A Prototypical Shift Back to the Original Role of Surgery for Endometriosis in Specialized Centres in Experienced Hands
In the last couple of decades with the modernization of newer instrumentation as well as surgical procedures there has been a rekindled interest in a field of Reproductive Surgery to which obituary had been paid with the advent of assisted reproductive technology (ART) as well as invitro fertilization (IVF). During that time period we were sceptical of Surgery for endometriosis due to surgery performed by incompetent surgeons leading to depletion of ovarian reserve with lowered markers of ovarian reserve for instance- anti mullerian hormone (AMH) as well as antral follicles counts(AFC).Nevertheless worldwide thre is switch towards greater training of reproductive endocrinology &Infertility specialists(REI) personnel in minimally invasive surgical strategies of endometriosis along with need for them to train the coming generations of REI so that with surgery performed by reproductive surgeons shaving expertise in addition to experience the chance of recurrent surgery dwindles & might even avoid need for ART in those desiring fertility. Even if future fertility is not the question REI’s experienced with needling procedures can perform sclerosing therapies which even aid in conception in those who might not have accessibility to a specialized endometriosis centre.
Introduction
Endometriosis portrays a chronic disease which significantly impacts the psychosocial good feeling, quality of life (QOL), decreased capacity of productivity in addition to cost incurred. It impacts 6-10% of reproductive aged women in addition to30-50% of women whose presentation is with infertility [1]. To their misfortune women having endometriosis encounter significant postponement of receipt of appropriate treatment. Canonically dependent on the treatment strategies based on the history of prior treatment strategies ,it has been acknowledged that surgery is the requirement with the documented rates of recurrent operations are substantially greater as much as 51% [2]. Probably this thought origination takes place in view of the utilization of medieval devices with the aim of diagnosis along with procedures using ablation, finally the diseased tissue remains back on key structures which ends in considerable fibrosis. Recurrent operations along with surgeries where extirpation done without any need might result in infertility, leaving a patient who is agonized. Recently Roman H, et al. [3], documented their observations from a substantially long term prospective database from a single centre which had been specialized with regards to endometriosis with the study portraying one of the biggest series having a long term follow up of patients having endometriosis in the literatue. They followed up greater than 1000 patients having endometriosis who had surgery performed by a single reproductive surgeon possessing expertise for performing as well as those who were having total endometriosis excision got followed up prospectively for greater than 10yrs for isolation of rates of recurrent surgeries in addition to situations which resulted in the requirement for recurrent Surgery.
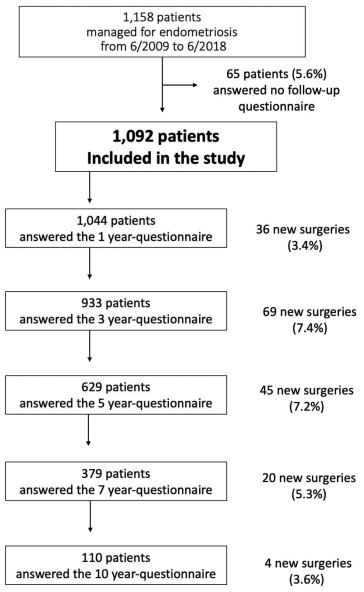
Figure 1: Kaplan-Meier curves presenting the probability of being free of repeated surgery for endometriosis during postoperative follow-up (mo). Numbers on the curve represent women free of repeated surgery who completed follow-up during the time interval (right-censored data).
Patients not having previous endometriosis had an extensive assessment preoperative, basically with utilization of magnetic resonance imaging (MRI) for accumulation of detailed knowledge with regards to placement along with stage of the disease. Subsequent to surgery classification was carried out with the utilization of American Society of Reproductive Medicine (ASRM) as well as ENZIAN classification systems. The risk of need for recurrent surgeries at1,3,5 as well as7 yrs was 3%,11% ,18%,23%, as well as 28% respectively see (Figure 1).
Study Flow Chart
Emphasizing the following these indicators with regards to this study were
- Surgery performed by a single reproductive surgeon possessing expertise for performing endometriosis surgery in a single centre substantially specialized with regards to surgeries for endometriosis having the objective of total excision of the macroscopic disease
- maximum patients possessed deep endometriosis(83%) of which 63% had infiltration in the bowel along with there was intactness of influence with regards to recall bias regarding illustration of postoperative hormonal repression in this long period .All these 3 factors might have aided in the generation of bias in this particular study. Clarification is there with regards to outcomes of this study from a single centre with specialization mainly for endometriosis resulting in complicated deep infiltrating endometriosis might restrict the significance of these external observations.
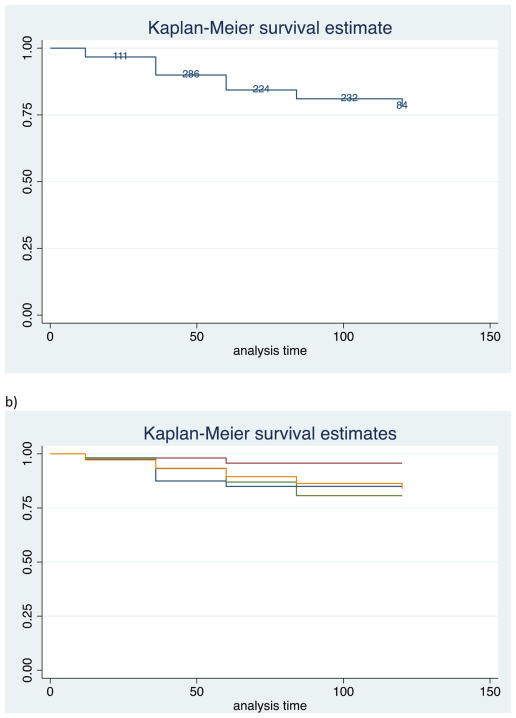
Figure 2: Kaplan-Meier curves presenting the probability of being free of repeated surgery in women managed for superficial endometriosis (blue line), endometriomas (red line), deep endometriosis sparing the bowel (green line), and deep endometriosis infiltrating the bowel (orange line).
Surgical treatment of endometriosis is complicated in view of variation of phenotypes; hurdles in pre-operative planning in addition to have to take into account what the patients preference is with regards to pain abrogation as well as chance of conception. Moreover, surgery for deep endometriosis might be full of hurdles in addition to usually implicate having a strategy of interdisciplinary team. Greater volume, specialized referral centres are best suited for guaranteeing both competence in addition to experience in the endometriosis treatment. Nevertheless, what is the requirement for these centres? These centres possess the properties of apart from greater surgical volume, having greater quality of care as well which gets ensured by the monitoring results. In addition to provision of state of the art clinical managing with regards to patients with endometriosis, the team of such centres need to delve in research, in particular prospective studies like this one performed by Roman H, et al. [3]. In view of retrospective studies in endometriosis are correlated with considerable significant biases inclusive of recall bias, ii) utilization of various staging systems iii) absence of long term follow up. The objective of this study was provision of answering queries associated with recurrent surgeries once surgeries got performed in a centre substantially specialized with regards to surgeries for endometriosis which fulfilled all these recruitment properties (namely greater volume, greater quality of care as well as research facilities). Recurrence risk is part of the maximum consideration for the patients in addition to the reproductive surgeons. Nevertheless, quantities of recurrence is variable in the form of;
- recurrence of symptoms
- recurrence of endometriosis depending on non-invasive imaging
- surgical repitition without recurrence of endometriotic damaged areas
- recurrence of visible endometriosis without histological corroboration along with
- recurrence of endometriotic damaged areas with histological corroboration [4].
One more commonly ignored impact is facilitating expert- level care of endometriosis centred with regards to endometriosis yields opportunity to reproductive surgeons who are functional in those centres the advantages of managing the greater volume, that causes reduction of learning curve. Furthermore, they rapidly became efficient in complicated techniques resulting in advantageous results. Noticeably, a direct correlation exists amongst the expertise in addition to experience of the reproductive surgeons along with risk of recurrence of deep endometriosis [5]. Women having surgeries performed by reproductive surgeons having greater surgical experience possess lesser association with recurrence in addition to need for repeated surgeries [5].
However, time is ripe to accept that this belief has switched, furthermore there has been alteration in workforce with numerous surgeons possessing expertise trying to get training in minimally invasive surgical strategies of endometriosis management with the generation of training programs all over the world. At present the accessibility of excellent management, specifically in the patients needing surgical management is great corroboration for stimulation of an archetype switch regarding endometriosis being a situation having the feasibility of great results along with negligible repeated surgeries once managed by skilled personnel in appropriate setting by surgeons possessing expertise. Provision of a holistic strategy is of utmost significance, to recognize that pain recurrence need not be the stimulation initiator for a repeat surgery in addition to accept the fact that there are numerous factors responsible for pain along with patients having the diagnosis of endometriosis made require an interdisciplinary team strategy in centres which are specialized referral centres for endometriosis treatment [6].
Conclusion
Earlier we reviewed role of surgery in endometriosis in addition to were sceptical over role of surgery in endometriosis with regards to need for repeated surgeries in view of no tackling by reproductive surgeons/ surgeons possessing the expertise in addition to experience for performing these complex surgeries which resulted in adhesions generation as well as depletion of ovarian reserve leading to reduction in anti mullerian hormone (AMH) or antral follicles counts(AFC)-for instance markers for ovarian reserve [7, 8, 9, 10, 11]. Nevertheless, there has been switch recently with rekindled interest in role of reproductive surgeons with plateauing of IVF outcomes in addition to worldwide emphasis on training programs for reproductive surgeons regarding training in minimally invasive surgical strategies of endometriosis as well as concentration on generation of specialized referral centres dedicated to treating endometriosis might aid in getting pregnancy even naturally subsequent to surgery in endometriosis in those desiring future fertility. Thus there has been a standardized shift back to surgeries for endometriosis; however in hands of experienced surgeons or even particularly specialized referral centres dedicated to treating endometriosis which avoids recurrent surgeries as well as might even avoid need for ART in those desiring fertility [3, 11]. In those not desiring future fertility even sclerosing therapies might be enough to relieve pain in case of ovarian endometriomas [9].
References
-
Practice Committee of the American Society of Reproductive Medicine (2012) Endometriosis and infertility:a Committee opinion. Fertil Steril 98(3): 591- 598.
-
Cheong Y, Tay P, Luk K, Gan HC, Li TC, et al. (2008) Laparoscopic surgery for endometriosis: how often do we need to reoperate. J Obstet Gynaecol 28(1): 82-85.
-
Roman H, Chavanaz Lacheray I, Hennetier C, Tuech JJ, Dennis T, et al. (2023) Longterm risk of repeated surgeries in women managed for endometriosis: A 1092 patient series. Fertil Steril 120(4): 870-879.
-
Mueleman C, Tomassetti C, Wolthius A, Van Cleynenbreugel B, Laenen A, et al. (2014) Clinical outcome after excision of moderate-severe endometriosis with or without bowel resection and reanastamosis:a prospective cohort study. Ann Surg; 259(3): 522-531.
-
Carmona F, Martinez ZA, Gonzalez X, Gines A, Bunesch L, et al. (2009) Does the learning curve of conservative surgery in women with endometriosis impair the recurrence rates? Fertil Steril 92(3): 868-875.
-
Carugno J, Moawad N, Mikhail E (2023) Time for aparadigm shift. Fertil Steril 120(4): 815-816.
-
Kaur KK, Allahbadia GN, Singh M (2018) Current Role of Surgery in Endometriosis; Indications and Progress. Surg Med Open Acc J.
-
Kaur KK, Allahbadia GN, Singh M (2020) Dilemna regarding preference of surgery or medical treatment in case of tubal blockade, endometriosis or adenomyosis and pelvic adhesion prevention once surgery is contemplated-a systematic review. Gynaecology, Andrology and Reproductive Medicine.
-
Kaur KK, Allahbadia GN, Singh M (2020) Management of Inoperable Recurrent Endometrioma Presenting as Severe Incapacitating Pain Following Leuprolide Acetate Depot by Aspiration, Recurring Again a 2 Yrs Subsequently for Sclerosing Therapy at Present: A Case Report. SunText Rev Case Rep Image 1(1): 107.
-
Kaur KK, Allahbadia GN, Singh M (2019) Dissecting the Reduced Ovarian Reserve Seen with Ovarian Enometriomas with That Caused by Surgical Excision of Ovarian Enometriomas- What Comes First. Surg Med Open Acc J.
-
Kaur KK, Allahbadia GN, Singh M (2023) The role of Reproductive Surgeons/Surgery has got Rekindled With Plateauing of IVF Results &Advances in Technology-A Comprehensive Narrative review.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era