 0.001) higher in the HA group than in the PVP group, as shown in Tables 3-5.
| Parameter | HA group Mean (SD) n.=150 | PVP group Mean (SD) | P- value |
|---|---|---|---|
| n.=150 | |||
| Collected oocytes mean(sd) | 6.85 (1.84) | 6.97 (2.23) | 0.612 |
| MII injected oocytes mean(sd) | 6.29 (1.87) | 6.49 (1.44) | 0.3 |
| Fertilized oocytes mean(sd) | 5.36 (2.08) | 4.63 (1.47) | < 0.001 |
| Fertilization rate, n/MII oocytes (%) | 804/943 (85.26) | 694/973 (71.33) | < 0.001 |
| Cleavage rate, n/fertilized oocytes (%) | 755/804 (93.91) | 538/694 (77.52) | < 0.001 |
| G1 embryos mean(sd) | 3.97 (0.99) | 2.95 (0.83) | < 0.001 |
| Transferred embryos mean(sd) | 2.02 (0.56) | 2.07 (0.58) | 0.448 |
Table 3: Controlled ovarian stimulation and ICSI outcomes in HA and PVP groups.
| Subgroups (n-=300) | Parameters | HA group) n.=50 | PVP group n.=50 | P-value |
|---|---|---|---|---|
| Oligoszoopermia | Collected oocyte, mean(sd) | 6.72 (1.74) | 7.08 (2.38) | 0.39 |
| MII injected oocytes, mean(sd) | 6.24 (2.15) | 6.58 (1.52) | 0.363 | |
| Fertilized oocytes, mean(sd) | 5.78 (1.69) | 5.06 (1.39) | 0.022 | |
| Fertilization rate, n/MII oocytes (%) | 289/312 (92.63%) | 253/329 (76.90) | < 0.001 | |
| Cleavage rate, n/fertilized oocytes (%) | 268/289 (92.73%) | 206/253 (81.42) | < 0.001 | |
| G1 embryos, mean(sd) | 4.88 (1.09) | 3.92 (1.03) | < 0.001 | |
| Transferred embryos, mean(sd) | 2.02 (0.58) | 2.08 (0.55) | 0.597 | |
| Asthenoszoopermia | Collected oocytes, mean(sd) | 7.02 (1.84) | 6.82 (2.26) | 0.622 |
| MII injected oocytes, mean(sd) | 6.34 (1.68) | 6.26 (1.47) | 0.801 | |
| Fertilized oocytes, mean(sd) | 4.48 (1.60) | 4.58 (1.61) | 0.756 | |
| Fertilization rate, n/MII oocytes (%) | 224/317 (70.66%) | 229/313 (73.16) | 0.486 | |
| Cleavage rate, n/fertilized oocytes (%) | 219/224 (97.77%) | 185/229 (80.79) | < 0.001 | |
| G1 embryos, mean(sd) | 4.06 (0.85) | 2.60 (0.75) | < 0.001 | |
| Transferred embryos, mean(sd) | 2.06 (0.56) | 2 (0.63) | 0.616 | |
| Teratozoospermia | Collected oocytes, mean(sd) | 6.8 (1.96) | 7 (2.09) | 0.616 |
| MII injected oocytes, mean(sd) | 6.28 (1.81) | 6.62 (1.33) | 0.279 | |
| Fertilized oocytes, mean(sd) | 5.82 (2.04) | 4.24 (1.3) | < 0.001 | |
| Fertilization rate, n/MII oocytes (%) | 291/314 (92.68%) | 212/331 (64.05) | < 0.001 | |
| Cleavage rate, n/fertilized oocytes (%) | 268/291 (92.10%) | 147/212 (69.34) | < 0.001 | |
| G1 embryos, mean(sd) | 2.96 (0.74) | 2.32 (0.53) | < 0.001 | |
| Transferred embryos, mean(sd) | 1.98 (0.54) | 2.12 (0.58) | 0.215 | |
| HA group | PVP group | p | ||
| The entire dataset | Clinical pregnancy, number (%) | 99 (66%) | 61 (40.67%) | < 0.001 |
| OR, estimate (95% CI) | 2.83 (1.77-4.53) | |||
| ARR, estimate (95% CI) | 25% (14-36%) | |||
| NNT, estimate (95% CI) | 4 (3-7) | |||
| Subgroups | ||||
| Oligozoospermia | Clinical pregnancy, number (%) | 35 (70%) | 23 (46%) | 0.011 |
| OR, estimate (95% CI) | 2.74 (1.2-6.23) | |||
| ARR, estimate (95% CI) | 24% (5-43%) | |||
| NNT, estimate (95% CI) | 4 (2-19) | |||
| Asthenozoospermia | Clinical pregnancy, number (%) | 33 (66) | 20 (40) | 0.006 |
| OR, estimate (95% CI) | 2.91 (1.29-6.57) | |||
| ARR, estimate (95% CI) | 26% (7-45%) | |||
| NNT, estimate (95% CI) | 4 (2-14) | |||
| Teratozoospermia | Clinical pregnancy, number (%) | 31 (62) | 18 (36) | 0.006 |
| OR, estimate (95% CI) | 2.9 (1.29-6.53) | |||
| ARR, estimate (95% CI) | 26% (7-45%) | |||
| NNT, estimate (95% CI) | 4 (2-14) |
Table 4: Controlled ovarian stimulation and ICSI outcomes in the subgroups.
OR: Odds Ratio; CI: Confidence Interval; ARR: Absolute Risk Reduction; NNT: Number Needed To Treat. Table 5: Clinical pregnancy among groups.
Discussion
The current randomized controlled study showed that the number of fertilized oocytes was higher in the HA group than in the PVP group. Also, G1 embryos was higher in the HA group than in the PVP group. In addition, in each of the oligozoospermia and teratozoospermia subsets, the number of fertilized oocytes and the fertilization rate were significantly higher in the HA group than in the PVP group. However, in the asthenozoospermia subset, the number of fertilized oocytes and the fertilization rate were comparable between both groups. Moreover, in each of the oligozoospermia, asthenozoospermia and teratozoospermia subsets, the cleavage rate, and the number of G1 embryos were higher in the HA group than in the PVP group.
Overall, the number of transferred embryos was comparable between the HA and PVP groups. Furthermore, in each of the oligozoospermia, asthenozoospermia and teratozoospermia subsets, the number of transferred embryos were comparable between the HA group and the PVP group.
Also generally, the clinical pregnancy rate, was significantly higher in the HA group than in the PVP group. Additionally, in each of the oligozoospermia, asthenozoospermia and teratozoospermia subsets, the clinical pregnancy rate, was significantly higher in the HA group than in the PVP group.
The current study agreed with the study done by Erberelli, et al. [18], who studied 56 cases (19 ICSI and 37 PICSI) and reached similar results. Like our study, it had the advantage of classifying the different types of abnormal semen parameters (oligo, terato and asthenozoospermia). However, our study recruited a larger number than that of [18].
In discordance with the results of the current study, the study of Erbelli, et al. [18] showed that the number of aspirated oocytes in the PICSI group was higher in comparison to the PVP group. That is because they did not follow a specific COS protocol. However, in the present study one controlled ovarian stimulation (COS) protocol was used for all participants [18].
Moreover, Erbelli, et al. [18] observed that the participants with teratozoospermia could benefit from the PICSI technique more than other factors sperm changes. However, in the current study, we observed the benefits in each type of sperm changes [18].
Seemingly, the benefits of the HA binding system showed significant encouraging results only for male factor infertility as shown in the study by Majumdar [19].
Worrilow, et al. [20], did a double-blinded randomized controlled study to test the effect of PICSI on implantation, clinical pregnancy and miscarriage rates initially recruiting 802 cases and classified the cases into two main groups according to the percent of sperm bound hyaluronan in semen (>65% or 65% and less) and found a significant decrease in miscarriage rates in cases using PICSI, while clinical pregnancy rate was not significant, the later finding is different from the results of the current study; however, a possible explanation of this difference is that the current study clearly demarcates the types of semen abnormalities [20].
Breznik, et al. [21], studied analysis of sperm DNA fragmentation, hyper activation and hyaluronan-binding ability on washed semen samples used for the insemination of oocytes in 133 cases undergoing IVF to determine the effect on both fertilization rate and embryo quality, and they had similar results to the current study in regarding both oligo and teratospermia groups [21].
In a systematic review by Georgina, et al. [22], to determine the efficacy of the physiological ICSI technique (PICSI) vs. conventional ICSI in the prognosis of couples with male factor, they concluded that there is no statistically significant difference between PICSI vs. ICSI, for any of the outcomes analyzed in this study.
When comparing PICSI vs. magnetic-activated cell sorting (MACS) for abnormal sperm DNA fragmentation ICSI cases Hasanen, et al. [23], in their clinical trial found that PICSI and MACS are efficient techniques for sperm selection in cases with abnormal sperm DNA fragmentation. However, MACS is preferred when the females are younger than 30 years, while PICSI is preferred in older females. However, enough information is still not available to prove the efficacy of the PICSI technique over ICSI in couples with male factor.
One advantage of this study is being randomized- controlled study with enough sample size. Furthermore, the current study categorizes three different types of male semen abnormalities separately. However, the study has some limitations as it did not report the miscarriage rate and the live-birth rate as the participant are still in the pregnancy phase.
Conclusion
PICSI technique provides better fertilization rate, higher quality embryos number, and better clinical pregnancy rate.in cases with male factor of infertility. Further studies are needed to define specific criteria for performing PICSI taking into consideration both the expenses and time of the technique.
Conflict of Interest
All authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Acknowledgement
Many thanks to all staff at embryology unit, Al-Azhar University for their support during finishing of this study.
References
-
Bonduelle M, Van Assche E, Joris H, Keymolen K, Devroey P, et al. (2002) Prenatal testing in ICSI pregnancies: incidence of chromosomal anomalies in 1586 karyotypes and relationto sperm parameters. Hum Reprod 17(10): 2600-2614.
-
Palermo GD, Neri QV, Hariprashad JJ, Davis OK, Veeck LL,et al. (2000) ICSI and its outcome. Semin Reprod Med 18(2): 161-169.
-
Simpson JL, Lamb DJ (2001) Genetic effects of intracytoplasmic sperm injection. Semin Reprod Med 19(3): 239-249.
-
Van Steirteghem A, Bonduelle M, Devroey P, Liebaers I (2002) Follow-up of children born after ICSI. Hum Reprod Update 8(2): 111-116.
-
Jakab A, Sakkas D, Delpiano E, Cayli S, Kovanci E, et al. (2005) Intracytoplasmic sperm injection: a novel selection method for sperm with normal frequency of chromosomal aneuploidies. Fertil Steril 84(6): 1665- 1673.
-
Huszar G, Ozkavukcu S, Jakab A, Celik Ozenci C, Sati GL, et al. (2006) Hyaluronic acid binding ability of human sperm reflects cellular maturity and fertilizing potential: selection of sperm for intracytoplasmic sperm injection. Curr Opin Obstet Gynecol 18(3): 260-267.
-
Daris B, Goropevsek A, Hojnik N, Vlaisavljevic V (2010) Sperm morphological abnormalities as indicators of DNA fragmentation and fertilization in ICSI. Arch Gynecol Obstet 281(2): 363-367.
-
Nasr Esfahani MH, Razavi S, Vahdati AA, Fathi F, Tavalaee M (2008) Evaluation of sperm selection procedure based on hyaluronic acid binding ability on ICSI outcome. J Assist Reprod Genet 25(5): 197-203.
-
Trisini AT, Singh NP, Duty SM, Hauser R (2004) Relationship between human sperm parameters and deoxyribonucleic damage assessed by the neutral comet assay. Fertil Steril 82(6): 1623-1632.
-
Velez de la Calle JF, Muller A, Walschaerts M, Clavere JL, Jimenez C, et al. (2008) Sperm deoxyribonucleic acid fragmentation as assessed by the chromatin dispersion test in assisted reproductive technology programs: results of a large prospective multicenter study. Fertil Steril 90(5): 1792-1799.
-
Beck Fruchter R, Shalev E, Weiss A (2016) Clinical benefit using sperm hyaluronic acid binding technique in ICSI cycles: a systematic review and meta-analysis. Reprod Biomed Online 32(3): 286-298.
-
Mokanszki A, Tothne EV, Bodnar B, Tandor Z, Molnar Z, et al. (2014) Is sperm hyaluronic acid binding ability predictive for clinical success of intracytoplasmic sperm injection: PICSI vs. ICSI? Syst Biol Reprod Med 60(6): 348-354.
-
World Health Organization (2010) WHO laboratory manual for the examination and processing of human semen. 5th (Edn.), Institutional Repository for information Sharing.
-
Verlhac MH, Terret ME (2016) Oocyte Maturation and Development. F1000Res 5: F1000 Faculty Rev-309.
-
Van Steirteghem A, Nagy P, Joris H, Verheyen G, Smitz J (1996) The development of intracytoplasmic sperm injection. Human Reproduction 11(Suppl 5): 59-72.
-
Baczkowski T, Kurzawa R, Głabowski W (2004) Methods of embryo scoring in in vitro fertilization. Reprod Biol 4(1): 5-22.
-
Nasiri N, Eftekhari Yazdi P (2015) An Overview of The Available Methods for Morphological Scoring of Pre- Implantation Embryos in In Vitro Fertilization. Cell J 16(4): 392-405.
-
Erberelli RF, Salgado RM, Pereira DH, Wolff P (2017) Hyaluronan-binding system for sperm selection enhances pregnancy rates in ICSI cycles associated with male factor infertility. JBRA Assist Reprod 21(1): 2-6.
-
Majumdar G, Majumdar A (2013) A prospective randomized study to evaluate the effect of hyaluronic acid sperm selection on the intracytoplasmic sperm injection outcome of patients with unexplained infertility having normal semen parameters. J Assist Reprod Genet 30(11): 1471-1475.
-
Worrilow KC, Smith S, Eid S, Witmyer J, Woodhouse D, et al. (2013) Use of hyaluronan in the selection of sperm for intracytoplasmic sperm injection (ICSI): significant improvement in clinical outcomes- Multicenter, double blinded and randomized controlled trial. Hum Reprod 28(2): 306-314.
-
Breznik BP, Kovacic B, Vlaisavljevic V (2013) Are sperm DNA fragmentation, hyperactivation, and hyaluronan- binding ability predictive for fertilization and embryo development in in vitro fertilization and intracytoplasmic sperm injection? Fertil Steril 99(5): 1233-1241.
-
Avalos Durán G, Cañedo Del Ángel AME, Rivero Murillo J, Zambrano Guerrero JE, Carballo Mondragón E, et al. (2018) The efficacy of the physiological ICSI technique (PICSI) vs. conventional ICSI in the prognosis of couples with Male Factor: A Systematic Review. JBRA Assist Reprod 22(2): 139-147.
-
Hasanen E, Elqusi K, ElTanbouly S, Hussin AE, AlKhadr H, et al. (2020) PICSI vs. MACS for abnormal sperm DNA fragmentation ICSI cases: a prospective randomized trial. J Assist Reprod Genet 37(10): 2605-2613.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era