Impact of MRI Defectography on Surgical Approach in Patients with Pelvic Floor Dysfunction
Background: Surgical treatment of pelvic floor dysfunctions carries frequent recurrences. The aim of the study was to evaluate the role dynamic MRI defecography in demonstrating the underlying anatomic and pathophysiologic background of pelvic floor disorders in these patients to guide surgical approach and minimize failure. Methods: Patients underwent perineal examination, conventional defecography, anorectal manometry, colonoscopy, and MRI defecography. The different pelvic floor morphologies were recorded. The type of treatment, whether conservative or surgical, was also recorded. Results: In total, 33 patients were included, with mean age 46.78 ± 10.51 years and the majority (69.7 %) of patients were female. 31 patients (93.9 %) with perineal descent, 21 patients (63.6 %) with rectoceles , 19 patients (57.57 %) with cystoceles, 4 patients (12.1 %) with enteroceles, 15 patients (45.4 %) with intussusceptions, 14 patients (42.2 %) with uterine prolapse and 12 patients with dyskinetic puborectalis muscle. The findings of dynamic MRI defecography were consistent with clinical results in 54.54 % with additional diagnostic parameters in 45.45 % of patients. Dynamic MRI findings changed treatment decision in 15 (45.5 %) patients with surgical treatment performed in 21 patients (63.6 %) and conservative treatment in 12 patients (36.3 %). Conclusion: Dynamic MRI defecography represents an essential diagnostic procedure in females and to a lesser extent in males, especially in terms of dynamic imaging of the pelvic floor organs during defecation. In addition to the clinical assessment, dynamic MRI defecography had clinical impact in pelvic floor dysfunction and interdisciplinary treatment decisions.
Introduction and Aim of the Work
The pelvic floor is composed of three interconnected layers: endopelvic fascia, pelvic diaphragm and perineal membrane. It serves two main functions: firstly, structural support to the abdominal viscera, pelvic organs, bladder and urethra in the anterior compartment, uterus and vagina in the middle compartment (in women) and the anorectal junction in the posterior compartment [1, 2]. Secondly, constrictor mechanism to the anal canal, vagina and urethra [1, 2]. Pelvic floor dysfunction is the abnormal function of the pelvic floor that may be caused by structural abnormalities, physical trauma or underlying disease [3]. PFD presents as a broad spectrum of clinical conditions ranging from urinary/ fecal incontinence, obstructed defecation, vulvodynia, dyspareunia to frank pelvic organ prolapse [4]. Patients may often present with a combination of symptoms simultaneously [5]. The initial presenting symptoms can often be masked by concomitant pathology in another anatomical compartment that may be then unmasked after surgery, which may later complicate recovery and prognosis, leading to higher reoperation rates [6]. Detailed history and proper physical examination is the cornerstone of clinically evaluating patients with symptoms related to the pelvic floor [7].
The rate of reoperation after first pelvic floor surgery is approximately 29% [8]. To avoid such recurrence and unmasking of latent symptoms, surgery must be tailored for each patient based on the specific anatomical and structural abnormalities of the pelvic floor in conjunction with clinical status. New MRI analytical approach (static and dynamic) can provide the detailed data regarding the predominant defects in the pelvic support system, and thus guide a more tailored approach to treatment [9, 10]. The Aim of this work is to asses the impact of MRI defectography on the surgical approach in patients with PFD.
Patients and Methods
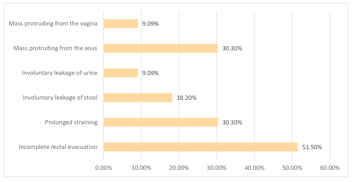
The current study included 33 patients with pelvic floor dysfunction (23 females 69.70 %, and 10 males 30.30%). 27 patients (81.80%) presented with obstructed defecation syndrome (4 patients out of 27 presented also with rectal prolapse) and 6 patients (18.20%) presented with anal Incontinence (3 patients out of 6 presented also with rectal prolapse and 3 patients out of 6 presented with rectal prolapse, uterine prolapse and urinary incontinence). The mean age of the patients was 46.78 ± 10.51 years. All Patients were enrolled from outpatient clinics of the Colorectal surgery department, Kasr Al- Aini hospital, Faculty of medicine, Cairo University. Inclusion criteria where of that male and female patient over the age of 16 with pelvic floor dysfunction. To be excluded in the study, patients had to meet the following criteria, (1) patients under the age of 16, (2) patients with a previous history of anorectal surgery, (3) patients with intestinal/colonic inertia, (4) Patients with polyp, tumor, or stricture, (5) patients with absent recto- anal inhibitory reflex (RAIR).
Methods
The Cairo University, Kasr Al-Aini Research Ethics Committee, institutional-review board approved this study. Each patient was informed of the planned examinations in a preliminary talk and gave their written informed consent in advance. Preoperative evaluation for all 33 patients was done. The evaluation included history taking (Cleveland constipation score & Wexner incontinence scores were used for patients with obstructed defecation and anal incontinence respectively) examining in Left lateral, lithotomy, or squatting positions (in some cases to show the rectal prolapse) [11]. Colonoscopy, colon transit time, anorectal manometry and conventional defecography were used in patients’ assessment whenever indicated.
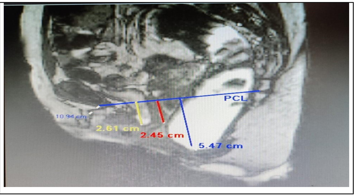
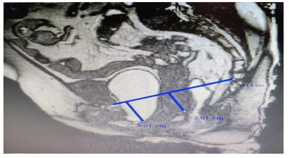
All patients with chronic constipation were subjected to colonoscopy to diagnose any contributing abnormalities. Patients with chronic constipation who did not have a desire to defecate for more than one week were subjected to colon motility assessment by colon transit time. Anorectal manometry with eight-channel manoetry smartlab was used to exclude any patient with absent recto-anal inhibitory reflex (RAIR) and in patients with suspicion for non-relaxing puborectalis with increase in anal pressures. Conventional defectography was done for all patients. In all women, a gynecological assessment was performed. The findings collected from the above examinations/investagations were interpreted in terms of clinical findings as well as the clinical diagnosis. The plan of management, based on these findings, was recorded and compared to that of MRI defectography. MRI defecography was done for all patients with comparison of its findings with clinical findings and changes in the management plan based on MRI defectography a finding was recorded (Figures 1-3).
Dynamic Magnetic Resonance Imaging Defecography Patient Preparation
- All patients underwent cleansing rectal enema the night before MR imaging.
- No fasting pre-examination was required.
- Patients were asked not to void 2 hours before the examination.
- Explanation of the technique and training of the patients was done prior to the examination by a doctor to ensure the patient understanding of how to preform Valsalva maneuver properly.
- Patients were examined in the supine position with the knees elevated (eg, on a pillow with firm consistency) to simulate a sitting position. This was found to facilitate the straining and evacuation process.
- A pad was placed under the patient to add more comfort to when evacuating the rectum.
- The patient was instructed to squeeze as if trying to prevent escape of feces or urine and hold this position for the duration of the sequence. For maximum straining, the patient was instructed to bear down as though constipated and trying to defecate. For the evacuation phase, patients were instructed to repeat the evacuation process until the rectum is emptied.
- The rectum should have been distended to visualize the anorectal junction (ARJ), rectoceles and intussusceptions. Ultrasound gel was used to distend the rectum with the amount varying between 120 to 250 cc according to patients individual tolerance (sensing an inevitable urge to dedicate).
- Patients were informed that the evacuation phase is important for a complete diagnostic study [12].
Dynamic MRI Defecography Protocol
MRI was performed on a 1.5 Tesla (Achieva; Philips Medical Systems, Best, the Netherlands), using a pelvic phased array coil which is the most agreed- upon field strength. The coil was centered low on the pelvis to ensure complete visualization of prolapsed organs. No oral or intravenous contrast agent was administered. The MRI protocol consisted of static MR sequences and dynamic MR sequences. Dynamic sequences entailed imaging during straining, squeezing and during evacuation/defecation. High resolution T2-weighted images (T2WI) (e.g. Turbo Spin Echo, TSE; Fast Spin Echo, FSE; Rapid Acquisition with Relaxation Enhancement, RARE) in three planes were used for the static images. Steady state (e.g., FISP, GRASS, FFE, PSIF, SSFP, T2- FFE) or balanced state free precession sequence (e.g., trueFISP, FIESTA, B-FFE) via a sagittal plane was used for dynamic sequences (squeezing and straining) and evacuation sequence. The dynamic sequence didn’t exceed 20 seconds each as breath holding was required. The evacuation sequence was repeated until the rectum was emptied to exclude intussusception (total time duration around 2-3 minutes). Dynamic MR imaging during evacuation was mandatory as certain abnormalities and full extent of POP was only visible during evacuation [12].
Image Analysis
MR study of the pelvic floor included analysis of the static images for the detection and classification of structural abnormalities, dynamic images were analyzed with regard to functional abnormalities that were assessed by metric measurements of the three compartments of the pelvic floor. The measurements helped to recognize and grade the extent of POP and grade anterior rectoceles and enteroceles [12].
Measurements
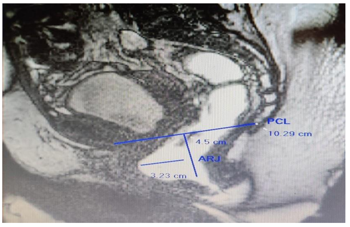
Defecography phase: The pubococcygeal line (PCL) was used as the reference from which pelvic organ descent was measured during evacuation. The PCL was drawn on the mid sagittal plane from the inferior aspect of the pubic symphysis to the last coccygeal joint. After defining the PCL, the distance from each reference point was measured perpendicularly to the PCL
• Anterior compartment descent: Urinary bladder base was used as the reference point, the distance between the most inferior aspect of the bladder base and the PCL was measured. Cystoceles were graded according to the “Rule of 3”; grade I (1-3 cm), grade II (3-6 cm) and grade III (> 6 cm below the PCL).
• Middle compartment descent: Anterior cervical lip was used as the reference point, or the vaginal vault (in case of previous hysterectomy). Measurements were taken from the PCL to the relevant reference point. Uterine prolapse was graded according to the “Rule of 3”; grade I (1-3 cm), grade II (3-6 cm) and grade III (> 6 cm) below the PCL). Enterocoeles were defined when small bowel loops prolapsed into the recto-genital space beyond the PCL during evacuation. Peritoneoceles were diagnosed when the peritoneum herniated into the rectovaginal space and beyond the PCL but with no associated bowel herniation.
• Posterior compartment descent: Anorectal junction was used as the reference point. Descending perineum syndrome (pelvic floor descent) was defined as descent of ARJ > 3 cm below the PCL. Classification; grade I between 3 to 5 cm below the PCL, grade II more than 5 cm below the PCL. An anterior rectal wall bulge extending beyond a line, drawn through the anterior wall of the anal canal and upward, of greater than 2 cm anterior was described as a rectocele. Rectoceles were graded as grade I (≤2 cm), grade II (>2-4 cm) and grade III (>4 cm). Rectal intussusception and prolapse was classified as “recto-rectal” intussusception, when rectal in-folding descends no lower than the proximal limit of the anal canal, and “recto-anal” intussusception when rectal in- folding reached the anal canal. “Rectal prolapse” was diagnosed when the rectum protruded beyond the anal canal. Presence of abnormal puborectalis contraction was diagnosed when effacement of the puborectalis muscle was absent during evacuation attempts.
Dynamic phase: Quantification of pelvic floor relaxation was achieved via three measurements: (1) sagittal, axial and coronal dynamic scans, (2) the levator plate angle, (3) the transverse width of the levator hiatus and the iliococcygeus angle, at maximum straining.
- Levator plate angle (LPA) is enclosed between the levator plate and the PCL on the sagittal plane at maximum straining.
- Width of the levator hiatus (WLH) is enclosed between the puborectalis muscle slings on the axial plane at maximum straining.
- Iliococcygeus angle (ILCA) is measured on the coronal plane, between the iliococcygeus muscle and the transverse plane of the pelvis in posterior coronal images at the level of the anal canal.
Static phase: Anal sphincter complex evaluation for the presence of sphincteric defects, scarring, and gross assessment of the sphincter bulk. Puborectalis muscle defects are recognizable by disruption of the normal symmetrical appearance of the muscle sling or of its attachment to the symphysispubis. Iliococcygeus muscle was assessed for loss of the normal symmetric appearance of its muscle slings or disruption of its attachment to the obturator internus muscle in the coronal plane [12].
Treatment: Surgical treatment was performed in 21 patients out of the initial 33, 9 patients received trans- perineal repair (e.g., Stapled trans-anal rectal resection, Altemeir, levatoplasty) and 12 patients received combined trans- abdominal and trans- perineal repair (Pelvic organ prolapse suspension [POPS], ventral mesh rectopexy, STARR, Altemeir, levatoplasty). Conservative treatment (Biofeedback) was used in 12 patients.
Statistical methods: A regression analysis was used to comparison between quantitative means. For comparison of qualitative variables, McNemar test was used. Data will be summarized using Mean and SD for quantitative variables, and number and percent for qualitative variable. All collected data was revised for completeness and accuracy. Pre coded data was entered on a computer system using the statistical package of social science software program, version 23 (SPSS). P-value equal to or less than 0.05 was considered of statistically significant (Figures 1 & 2).
Results
This study included 33 patients with pelvic floor dysfunction (23 females 69.70 %, and 10 males 30.30%). 27 patients (81.80%) presented with obstructed defecation syndrome (4 patients out of 27 presented with superimposed rectal prolapse) and 6 patients (18.20%) presented with anal Incontinence (3 presented with superimposed rectal prolapse only, and 3 presented with superimposed rectal prolapse, uterine prolapse and urinary incontinence) (Tables 1 & 2)(Figure 3).
(a)
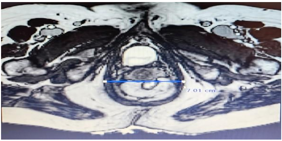
(b) Figure 3: A 57-year-old woman with rectal prolapse and anal incontinence. T2-weighted images (T2WI). (a) sagittal plane during defecation phase showed complete rectal prolapse and cystocele and uterine prolapse. (b) axial plane during dynamic phase showed abnormal widening of the levator hiatus.
| Cleveland constipation score | Number of patients | % |
|---|---|---|
| Oct-14 | 5 | 18.51% |
| 15-19 | 12 | 44.44% |
| 20-25 | 10 | 37.03% |
Table 1: Cleveland constipation score in patients with obstructive defecation26.
| Wexner incontinence score | Number of patients | % |
|---|---|---|
| Oct-14 | 4 | 66.66% |
| 15-20 | 2 | 33.33% |
Table 2: Wexner incontinence score in patients with incontinence 27.
On clinical evaluation of patients with obstructed defecation syndrome, rectal prolapse was detected in 4 patients (14.81%), rectocele was detected in 13 patients (48.14%), intussusception in 12 patients (44.44%), perineal descent in 7 patients (25.92 %), and non-relaxing puborectalis in 7 patients 25.92% (Table 3).
| Clinical | N | % |
|---|---|---|
| Cystocele | 0 | 0 |
| Uterine prolapse | 0 | 0 |
| Rectal prolapse | 4 | 14.81 |
| Rectocele | 13 | 48.14 |
| Intussusception | 12 | 44.44 |
| Perineal descent | 7 | 25.92 |
| Non-relaxing puborectalis | 7 | 25.92 |
Table 3: Clinical findings in patients with obstructed defecation.
On clinical evaluation of patients with Anal incontinence, uterine prolapse was detected in 3 patients (50 %) while rectal prolapse and rectoceles were detected in all patients (100%). Intussusception was detected in 3 patients (50.0 %) and 5 patients (83.33 %) had perineal descent (Table 4).
| Clinical | N | % |
|---|---|---|
| Cystocele | 0 | 0 |
| Uterine prolapse | 3 | 50 |
| Rectal prolapse | 6 | 100 |
| Rectocele | 6 | 100 |
| Intussusception | 3 | 50 |
| Perineal descent | 5 | 83.33 |
| Non-relaxing puborectalis | 0 | 0 |
Table 4: Clinical findings in patients with obstructed incontinence.
Anterior Compartment
Cystocele in 13 out of 27 patients (48.14 %) [3.23 ± 1.804 cm], Grade I cystocele [1-3cm] was detected in 6 patients (22.22%) and grade II cystocele [3-6cm] in 7 patients (25.92 %).
Middle Compartment
Uterine prolapse was found in8 out of 27 patients (29.62 %) [3.75±1.98 cm], grade I [< 3cm] uterine prolapse was found in 3 patients (11.11%) and grade II [3-6 cm] in 5 patients (18.51%). Enterocele was present in only 2 patients (7.40%).
Posterior Compartment
ARJ descent was found in 25 out of 27 patients (92.95 %) [4.84±1.88 cm]. It showed grade I ARJ descent [3-5 cm] in 7 patients (25.92%), grade II [> 5cm] ARJ descent in 12 patients (44.44%) and grade III in 6 patients (22.22 %). Rectocele was detected in 16 out of 27 patients (59.25%) [3.09±0.955 cm], grade I rectocele [<2cm] was found in 3 patients (11.11 %) and grade II rectocele [2-4cm] in 13 patients (48.18%).
Intussusception was detected in 12 patients (44.44%) and dyskinetic puborectalis was found in 12 patients (44.44%) (Table 5).
Dynamic MRI Findings in Patients with Obstructed Defecation Syndrome
Wide levator plate angle was found in 9 out of 27 of patients (33.33 %) [ 21.11 ± 3.314(cm)]. Abnormal widening of the levator hiatus (> 4.5cm) was detected in 10 out of 27 patients (37.03%) [5.67 ± 0.654]. Elongation of the ileococcygeus angle (> 32) was detected in 9 out of 27 of patients (33.33 %) [39.77 ± 3.764] (Table 6).
Static MRI Findings in Patients with Obstructed Defecation Syndrome
The puborectalis muscle was found thinned in 5 patients (18.5 %) while the Ileococcygeus muscle was found thinned in 2 patients (7.40 %). Level II endopelvic Fascia defect was detected in 5 patients (18.5 %) and in 1 patient 3.70 % it was associated with a level III endopelvic fascia defect. Anal sphincter complex was intact in all patients.
| MRI defecography | ||||
|---|---|---|---|---|
| Cystocele | N | % | mean ±SD (cm) | |
| Anterior compartment | Grade I | 6 | 22.22 | 3.23±1.804 |
| Grade II | 7 | 25.92 | ||
| Grade III | 0 | 0 | ||
| Cystocele | N | % | ||
| Absent | 14 | 51.85 | ||
| Present | 13 | 48.14 | ||
| Uterine prolapse | N | % | ||
| Middle compartment | Grade I | 3 | 11.11 | 3.75±1.98 |
| Grade II | 5 | 18.51 | ||
| Uterine prolapse | N | % | ||
| Absent | 19 | 70.37 | ||
| Present | 8 | 29.62 | ||
| Enterocele | ||||
| Absent | 25 | 92.59 | ||
| Present | 2 | 7.4 | ||
| ARJ descent | N | % |
Table 5: MRI defectography findings in patients with ODS.
| Posterior compartment | Grade I | 7 | 25.92 | 4.84±1.88 |
|---|---|---|---|---|
| Grade II | 12 | 44.44 | ||
| Grade III | 6 | 22.22 | ||
| ARJ descent | N | % | ||
| Absent | 2 | 7.4 | ||
| Present | 25 | 92.59 | ||
| Rectocele | N | % | ||
| Anorectal dysfunction | Grade I | 3 | 11.11 | 3.09±0.95 |
| Grade II | 13 | 48.14 | ||
| Rectocele | N | % | ||
| Absent | 11 | 40.74 | ||
| Present | 16 | 59.25 | ||
| Intussusception | N | % | ||
| Absent | 15 | 55.55 | ||
| Present | 12 | 44.44 | ||
| Dyskinetic puborectalis | N | % | ||
| Absent | 15 | 55.55 | ||
| Present | 12 | 44.44 |
Table 6: MRI defectography findings in patients with ODS.
| Levator plate angle | N | % | Mean ± SD (cm) | |
|---|---|---|---|---|
| Dynamic MRI | normal | 18 | 66.66 | |
| Wide angle ( >15 ) | 9 | 33.33 | 21.11±3.314 | |
| Levator Hiatus | N | % | ||
| Normal | 17 | 62.96 | ||
| Abnormal widening( > 4.5 cm) | 10 | 37.03 | 5.67 ± 0.654 | |
| Ileococcygeus angle | N | % | ||
| normal | 18 | 66.66 | ||
| Elongation ( > 32 ) | 9 | 33.33 | 39.77±3.764 | |
| Puborectalis muscle | N | % | ||
| Preserved | 22 | 81.48 | ||
| Static MRI | Thinned | 2 | 7.4 | |
| Thinned Rt sling | 3 | 11.11 | ||
| Ileococcygeus muscle | N | % | ||
| Preserved | 25 | 92.59 | ||
| thinned | 2 | 7.4 | ||
| Anal sphincter complex | N | % | ||
| Preserved | 27 | 100 | ||
| Thinned or torn | 0 | 0 | ||
| Endopelvic Fascia | N | % | ||
| normal | 21 | 77.77 | ||
| Level II defect | 5 | 18.51 | ||
| Level III defect | 1 | 3.7 |
Table 7: Dynamic and static MRI findings in patients with ODS.
MRI Defecography Findings in Patients with Anal Incontinence
Out of 6 patients who were diagnosed with anal inconvenience, the following was found with respect to anatomical compartments and MRI phases.
Anterior compartment: Cystocele was present in 6 patients (100 %) [4.33±1.05cm], grade II cystocele (3-6cm) in 4 patients (66.66 %) and grade III cystocele [> 6cm] in 2 patients (33.33 %).
Middle compartment: Uterine prolapse was found in 6 patients (100 %) [4.5±1.70 cm], grade I (< 3cm) uterine prolapse in 1 patient (16.66%) and grade II [3-6 cm] in 5 patients (83.33%), finally enterocele in 2 patients (33.33%).
Posterior compartment: ARJ descent was found in 6 patients (100 %) [6.16±0.687 cm] with all of them being of grade II [> 5 cm]. Rectocele was detected in 5 patients (83.33%) [2.4±1.02 cm], grade I rectocele [<2 cm] in 3 patients (50.0 %) and grade II rectocele [2-4 cm] in 2 patients (33.33%). Intussusception detected in 3 patients (50.0 %) (Table 7).
Dynamic MRI Findings in Patients with Anal Incontinence: Out of 6 patients diagnosed with anal incontinence, 4 (66.66 %) had a wide levator plate angle [19.5 ± 0.866 cm], 5 (83.33%) an abnormal widening of the levator hiatus [> 4.5cm] [5.6 ± 0.583 cm] and 3 (50.0 %) had elongation of the ileococcygeus angle [> 32 cm] [40 ± 4.0824 cm].
Static MRI findings in patients with anal incontinence: The puborectalis muscle, Ileococcygeus muscle and Anal sphincter complex were intact in all patients. Level II endopelvic Fascia defect was detected in 5 patients (83.33 %) and one patient (16.66 %) had findings consistent with a level III fascia defect. (Table 8)
| MRI defecography | ||||
|---|---|---|---|---|
| Cystocele | N | % | mean ± SD (cm) | |
| Anterior compartment | Absent | 0 | 0 | 4.33±1.05 |
| Grade I | 0 | 0 | ||
| Grade II | 4 | 66.66 | ||
| Grade III | 2 | 33.33 | ||
| Cystocele | N | % | ||
| Absent | 0 | 0 | ||
| Present | 6 | 100 | ||
| Uterine prolapse | N | % | ||
| Middle compartment | Absent | 0 | 0 | 4.5±1.70 |
| Grade I | 1 | 16.66 | ||
| Grade II | 5 | 83.33 | ||
| Uterine prolapse | N | % | ||
| Absent | 0 | 0 | ||
| Present | 6 | 100 | ||
| Enterocele | N | % | ||
| Absent | 4 | 66.66 | ||
| Present | 2 | 33.33 | ||
| ARJ descent | N | % |
Table 8: MRI defectography findings in patients with anal inconvenience.
| Posterior compartment | Absent | 0 | 0 | 6.16±0.687 |
|---|---|---|---|---|
| Grade I | 0 | 0 | ||
| Grade II | 6 | 100 | ||
| Grade III | 0 | 0 | ||
| ARJ descent | N | % | ||
| Absent | 0 | 0 | ||
| Present | 6 | 100 | ||
| Rectocele | N | % | ||
| Anorectal dysfunction | Absent | 1 | 16.66 | 2.4±1.02 |
| Grade I | 3 | 50 | ||
| Grade II | 2 | 33.33 | ||
| Rectocele | N | % | ||
| Absent | 1 | 16.66 | ||
| Present | 5 | 83.33 | ||
| Intussusception | N | % | ||
| Absent | 3 | 50 | ||
| Present | 3 | 50 | ||
| Dyskinetic puborectalis | N | % | ||
| Absent | 6 | 100 | ||
| Present | 0 | 0 |
Table 9: MRI defectography findings in patients with anal inconvenience.
| Levator plate angle | N | % | Mean ± SD(cm) | |
|---|---|---|---|---|
| Dynamic MRI | normal | 2 | 33.33 | |
| Wide angle ( >15 ) | 4 | 66.66 | 19.5 ± 0.866 | |
| Levator Hiatus | N | % | ||
| Normal | 1 | 16.66 | ||
| Abnormal widening( > 4.5 cm) | 5 | 83.33 | 5.6 ± 0.583 (cm) | |
| Ileococcygeus angle | N | % | ||
| normal | 3 | 50 | ||
| Elongation ( > 32 ) | 3 | 50 | 40 ± 4.0824 | |
| Puborectalis muscle | N | % |
Table 10: Dynamic and static MRI findings in patients with anal incontinence.
| Static MRI | Preserved | 6 | 100 | |
|---|---|---|---|---|
| Thinned | 0 | 0 | ||
| Thinned Rt sling | 0 | 0 | ||
| Ileococcygeus muscle | N | % | ||
| Preserved | 6 | 100 | ||
| thinned | 0 | 0 | ||
| Anal sphincter complex | N | % | ||
| Preserved | 6 | 100 | ||
| Thinned or torn | 0 | 0 | ||
| Endopelvic Fascia | N | % | ||
| normal | 1 | 16.66 | ||
| Level II defect | 5 | 83.33 | ||
| Level III defect | 1 | 16.66 |
Table 11: Dynamic and static MRI findings in patients with anal incontinence.
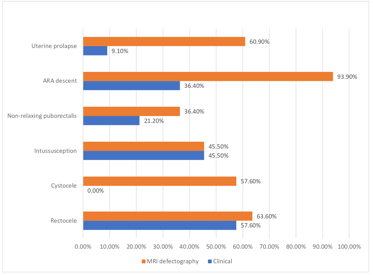
Comparison between clinical and dynamic MRI diagnosis in patients with PFD Radiological diagnosis was consistent with clinical diagnosis in 18 patients (54.54%), however, in 15 patients (45.45 %) radiological diagnosis provided additional information, and thus a difference in diagnosis. This difference was consistent among the diagnosis of cystoceles (Anterior compartment), uterine prolapse, enterocele (middle compartment), and ARJ descent. The difference between dynamic MRI defecography over clinical diagnosis in rectocele and dyskinetic puborectalis lacked statistical significance. There was no difference in diagnosing intussusception as it was achieved via conventional defecography (Table 9).
| Clinical | Radio(MRI) | ||||
|---|---|---|---|---|---|
| Absent | Present | Absent | Present | p value | |
| Cystocele | 33(100.0) | 0(0.00) | 14(42.4) | 19(57.6) | <0.001* |
| Uterine prolapse | 30(90.9) | 3(9.1) | 9(39.1) | 14(60.9) | 0.001* |
| enterocele | 33(100.0) | 0(0.00) | 29(87.87) | 4(12.12) | <0.001* |
| ARJ descent | 21(63.6) | 12(36.4) | 2(6.1) | 31(93.9) | <0.001* |
| Rectocele | 14(42.4) | 19(57.6) | 12(36.4) | 21(63.6) | 0.5 |
| Intussusception | 18(54.5) | 15(45.5) | 18(54.5) | 15(45.5) | 1 |
| Non-relaxing puborectalis | 26(78.8) | 7(21.2) | 21(63.6) | 12(36.4) | 0.06 |
Table 12: Comparison between clinical and dynamic MRI diagnosis in patients with PFD.
| Number of compartments affected per patient | Number of patients | % |
|---|---|---|
| One | 4 | 14.81 |
| Two | 5 | 18.51 |
| Three | 18 | 66.66 |
Table 13: Compartments affected per-patient with obstructed defecation.
Patients who suffered from obstructed defecation were found to have multi-compartment involvement, as 23 out of the 27 patients (85.18%) with obstructed defecation had more than one compartment affected; 5 (18.51%) had two compartments involved, and 18 (66.66 %) had three compartments involved (Table 10).
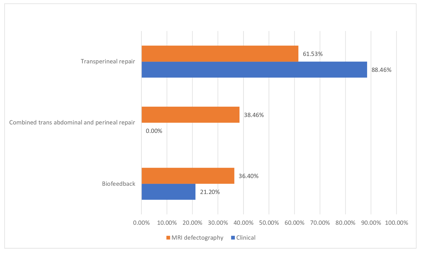
Changes in treatment decision and role of dynamic mri defecography: Based on clinical findings, conservative management (biofeedback) was scheduled for 7/33 patients (21.21%) and surgical treatment for 26/33 patients (78.78%). 23 (88.46%) out of the 26 who were assigned to surgical treatment were scheduled for trans- perineal approach and the remaining 3 patients (11.53%) were scheduled for trans-abdominal repair. Conversely, additional findings detected via dynamic MRI defecography affected the surgical approach significantly (P- value 0.004), specifically from trans-perineal approach to combined trans- abdominal and trans- perineal repair in 7 patients and from trans-abdominal repair to combined trans-abdominal and trans-perineal repair in 3 patients. This difference occured primarily in female patients with additional findings in the anterior compartment (cystocele), middle compartment (uterine prolapse, enterocele) and abnormal widening of levator hiatus. Furthermore, dynamic MRI defecography changed the decision from surgery to biofeedback in 5 patients (19.23%), where dyskinetic puborectalis was additionally detected (Tables 11 & 12).
| Radio vs Clinical | Biofeedback | Trans perineal repair | Combined trans abdominal &perineal repair | |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | P value | |
| Biofeedback | 7(100) | 0(0) | 0(0) | 0.063 |
| Trans abdominal repair | 0(0) | 0(0) | 3(100) | 0.065 |
| Trans perineal repair | 5(21.73) | 11(47.82) | 7(30.43) | 0.004* |
Table 14: Decision based on clinical findings and radiological findings.
| Patient | Clinical findings | Decision | Additional MRI findings that impacted surgical decision | Decision |
|---|---|---|---|---|
| 1 | complete Rectal prolapse (with incontinence), uterine prolapse | ARJ descent, uterine prolapse, cystocele, abnormal widening of levator hiatus | ||
| Surgery Trans Abdominal approach | Surgery Transabdominal combined repair | |||
| 2 | complete Rectal prolapse(with incontinence), uterine prolapse | Rectocele, ARJ descent, cystocele, uterine prolapse, enterocele, abnormal widening of levator hiatus. | ||
| 3 | complete Rectal prolapse(with incontinence), uterine prolapse | Rectocele, ARJ descent, cystocele, uterine prolapse, abnormal widening of levator hiatus. | ||
| 4 | Rectocele, perineal descent, Intussusception | Rectocele, ARJ descent, Intussusception, cystocele, uterine prolapse, abnormal widening of levator hiatus. | ||
| Surgery Trans- perineal approach |
Table 15: Role of MRI defectography and changes in surgical approach (red color indicates additional findings).
- 5
- Rectocele, perineal descent.
- Rectocele, ARJ descent,
- Intussusception, cystocele, uterine prolapse, enterocele, abnormal widening of levator hiatus.
- Rectocele, ARJ descent, Intussusception, cystocele, uterine prolapse, enterocele, abnormal widening of levator hiatus.
- 6
- Rectocele, perineal descent,
- Intussusception
- 7
- Rectocele, perineal descent.
- Rectocele, ARJ descent , cystocele,uterine prolapse, abnormal widening of levator hiatus.
- Rectocele, ARJ descent, Intussusception, cystocele, uterine prolapse, abnormal widening of levator hiatus.
- 8
- Rectocele , perineal descent, Intussusception
- 9
- Rectocele, Intussusception
- Rectocele, ARJ descent, cystocele, uterine prolapse, abnormal widening of levator hiatus.
- 10
- Rectocele, perineal descent
- Rectocele, ARJ descent, Intussusception, cystocele, uterine prolapse, enterocele, abnormal widening of levator hiatus.
- 11
- Rectocele
- Rectocele, ARJ descent, Dyskinetic puborectalis surgery Transperineal approach
- 12
- Intussusception
- ARJ descent, Dyskinetic puborectalis
- 13
- Intussusception
- ARJ descent, Dyskinetic puborectalis
- 14
- Rectocele
- Rectocele, ARJ descent, Dyskinetic puborectalis
- 15
- Rectocele
- Rectocele, ARJ descent, Dyskinetic puborectalis
Table 16: Role of MRI defectography and changes in surgical approach (red color indicates additional findings).
Impact of MRI defecography on surgical decision in female patients: There was a statistically significant change in treatment decision for female patients after radiological findings in comparison to treatment decision based on clinical findings (p-value<0.001). 19 out of 23 females (82.60%) were scheduled for trans-perineal approach while 3 patients (13.04%) were scheduled for trans-abdominal repair. However, with the detection of additional findings via dynamic MRI defecography a significant changed in the surgical decision was observed, from trans-perineal approach to combined trans-abdominal and trans-perineal repair in 7 patients (30.43%), trans-abdominal repair to combined trans-abdominal and trans- perineal repair in 3 patients (13.04%) and from surgery to biofeedback in 4 patients (17.39%) (Table13).
| Radio Vs Clinical | Trans perineal repair | Combined trans abdominal and perineal repair | Total | |
|---|---|---|---|---|
| N (%) | N% | N (%) | p value | |
| Biofeedback | 0(0) | 0(0) | 1(100) | 0.125 |
| Trans abdominal repair | 0(0) | 3(100) | 3(100) | 0.002 |
| Trans perineal repair | 8(42.10) | 7(36.84) | 19(100) | <0.001 |
Table 17: Decisions among females.
Impact of MRI defecography on surgical decision in male patients: There was no difference in treatment decision for male patients after radiological findings in comparison to treatment decisions made on the basis of clinical findings (p value 1). However, in 1 patient (25%) treatment course changed from operative to conservative (Biofeedback) (Table 14).
| Radio Vs Clinical | Trans perineal repair | Total | |
|---|---|---|---|
| N (%) | N (%) | p value | |
| Biofeedback | 0(0) | 6(100) | 1 |
| Trans perineal repair | 3(75) | 4(100) | 1 |
Table 18: Decisions among males.
Discussion
Pelvic floor dysfunction is the abnormal function of the pelvic floor that may be caused by structural abnormalities, physical trauma or underlying disease, leading to a broad spectrum of clinical conditions such as urinary/fecal incontinence, obstructed defecation, vulvodynia, dyspareunia and frank pelvic organ prolapse. the patient may often present with a multitude of symptoms at presentation [5]. Patients may exhibit symptoms that are specific to one anatomical compartment, however, frequently these symptoms are associated with a multi-compartmental involvement and in general pelvic floor weakness often involves all three compartments [13]. This masked concomitant pathology poses significant treatment and prognostic complications as another compartment pathology may be unmasked after surgery [6]. The coexistence of multiple compartment defects and frequent recurrence/persistent of symptoms after surgery suggest that more precise anatomic information is required before treatment. Therefore, accurate diagnosis of the coexisting abnormalities is essential in planning of the reconstructive procedures so that the risks of surgical failure, recurrence, and reoperation can be minimized [13].
In the current study, clinical diagnosis of PFD was based on the clinical examination and standard investagations, such as anorectal manometry and conventional defecography, and was compared to advanced radiological diagnostics with dynamic MRI defecography. The Magnetic resonance imaging defecography diagnosis was consistent with the clinical diagnosis in 54.54%, and thus gave more information in 45.45 %. With a similar sample size of 40 patients (31 female), Elshazly, et al. [11] showed that dynamic MRI defectography was consistent with clinical results in 72.5% with additional information being detected in 27.5% of patients, which showed that for the most part dynamic MRI defectography did not provide any benefit when compared to treatment decisions made on the clinical basis. This is consistent with these studies findings; however, the difference is much smaller for this study. Similarly, Rentsch, et al. [14] with a sample size of 20 patients (13 female), showed that, in 77.3%, treatment decisions were consistent with those based made based on clinical results and 34% gave more information in addition to clinical diagnoses. El sayed, et al. [15] found that MRI findings were consistent with clinical findings in 59.4 % and in 41.6% gave more information in addition to clinical diagnoses, they included a sample size of 29 patients (all female) and their results were the most consistent with our findings. The discrepancy between the results of both Elshazly, et al. [11] and Rentsch, et al. [14] from El sayed, et al. [15] and the results of this study can be explained by two main differences in study design. First, the sample size and distribution based on gender was consistent with this study in El sayed’s15 study only, with the Eshazly and Rentsch having significantly smaller sample sizes that were more equally distributed amongst the genders. Secondly, the basis of the inclusion criteria, Elshazly included patients with obstructed dedication only, and thus a definitive conclusion cannot be drawn on the effectiveness of MRI defectography in pelvic floor dysfunction diagnosis based on that alone.
Associated cystocele was observed in MRI defecography in 19 out of 33 (57.60 %) of patients while clinically cystocele was not detected. Elshazly, et al. [11] detected cystoceles in 5 out of 40 (12.5%) patients on clinical examination and 12 out of 40 (30 %) patients in MRI defecography which was similar to Rentsch, et al. [14] 6/20 (30%). Contrary to these findings, Ramage, et al. [16] found in a systematic review and meta-analysis of eight studies including 315 patients that no significant difference in detection rates of cystocele between dynamic MRI defecography and clinical examination with MRI defecography detecting cystoceles in 62.22% of patients and clinical examination detecting in 61.59%. This difference could be attributed to the larger sample size and more diverse inclusion criteria pooled by the meta-analysis.
Uterine prolapse was detected in MRI defecography in 14 out of 33 (60.90%) patients and 3 out of 33(9.1%) on clinical examination. Contrary to the findings from this study, Elshazly, et al. [11] detected uterine prolapse only in 2 out of 40 (6.45%) of patients via MRI defecography and did not detect it clinically in any patient. Ramage, et al. [16] found in a systematic review and meta- analysis of six studies including 263 patients that no statistically significant difference in detection rates of middle compartment descent between dynamic MRI defecography and clinical examination with MRI defecography detecting middle compartment descent in 49.43 % of patients and clinical examination detecting in 44.87 %.
The prevalence of enteroceles in patients with pelvic floor disorders was between17% and 37% with women being more frequently affected [17, 18]. The clinical symptoms are non-specific, and the physical examination is insufficient for an accurate assessment of enteroceles. Hence enteroceles are often missed at clinical examination [19].In the current study enterocele was found in 4 out of 33 (12.10%) patients via dynamic MRI defecography and was not detected clinically in any patient. These findings are consistent with previous studies; Elshazly, et al. [11] detected enteroceles in 6 out of 40 (15 %) patients. Rentsch, et al. [14] detected enteroceles in 4 out of 20 (20%) patients. Also, Ramage, et al. [16] found a systematic review and meta-analysis of eight studies including 323patients that the detection rate of enteroceles overall was 37.16% using dynamic MRI defecography versus 25.08% with clinical examination. JV RV, et al. [20] detected enterocele in 4 out of 30 (13.3%) patients and Paetzel, et al. [21] detected enteroceles in 2 out of 15 (13.33%) and documented that MRI defectography was superior to clinical investigation in the detection of enteroceles.
The Ano-rectal junction (ARJ) is the landmark of the posterior compartment [22]. In the current study perineal descent was detected in 12 out of 33(36.4%) patients while was observed in MRI defecography in 31 out of 33 (93.90%) patients. Similar to results of Elshazly, et al. [11] who detected perineal descent in 17 out of 40 (42.5%) of patients clinically and 29 out of 40 (72.50%) in MRI defecography. Rentsch, et al. [14] detected in12 out of 20 (60%) while Paetzel, et al. [21] detected in 5 out of 15 (33.33%). Intussusception, also termed internal rectal prolapse, had a frequency of between 12% and 27 % in patients with pelvic floor disorders. In the current study Intussusception was found in 15 out of 33 (45.45%) of patients with dynamic MRI defecography which was the same as clinical diagnosis 15 out of 33(45.44 %) of patients. Ramage, et al. [16] who found in a systematic review and meta-analysis of five studies including 162 patients that no statistically significant difference in detection rates of intussusception between dynamic MRI defecography and clinical examination with MRI defecography detecting intussusception in 27.78% of patients and clinical examination detecting in 22.84 %, which is consistent with our findings. Elshazly, et al. [11] who recorded intussusception in 10 out of 40 (25%) patients based on clinical diagnosis and this value was raised to 18 (45%) when dynamic MRI defecography was used. Rentsch, et al. [14] detected intussusceptions in 8 out of 20 (40%) patients. Similarly, JV RV, et al. [20] detected intussusceptions in 8 out of 30(26.70%) patients with MRI defecography with none being detected clinically.
In the current study, dynamic MRI defecography could detect more rectoceles and non-relaxing puborectalis when compared to clinical diagnosis, however the results were statistically insignificant (Table 9). Most of the rectoceles are diagnosed during physical examination but a reliable classification regarding size, emptying, and associated abnormalities are only provided by imaging with dynamic MRI defecography allowing for an accurate assessment of the location, size and degree of emptying of a rectocele.11 In the current study rectoceles were found in 21 out of 33 (63.60%) patients with dynamic MRI defecography and were detected clinically in 19 out of 33 (57.60%) patients. Elshazly, et al. [11] who detected a higher rate of rectocele, 32 out of 40 (80 %) patients, with MRI defecography and a similar rate to this study with clinical examination, in 24 out of 40 (60%) patients. JV RV, et al [20] detected rectoceles in 26 out of 30 (86.6%) of patients with MRI defecography and in 21 out of 30 (70%) of patients with clinical examination. Ramage, et al. [16] found in a systematic review and meta-analysis of nine studies including 439 patients that detection of rectoceles was similar across clinical examination and dynamic MRI defecography with a detection rate of 51.25% with MRI defecography versus 53.76% with clinical examination. Elshazly, et al. [11] detected non –relaxing puborectalis in 7/40 (17.5 %) of patients in MRI defecography while found it in 5/40 (12.5%) of patients in the clinical diagnosis.
In the current study, obstructed defecation was found to involve multi anatomical compartments with 85.18% of patients with obstructed defecation had more than one compartment affected. This finding was in line with previous studies; Elshazly, et al. found that 90% of patients had more than one compartment affected and 60 % had three compartments affected. Pescatori, et al. found that all patients had at least two occult obstructed defecation related diseases [23]. Finally, Renzi, et al. stated that obstructed defecation is caused by multiple patterns of different abnormalities of the rectum and pelvic floor and any treatment in symptomatic patients should be tailored to treat multiple combinations of different abnormalities [24].
In the current study, surgical treatment was scheduled for 26 out of 33 patients. 23 (88.46%) were scheduled for trans-perineal approach and 3 patients (11.53%) were scheduled for trans-abdominal repair. However, additional findings detected by dynamic MRI defecography significantly changed the surgical decision from trans-perineal approach to combined trans abdominal and trans perineal repair in 7 patients and from trans abdominal repair to combined trans- abdominal and trans perineal repair in 3 patients (P-value 0.004). Moreover, dynamic MRI defecography changed the decision from surgery to biofeedback in 5 patients 19.23% when dyskinetic puborectalis was detected. This result ties well with previous studies wherein Elshazly, et al. [11] found that additional findings detected by dynamic MRI defecography changed the management from trans-perineal to trans-abdominal combined repair in 6 patients out of
25 patients who were scheduled for trans perineal repair. Furthermore, dynamic MRI changed decision from surgery to biofeedback in 2 patients where dyskinetic puborectalis was detected. Attenberger UI, et al. [25] found that MRI findings led to a change of management in 13 out of 22 (59%) of patients. In 3 patients, conservative treatment was chosen instead of surgical management [26, 27] 4 cases were managed surgically rather than conservatively based on MRI findings, and in 6 patients the surgical procedure was altered based on the MRI findings. In the current study there was a significant difference with dynamic MRI defecography over the clinical diagnosis of cystocele (Anterior compartment), uterine prolapse, enterocele (middle compartment) and perineal descent (posterior compartment).
It is important to note that comparative studies had similar design, subjects, methods and limitations. The latter being the most influential in producing a definitive conclusion on its basis. MRI defectography does play an essential role in patients with PFD, however individual studies that are comparable to the current one should be read with caution as the level of diversity intrinsically varies widely resulting in many study limitations and variations. Rather, we encouraged that these studies be compiled in a systems review and meta-analysis or read in conjunction, to conduct a stronger conclusion. Future studies should include a larger sample size with stratification of data based on gender and type of dysfunction, as well as have a wide range of inclusion criteria for PFD.
Limitations
We acknowledge several notable limitations in this study. Naturally, a small sample size (n=33), mixed cohort of males and females may harbor heterogeneity of results due to lack of generalization and thus compromising external validity. Further, a conclusion on the efficacy of treatment (post- modification) on the basis of treatment success, recurrence rate, specificity and prognosis is lacking due to absence of post-operative follow up. These limitations prevent us from drawing a definitive conclusion. Finally, it is important to note that the size of the study group in comparative studies was not significantly different.
Conclusion
Dynamic magnetic resonance imaging represents a convenient diagnostic procedure in females, and to a much lesser extent in males, in the assessment of pelvic floor muscles and organs and detection of any concomitant masked pathology that may be unmasked later after surgery. Thus, dynamic MRI defecography in addition to the clinical assessment plays an important role in guiding interdisciplinary treatment decisions in patients with pelvic floor dysfunction to tailor treatment in order to avoid failure and recurrence.
References
-
Macura KJ, Genadry RR, Bluemke DA (2006) MR imaging of the female urethra and supporting ligaments in assessment of urinary incontinence: spectrum of abnormalities. Radiographics 26(4): 1135-1149.
-
El-Sayed RF, Morsy MM, el-Mashed SM, Abdel-Azim MS (2007) Anatomy of the urethral supporting ligaments defined by dissection, histology, and MRI of female cadavers and MRI of healthy nulliparous women. AJR Am J Roentgenol 189(5): 1145-1157.
-
Durnea CM, Khashan AS, Kenny LC, Durnea UA, Dornan JC, et al. (2017) What is to blame for postnatal pelvic floor dysfunction in primiparous women-Pre-pregnancy or intrapartum risk factors? Eur J Obstet Gynecol Reprod Biol 214: 36-43.
-
Nygaard I, Barber MD, Burgio KL, Kenton K, Meikle S, et al. (2008) Pelvic Floor Disorders Network. Prevalence of symptomatic pelvic floor disorders in US women. Jama 300(11): 1311-1316.
-
Maglinte DD, Kelvin FM, Fitzgerald K, Hale DS, Benson JT (1999) Association of compartment defects in pelvic floor dysfunction. AJR Am J Roentgenol 172(2): 439-444.
-
Dann EW (2008) Magnetic resonance defecography: an evaluation of obstructed defecation and pelvic floor weakness. Semin Ultrasound CT MRI 29(6): 414-419.
-
Zonca G, De Thomatis A, Marchesini R, Sala S, Bozzini B, et al. (1997) Dose assorbita dalle gonadi dei pazienti adulti sottoposti a studio defecografico con acquisizione radiografica digitale o tradizionale [The absorbed dose to the gonads in adult patients undergoing defecographic study by digital or traditional radiographic imaging]. Radiol Med 94(5): 520-523.
-
Seynaeve R, Billiet I, Vossaert P, Verleyen P, Steegmans A (2006) MR imaging of the pelvic floor. JBR-BTR. 89(4): 182-189.
-
El Sayed RF (2020) Magnetic Resonance Imaging of the Female Pelvic Floor: Anatomy Overview, Indications, and Imaging Protocols. Radiol Clin North Am 58(2): 291-303.
-
El Sayed RF (2020) Integrated MR Analytical Approach and Reporting of Pelvic Floor Dysfunction: Current Implications and New Horizons. Radiol Clin North Am 58(2): 305-327.
-
Elshazly WG, El Nekady Ael A, Hassan H (2010) Role of dynamic magnetic resonance imaging in management of obstructed defecation case series. Int J Surg 8(4): 274- 282.
-
El Sayed RF, Alt CD, Maccioni F, Meissnitzer M, Masselli G, et al. (2017) ESUR and ESGAR Pelvic Floor Working Group. Magnetic resonance imaging of pelvic floor dysfunction - joint recommendations of the ESUR and ESGAR Pelvic Floor Working Group. Eur Radiol 27(5): 2067-2085.
-
Kamal EM, Rahman FM (2013) Role of MR imaging in surgical planning and prediction of successful surgical repair of pelvic organ prolapse. Middle East Fertility Society Journal 18(3): 196-201.
-
Ren Rentsch M, Paetzel C, Lenhart M, Feuerbach S, Jauch KW, et al. (2001) Dynamic magnetic resonance imaging defecography: a diagnostic alternative in the assessment of pelvic floor disorders in proctology. Dis Colon Rectum 44(7): 999-1007.
-
El Sayed RF, Fielding JR, El Mashed S, Morsy MM, El Azim MS (2005) Preoperative and postoperative magnetic resonance imaging of female pelvic floor dysfunction: correlation with clinical findings. Journal Of Womens Imaging (4):163 7(4): 163-180.
-
Ramage L, Simillis C, Yen C, Lutterodt C, Qiu S, et al. (2017) Magnetic resonance defecography versus clinical examination and fluoroscopy: a systematic review and meta-analysis. Tech Coloproctol 21(12): 915-927.
-
Fenner DE (1996) Diagnosis and assessment of sigmoidoceles. Am J Obstet Gynecol 175(6): 1438-1441.
-
Jorge JM, Yang YK, Wexner SD (1994) Incidence and clinical significance of sigmoidoceles as determined by a new classification system. Dis Colon Rectum 37(11): 1112-1117.
-
Hauck, R. (1993). Rectal Outpocketing. In: Buchmann, P., Brühlmann, W. (eds) Investigation of Anorectal Functional Disorders. Springer, Berlin, Heidelberg.
-
Martín Martín G, García Armengol J, Roig Vila JV, García Coret MJ, Martínez Sanjuán V, et al. (2012) M. Análisis de nuestra experiencia mediante el uso de resonancia magnética dinámica pelviana en la evaluación del síndrome de defecación obstructiva [Analysis of experience in the use of dynamic pelvic magnetic resonance imaging in the assessment of obstructive defaecation syndrome. Cir Esp 90(5): 292-297.
-
Paetzel C, Strotzer M, Fürst A, Rentsch M, Lenhart M, et al. (2001) Dynamische MR-Defäkographie zur Diagnostik kombinierter Beckenbodenfunktionsstörungen in der Proktologie [Dynamic MR defecography for diagnosis of combined functional disorders of the pelvic floor in proctology]. Rofo 173(5): 410-415.
-
Locke GR 3rd, Pemberton JH, Phillips SF (2000) AGA technical review on constipation. American Gastroenterological Association. Gastroenterology 119(6): 1766-1778.
-
Pescatori M, Spyrou M, Pulvirenti d’Urso A. (2006) A prospective evaluation of occult disorders in obstructed defecation using the ‘iceberg diagram’. Colorectal Dis 8(9): 785-789.
-
Renzi A, Izzo D, Di Sarno G, De Iuri A, Bucci L, et al. (2006) Cinedefecographic findings in patients with obstructed defecation sindrome. A study in 420 cases. Minerva Chir 61(6): 493-499.
-
Attenberger UI, Morelli JN, Budjan J, Herold A, Kienle P, et al. (2015) The value of dynamic magnetic resonance imaging in interdisciplinary treatment of pelvic floor dysfunction. Abdom Imaging 40(7): 2242-2247.
-
Agachan F, Chen T, Pfeifer J, Reissman P, Wexner SD (1996) A constipation scoring system to simplify evaluation and management of constipated patients. Dis Colon Rectum 39(6): 681-685.
-
Andrew PZ, Steven DW (2010) Coloproctology, Springer Science & Business Media (Springers Special Surgery Series).
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era