An Unusual Complication of Gluteal Fistula after Sacrospinous Ligament Suspension: A Case Report
Background: Sacrospinous ligament suspension (SSLS), also referred to as sacrospinous ligament fixation, is a well-established transvaginal procedure performed to treat apical prolapse. Serious complications are uncommon following SSLS, and mild infectious complications, such as cystitis, are most common. In this report, we present an uncommon case of gluteal fistula as a complication of this procedure. Case: A multiparous 48-year-old with a history of vaginal hysterectomy with bilateral salpingectomy, anterior and posterior colporrhaphy, and sacrospinous ligament suspension presented one year later with multiple emergency department visits for gluteal abscesses and continuous right gluteal drainage. MRI confirmed a gluteal fistula extending from the sacrum to the right gluteal fold and right piriformis muscle, thought to be caused by retained suture. The patient subsequently underwent an exam under anesthesia in which the reproduction of the vaginal dissection performed to place the SSLS sutures and probing of the fistula failed to expose any suture. The fistula was copiously irrigated with antibiotic solution, and on a 2-week postoperative visit, the fistula was noted to be completely healed. Conclusion: This is a rare case of gluteal fistula as a complication of SSLS procedure. In this case, the suspected retained suture causing the fistula was not identified; however, the fistula was still able to heal.
Introduction
Pelvic organ prolapse (POP) is a common benign condition that affects the quality of life of many women. It is estimated that women in the United States have a
13% lifetime risk of undergoing surgery for POP [1]. Sacrospinous ligament suspension is a procedure carried out trans-vaginally to correct apical prolapse at the time of hysterectomy or in patients with post hysterectomy vaginal vault prolapse.
The sacrospinous ligament courses laterally from the ischial spine and attaches medially to the sacrum. In a sacrospinous ligament suspension procedure (SSLS), the ligament can be approached via the anterior or posterior vaginal compartment. Delayed absorbable or permanent sutures are used, and the first suture is placed 2 centimeters medial to the ischial spine, with one or two additional sutures placed at 1-centimeter increments medial to the initial suture. The planned vaginal apex is then lifted and the sutures are used to secure the apex.
Serious complications are rare after SSLS, but well- documented complications include infection such as cystitis, abscesses, and pain, and more severe complications including rectal injury and hemorrhage [2]. To our knowledge, there are only 3 reported cases in the literature regarding fistula as a complication of sacrospinous ligament suspension surgery [3, 4, 5]. We seek to illustrate an additional case of gluteal fistula following SSLS that resolved following an exam under anesthesia and washout.
Case Illustration
A 48-year-old woman, with history of a posterior colporrhaphy and perineorrhaphy 3 years prior, underwent a vaginal hysterectomy, bilateral salpingectomy, anterior and posterior colporrhaphy with perineorrhaphy, sacrospinous ligament suspension and cystoscopy for stage 4 pelvic organ prolapse. During the SSLS portion of the procedure, a posterior approach was taken to visualize the sacrospinous ligament. Once identified, a #0 prolene was placed through the sacrospinous ligament and the right side of the vagina was anchored to the right uterosacral ligament. The posterior repair was then carried out in a normal fashion. The case itself was noted to be uncomplicated.
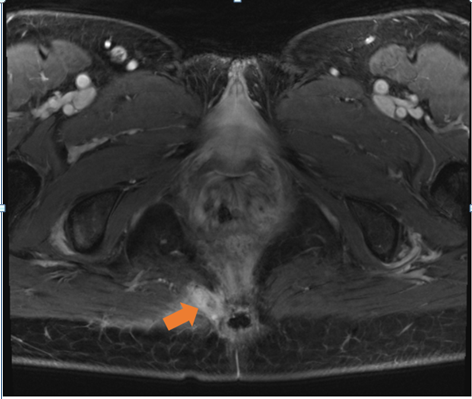
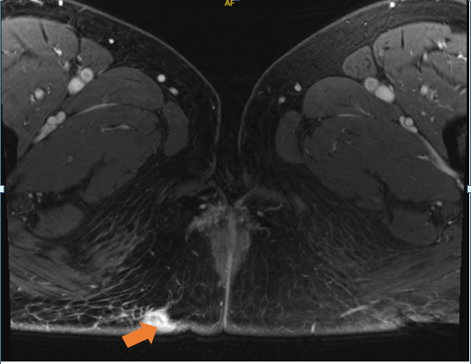
One year later, the patient presented to a colorectal surgeon with drainage from her right buttock. She reported that she had visited the emergency room 3 times in the past 6 months for a right buttock abscess, and each time it was incised and drained, and she received antibiotics. A right gluteal fistula was noted on exam, and an MRI was performed which showed a predominantly collapsed sinus tract extending from the sacrum to the right gluteal fold and right piriformis muscle with no associated abscess (Figures 1 & 2). Recurrent stage IV prolapse was also noted. The fistula was thought to be caused by the prolene suture that was used for the SSLS, and an exam under anesthesia was performed with collaboration of urogynecology and colorectal surgery with planned removal of offending suture.
In the operating room, a posterior approach was reproduced and the right sacrospinous ligament was identified. However, the prolene suture was not visualized at this location. At this point, the fistula tract was outlined with a Kelly clamp and noted to be more lateral to the sacrospinous ligament. It was thought that the prolene suture may have been placed lateral and inferior to the ligament, or there may have been migration of the suture. After gentle probing through the fistulous tract, the prolene suture was unable to be found. Decision was made to copiously irrigate the area with gentamicin and cefazolin diluted in normal saline. Bacitracin was also applied to the fistula tract.
At her postoperative visit, the prior site of the patient’s right gluteal fistula was noted to be well-healed and epithelialized, with no drainage or erythema. Of note, for the patient’s recurrent prolapse, she initially was to undergo interval minimally invasive sacrocolpopexy, however, on her last visit, she declined further surgical management, citing mistrust of female pelvic reconstructive surgery.
Discussion
Sacrospinous ligament suspension is a commonly performed procedure for treating apical prolapse, and serious complications are uncommon. Infectious complications are most common, with cystitis occurring in up to 4.5% of patients [1]. Other complications include urinary retention, post-operative pain, hemorrhage, and nerve damage. Fistula formation is not often cited as a complication, and to our knowledge, there are only a handful of case reports regarding fistulas as a complication.
When performing an SSLS procedure, either permanent sutures or delayed absorbable sutures may be used. Synthetic permanent sutures, such as prolene, are relatively inert, and provoke minimal tissue reaction. In our case, as well as the cases delineated by Gafni-Kane et al. and Costa et al., synthetic non-absorbable sutures were used for the SSLS procedure [3, 5]. However, in light of some postoperative complications, including nerve entrapment and persistent buttock pain, some sources believe that delayed absorbable sutures may be more advantageous, given that they dissolve and also may be easier to remove in case of complications [6]. In all case reports of fistula formation after SSLS procedure, the suture was thought to be the offending agent.
In cases where fistula formation is thought to be due to a foreign body, management usually focuses upon removal of the offending agent, followed by repair of fistula by either fistulotomy or fistulectomy. In our case, we first attempted to visualize and retrieve the suture through reproducing the posterior approach used to perform the SSLS procedure, however we were unable to identify the suture. Of note, Gafni Kane, et al. and Costa et al. also first attempted to retrieve the suture by reproduction of the vaginal dissection, but failed.
We then attempted to retrieve the suture through probing the fistula, but were unable to do so. In the other case reports mentioned, the offending suture was removed with subsequent resolution of the fistula. However, we present a case in which the fistula was able to heal after an antibiotic washout despite being unable to remove the non-absorbable suture used for the SSLS procedure.
Conclusion
Fistulas are an uncommon complication after sacrospinous fixation, with only few case reports available in the literature. In prior cases, the offending suture was unable to be visualized through reproducing the initial vaginal approach and was usually retrieved by following the fistulous tract. In our case, the fistula was able to heal without removal of the offending suture.
References
-
Beer M, Kuhn A (2005) Surgical Techniques for Vault Prolapse: A Review of the Literature. Eur J Obstet Gynecol Reprod Biol 119(2): 144-55.
-
Wu JM, Matthews CA, Conover MM, Pate V, Jonsson Funk M (2014) Lifetime Risk of Stress Urinary Incontinence or Pelvic Organ Prolapse Surgery. Obstet Gynecol 123(6): 1201-1206.
-
Gafni-Kane A, Goldberg RP, Spitz JS, Sand PK (2011) Extrasphincteric Perianal Fistulae after Sacrospinous Fixation for Apical Prolapse. Obstet Gynecol 117(2): 438-440.
-
Kadam PD (2015) Rectocutaneous Fistula with Transmigration of the Suture: A Rare Delayed Complication of Vault Fixation with the Sacrospinous Ligament. Int Urogynecol J 27(1): 155-157.
-
Costa MM, Anna MB, Josep PS, Judith LJ, Natalia HT, et al. (2021) Gluteal-Sacrospinous-Vaginal Fistula as a Complication of Sacrospinous Ligament Fixation after a Vault Prolapse: A Case Report. Journal of Clinical Images and Medical Case Reports 2(6).
-
Rock JA, Howard WJ, Te Linde RW (2011) Section VI Surgery for Pelvic Floor Disorders Transvaginal Apical Suspensions for Uterovaginal Prolapse. In Telinde’s Operative Gynecology 501-6. Lippincott Williams & Wilkins.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era