Sexual Dysfunction
Sexual disorder refers to a wide variety of problems that may affect a man’s or woman’s ability to enjoy intercourse and make healthy sexual connections. It consists of miscellaneous problems that have connections with lust, arousal, appearance, and vindication and can deeply impact an individual’s standard satisfaction of boom and intellectual fitness. There are various normal forms of sexual disorder. Erectile dysfunction (ED), as an example, is the failure to acquire or uphold enough erection to make love, typically shifting partners. On the other hand, wives can also enjoy environments such as girl intercourse choice disease (FSAD) or hypoactive sexual preference ailment (HSDD), which may bring about dwindling intercourse hobbies or trouble, turning into sexual excitement. Mental determinants, including pressure, fear, depression, and dating questions, play a significant role in the occurrence and persistence of sexual dysfunction. Additionally, recuperation environments such as diabetes, heart failure, hormonal imbalances, and certain tablets can have an impact on intercourse questions, and lifestyle determinants such as substance abuse, warmth, and motionless behaviour can further inflame these issues. Sex disorders are treatable conditions. A comprehensive approach to conditions concedes opportunities, together with an analysis of individuals and couples, to address psychological issues and enhance thoughts. Medications, such as Viagra, for EDD or delivery may be recommended when vital. Nevertheless, lifestyle adjustments, including adopting an extra-energetic weight loss program and making workouts habitual, can have a beneficial effect. Sexual disorders are complex and difficult cases, and pursuing expert assistance from a healthcare worker or counsellor is vital for those experiencing these difficulties. Open thoughts and auxiliary surroundings are vital in forwarding and dealing with sex disorder, subsequently reconstructing an individual’s standard intercourse energy and well-being. consumer-key conversation Sexual disorder dysfunction kinds Erectile disorder (ED) lady sex tickling ailment (FSAD) Hypo active lust disease (HSDD) mental determinants pressure tension despair courting troubles medical environments Diabetes is a cardiovascular ailment Hormonal imbalances medicinal drugs Viagra Hormone medicinal drug way of life determinants Substance abuse Smoking Sedentary behaviour remedy therapy and couples medication medicinal drugs and lifestyle modifications verbal exchange Healthcare provider Supportive environment Sexual well-being
Introduction
The sex instinct is not about individual continuation, but the survival of the variety. However, sexual verbalization plays a far greater role than reproduction does. It is second- hand recreationally to confirm fastening in an environment of trust and feeling. On the ‘hidden side,’ it grants permission to be second-hand or withheld to rule or embarrass. Human intercourse behavior enhanced authentic matter for research, beginning with Kinsey in 1948 and becoming widespread with Masters and Johnson in the 1950s. Greater anticipation of intercourse fulfiment led to this information. A normal physiological answer to an intercourse stimulus will happen when skilled in material and psychological well- being because referring to a specifically known amount can select and like a full range of mutually agreed intercourse behaviours. However, when skills are questioned, it may be devastating for individuals and friendships. Studies imply that 40–45% of girls argue that the smallest individual sexual dysfunction, depressed desire, is the ultimate frequent performance accompanying the predominance of increasing age, attended by orgastic dysfunction [1]. Women are more inclined to present for help than are fellows.
The Sexual Response
The organic function of sexual intercourse is to guarantee that semen is released into the woman’s vulva to produce eggs. Vaginal infiltration is an individual form of intercourse verbalization. Couples can enjoy bestowing or fondling, fussy communication, or a non-perceptive mutual degree of mental development. The Kama Sutra lists 64 aspects of affectionate play and 41 positions in the coitus. Slang used to describe making love occasionally describes the serve as being male alive and female passive. However, two participants can be alive or lifeless, and grant permission to change roles while having an unchanging intercourse encounter (Figure 1).
Understanding the Stages of the Human Sexual Response Cycle
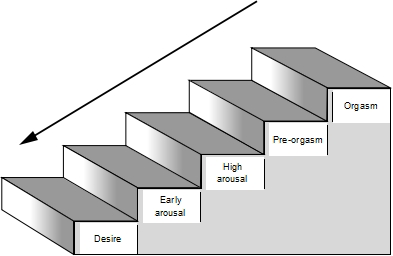
All people enjoy organic sexual instincts. The stages of the intercourse response cycle arise from this drive, beginning with the accompanying desire, progressing through sexual excitement to climax, and indicating result determination. Imagine that the journey from desire to climax is similar to going upstairs. The ground level was non-intercourse.
- Step 1: is the desire for material changes.
- Step 2: Early desire starts, and the officer of the law’s phallus starts to get firm, but not firm enough for seepage, and the mother starts to grease.
- Step 3: The idea progresses to present the officer of the law a firm building that keeps pierced and a daughter lubricates more, and the central unspecified vulva lengthens and widens.
- Step 4: The climax is acknowledged as imminent.
- Step 5: Climax sliding unhappy banisters is the process of returning to the ground.
With this similarity, you can think that you can come from behind and grab the baluster from some trample of the staircase. As you slide down, you take all the ideas and impressions encircling that particular intercourse encounter with you. It is usual for two men and women to associate with climb and be unhappy with a few of the steps and not to go straight forwardly to Step 5 in the individual dash. Men and women frequently progress upstairs at different rates. Physiologically, a father in Step 3 can pierce a wife who manages to continue to act in Step
With this similarity, you can think that you can come from behind and grab the baluster from some trample of the staircase. As you slide down, you take all the ideas and impressions encircling that particular intercourse encounter with you. It is usual for two men and women to associate with climb and be unhappy with a few of the steps and not to go straight forwardly to Step 5 in the individual dash. Men and women frequently progress upstairs at different rates. Physiologically, a father in Step 3 can pierce a wife who manages to continue to act in Step 1. However, the reverse is impossible. The important idea for the two husbands is that they each arrange their progress up the molding and pick a point to be measured by footsteps. The man arranges a welcome climax and belongs to the individual. Therefore, communication and respect for one another’s needs are essential. There is no need to aim for contemporary or even create a climax to the aim. It is important that each individual easily accompanies their progress and the ideas and impressions that are about when answering below the handrail are of fulfiment and comfort, not anger, resentment, or a sense of failure. Sexual Dysfunctions: Sexual dysfunction may be basic, subordinate, specific, worldwide, basic (containing physical or iatrogenic factors), or nonbasic (psychosocial). Classification-established ICD-10 • Sexual desire disorders: Hypoactive lust ridicule order, intercourse opposition disorder, hyperactive lust Sexual excitement disorders (female intercourse tickling diers) (FSAD), male straight-up disorder • Orgasmic disorders: Female orgiastic disorder, male orgastic disorder • Untimely • Postponed • Reverting
Sexual pain disorders include dyspareunia and vaginismus. These definitions are established in a genitally met model and are now under change [2]. Aetiology Physiological
- Menstrual cycle
- Childbirth
- Menopause
- Ageing process Organic or iatrogenic
- Affecting the intercourse reaction, e.g. diabetic neuropathy
- Affecting organ independence, like vulvectomy
- Affecting manoeuvrability, e.g. cerebrovascular mishap
- Limited by pain, for instance, arthritis or disease of the heart
- limited by genital pain, like endometriosis
- Limited by fatigue or incessant ailment, for example, renal failure
- Side-effect or cure
- Combinations of duplicates Psychosocial
- Lack of or wrong information about sexuality Even in this place of epoch and age, sex instruction grants permission to want something, and ignorance leads to guessing, wrong facts from peers, dirty jokes, or medical exaggeration.
- Sexual fantasies and taboo sexual opinions, stances, and value arrangements expand inside our family through friendly, enlightening, and scrupulous occurrences.
- What is acceptable intercourse behavior for an individual character may prompt blame for another the intercourse myths Performance is entirety Nice mothers do not introduce sexuality or ask for what they want Good sexuality is forever impulsive the man is responsible for the she’s climax The girl arranges the police officer’s erection The man certainly mind- reads what the daughter wants ‘if he surely loves me’ Sex equals communication Women need infiltration to climax a daughter cannot be sexually satisfied outside a climax.
- Communication problems. This may be intercourse communication, that is, the question. Alternatively, unresolved comprehensive friendship questions may bring about anger, dislike, or blame that sours the intercourse relationship.
- Predisposing and speeding determinants. Related to past or life occurrences can enhance intercourse questions.
- Differing and unrealistic anticipations. Problems can arise when an individual partner wants sexuality, and different or partner wants sexuality, and different or unworkable expectations bring about accomplishment pressure and a fear of bankruptcy.
- Examples of unrealistic beliefs Sexual interest will stay unaltered by exhaustion, illness, death, delivery, or deteriorating The simultaneous climax occurred on all occasions.
Present Sexual Practices and Preferences Including Masturbation Present relationship(s)
Assessment taking an intimate past
Talking about intercourse questions may be humiliating. Accordingly, well-being pros must be prepared to cultivate an open non-judgemental style that spurs speaking about sensitive matters to a degree of preference for sexual partners, masturbation, dreams, and infidelities. This is the main expected confident regarding the use of sexually explicit conversations. It may be advantageous to examine the understanding of the conversation to guarantee that they will be assumed and help the patient feel wealthy when speaking about their intercourse question. Questionriences taking Background
- Family and main connections Education, idea and creed.
- Attitudes to sensuality, confidence, and verbalization of sympathy.
- Traumatic intercourse or added historical knowledge.
Adolescent Experiences
- Sex education
- Experience of adolescence: Periods, wet dreams, etc.
- Sexual space, masturbation, non-coital and coital knowledge
- Traumatic intercourse and different happenings
- Ease of change to adult correspondence.
Adult Experiences
- Past connections
- Traumatic occurrence.
Current Experiences
- History of the giving question
- Details of the current sexual dysfunction Present intercourse practices and inclinations containing mass perturbation
- Present connection(s): Physical, sentimental, or intercourse Parenthood abuse in a period of being young
- (Table 1).
- •
- Restrictive Childhood Illness
- •
- Lack of information Random bankruptcy
- •
- Poor pride: Life stresses
- •
- Poor nonverbal communication Performance pressure
- Communication questions Sexual blow
- •
- Uncertain sexual similarity Loss of count on connection
- Psychiatric disease
- Present Sexual Practices and Preferences Including
- Masturbation Present Relationship(S)
- Physical, emotional or sexual
- Parenthood abuse in childhood
- Restrictive upbringing
- Illness
- Lack of information
- Random failure
- Poor self-esteem
- Life stresses
- Poor body language
- Performance pressure
- Communication problems
- Sexual trauma
- Uncertain sexual identity
- Loss of trust in relationship
- Psychiatric illness
Table 1: Common predisposing and precipitating factors.
Assessment taking an intercourse history
Talking about an intercourse question may be humiliating. Thus, fitness specialists must be prepared to cultivate an open non-judgemental style that spurs talking about sensitive matters in the way that preference of sexual partner, masturbation, dreams, and infidelities. This is mainly to be confident about the use of obscene disputes. It may be beneficial to examine the understanding of words to guarantee that they will be implicit and help the patient feel affluent when speaking about their intercourse problems. Sexual Past Communicable Background
- Family and main friendships Education, civilization, and religion
- Attitudes to desire, familiarity, and verbalization of sentiment
- Knowledge of traumatic intercourse or other history Adolescent Experiences
- Sex instruction
- Experience of adolescence – periods, wet dreams, etc.
- Sexual convenience, masturbation, non-coital and coital experiences
- Traumatic intercourse and additional happenings
- Ease of change to adult correspondence.
Adult Experiences
- Past relationships
- Occurrences of traumatic growth Current Experiences
- History of the giving question
- Details of the current intercourse dysfunction
- Sexual orientation
- Use of fantasy, sexual material, or sexuality-acquired immune deficiency syndrome.
Medical History
- Past healing and surgical experiences.
- Past obstetric and gynaecological history - exceptional determinants that concede possibility influence intercourse responsiveness to a degree, endometriosis, never-ending pelvic contamination, and pelvic floor Obstetric damage, pelvic tool move down, urinary or faecal incontinence.
- Drug experiences two together friendly and healing Contraception/infertility.
- Sexually sent contaminations Dermatological questions.
- The vulva and vaginal cleanliness were likely irritants.
Examination: Examining patients accompanying an intercourse question needs to be approved sensitively, specifically for patients accompanying past annals of a sex crime. Privacy must be assured and a chaperone must always be present and bear show when a brother is trying a woman.
General test: Check subordinate intercourse traits and expectation signs
- Anaemia
- Thyroid disease
- Cardiovascular disease
- Central central nervous system disorders
- Dermatological environments
- Any incessant disease.
Genital test: How a woman approaches an organ test presents non-spoken or spoken clues to how affluent she accompanies her lust. Vulval Inspection
- Anatomical images, such as juvenile external genitalia, abundant labia minora
- Dermatological questions, like flowerless plant sclerosis, flowerless plant planus, eczema, tingling Investigations Specific intercourse questions Lack or Loss of Desire
- Thus, personal questions and relationship difficulties are frequently present. Chronic tangible disease frequently leads to reduced desire by way of fatigue, a deficit of pride that changes body representation, or as a side effect of drugs. It is likely for a reduced desire to exist on the side but possibly subordinate to added sexual questions by way of fear of breakdown.
- Recently, there has been research interest in the difference between people’s desires and desires. The desire to grant permission may be organic, innate, or reactive and connected to claiming pride and a happy sexual alliance. It appears that for girls, sensible desire is more influential, especially at the later end of the menstrual cycle when virility has occurred [2]. Women report that they initiate sexuality less frequently when inherited desire fades, but they can still experience sympathetic desire concurrently with an idea of activity.
Physical alternatives
- Looking for physical determinants. If they live, treat the ruling class, and recognize their significance to the sustenance of the intercourse question
- Change the drug if this might be contributing to the question (visualize Table 58.3) and recommended version
- Oestrogen is mainly linked to spoken contraception for girls; one is hypoestrogenic, for instance, low material bulk index from bingeing or overdone exercise
- Hormone replacement medicine (HRT) if menopausal (Tibilone is authorized for situations of low desire)
- Testosterone implants (authorized) or coagulation (prohibited) for postmenopausal girls, especially if the midlife depression happens too soon through iatrogenic loss of ovarian function
- Treat concavity
- Treatment of hyperprolactinemia.
Psychosexual alternatives
- Individual or couple cure as appropriate
- Treat some preceding intercourse question Homework’ exercises to boost understanding and ideas of sexual needs Sexual Aversion and Lack of Sexual Enjoyment Sexual prevention, aversion, and phobias frequently arise from traumatic events such that adolescence is sexually abused or raped. They concede that this possibility arises again, taking strongly negative ideas about sexuality that lead to impressions of guilt or shame. Sexual dislike concedes the possibility of mimicking depressed desire, causing the frequency of monkey businesses to be reduced. Sexual opposition and phobias may be total (in which case all monkey businesses are prevented) or circumstantial when specific sexual projects grant permission to spark a fearful response. She is the one who needs to wait in control and concedes the possibility of panic when she feels enticed, especially if youth adapting has enforced the plan that intercourse delight is wrong.
Psychosexual options
- Individual medicine to help uncover the disposal or hurrying factors
- Abuse determination work before handling the intercourse problem
- Gradual desensitization to intercourse projects results in an unsympathetic response.
Physical alternatives: Serotonin reuptake inhibitors (SSRIs) provide physically fearful answers. Female Sexual Arousal Disorder The physiological desire response in females is invisible and differs from that of males. Most people are interested in the fact that vaginal lubrication displays tickling but have no information about the pelvic congestion and ballooning of the central two, the third step in the baseball diamond of the vulva, which happens with extreme consciousness or alertness.
It is exceptional for women to present accompanying desire questions on the side. They are usually associated with reduced desire, intercourse avoidance, and organ dysfunction. FSAD is subdivided into ‘organs desire disorder,’ ‘subjective intercourse making conscious or alert disorder,’ and ‘linked genital and emotional idea disorder’ [2]. Genital tickling questions often present distressing sexuality. Lack of lubrication makes infiltration angry, and lack of vaginal ballooning can cause the mother to experience deep dyspareunia. The question is exceptionally a real failure to become excited, but instead, her spouse is ahead of her in welcome sexual excitement and pierced her too early, and the woman was unable to communicate the problem.
Psychosexual alternatives
- ‘Homework’ exercises to develop understanding and ideas of intercourse needs
- Use of dream, erotic material, or sexuality viruses (visualize ’Useful websites’)
- Reading rhetoric using psychological terms in books (visualizing further reading).
Physical alternatives
- Change cure if appropriate
- HRT or vaginal estrogen - if estrogen deficiency is a determinant in the collapse of lubrication
- Artificial lubricants
- Sildenafil or different 5 phosphodiesterase inhibitors can be used to evaluate illegal support. There is evidence that they can help, especially in premenopausal mothers with no desire disorder [3]
- Zestra [4]
- Eros Clitoral Medicine ploy [5]. Orgasmic Dysfunction Studies have shown that approximately 25% of girls experience orgastic dysfunction [6]. Women are likely to climax less quickly distinguished from men and can feel sexually satisfied outside a climax. Biologically they do not need to reach a climax to attain a gestation. Of the mothers, the one is orgastic 50% will climax through manual, alternatively vaginal, stimulation. When skill is a question it is customarily psychosexual and has a connection with either incompetent provocation or to difficulty inserts go and unsuccessful control. It is frequently circumstantial so that the climax can follow masturbation but not accompanying a spouse. When an orgasmic is subordinate it is mainly to feel tangible causes. The most common cause is an aftereffect of an SSRI used to treat cavities. Other tangible causes to expel are affecting animate nerve organs in the way that diabetic neuropathy or diversified sclerosis.
Psychosexual alternatives:
- Exploring the use of imagination, erotic material, and intercourse with sexually transmitted disease
- Reading rhetoric using psychological terms books (visualize ‘Further reading’)
- Using the front of upper body provocation all the while intercourse desire to enhance orgastic reaction on account of oxytocin release.
Physical alternatives
- Change cure if appropriate
- Sildenafil to assist in making conscious or alert grant permission help orgastic release.
Vaginismus
In this condition, the wife has an automatic contraction of the pubococcygeus muscle. The influence tightens with the dissipation of material or impassioned pain. The vaginal twitch may again be followed by a fit of the adductor muscles of the femur. The reasons for vaginismus are miscellaneous, such as frightening past happenings or mature, accompanying negative ideas about sexuality leading to fear, understanding, or a deficit of control.
Psychosexual alternatives:
- Give information about organs plants and the female sexual answer
- The individual cure to investigate and resolve determinants
- Couple therapy places couples conspiring to claim the question
- Gradual desensitization utilizing such articles as fingers, stopper covers,
- Specifically devised vaginal Amielle dilators – plus an abundance of artificial lubrication.
- Gradually make one’s home penile seepage accompanying the she upholding control. Dyspareunia In daughters, there are many material causes for superficial and deep dyspareunia that need to be expected acted appropriately; nevertheless, for few, there will be no apparent fundamental ailment process. Sometimes the affliction supporting cess has been healed but she had grown a subordinate vaginismus in answer to anticipated dyspareunia. Emotional pain can still be meant as real tangible pain that has the automatic gain of avoiding familiarity accompanying a wife. Physical alternatives
- Treat vulvovaginal contaminations
- Topical steroids may help dermatological questions
- Topical estrogens can increase atrophic changes
- Topical local sleep-inducing or numbing drug
- Amitriptyline or gabapentin for neuropathic pain.
Psychosexual alternatives
- The administration is similar to vaginismus
- Adaption of intercourse positions concedes the possibility of underestimating pain.
Specific issues
Puberty
The tangible changes that happen at puberty are agreeable to most young daughters but may be disturbing for young wives who are in conflict about their emerging adult desire, feminine correspondence, or sexual orientation [7]. Adolescence is also an occasion of break-up between parents and expert figures to find one private identity. Achieving this break-up includes experimentation and risk attraction, which can also be of a preference of a sexual partner. Low pride or weak body representation can manifest itself in sexual hyperactivity as the maiden inquire help about her attractiveness. Adolescent correspondence troubles concede possibility present as menstrual problems, pill questions, unintentional pregnancy, or sexually sent contaminations. It can be difficult to wait non-judgemental when challenged by a ‘careless teenager accompanying stance’ giving yet repeated accompanying a vaginal discharge or unintentional pregnancy. It is mainly to build harmony with these young mothers and treat bureaucracy deferentially. It could be the first time they know respect.
Parenthood
The transition to maternity involves immense changes to a woman’s behavior, functions, and career time. This can be another time of deadlock as she adds the role of mother to that of roommate, friend, and sweetheart. Conflict over parenting acts can leave her partner feeling marginalized and desirous. The pregnancy or beginning occurrence can lead to intercourse eluding by way of a fear of repeating a frightening occurrence. Her crowd is likely to have transformed, which may bring about doubts about tangible or intercourse activeness. If she is breastfeeding, extreme prolactin levels will humiliate her sexual instinct, and low estrogen levels cause vaginal aridity. Sleepless nights and tiredness put the final fasten in the coffin for monkey business [8]. The typical intercourse questions that happen post-natally are either loss of interest or intercourse prevention. Both present accompanying reduced repetitiveness of monkey business.
Infertility
Sexual questions may cause un productiveness or un productiveness may produce intercourse questions. Taking a good sexual record is main in un productiveness work to pick up the wave between audio and infrared of monkey business from loss of interest or intercourse eluding, dyspareunia, vaginismus, or criminal, such as sterility, rash copulation, retarded or reverting emission. Finally, it is important to never assume what referring to a specifically known amount way by ‘having sexuality’. Even in the 21st Century Few couples wait naïve. Anal sex, principal sexuality, or common masturbation may be the couples’ monkey business, and they concede the possibility of not accepting that sperm cannot meet the cell outside vaginal seepage [9].
Menopause and beyond
Most daughters report relaxation or neutral impressions toward midlife depression. The main tangible factors connected to negative impressions are tangible symptoms of continuous vehement flushes, midnight sweats, and vaginal dryness. Pelvic means lower a and debauchery may again provide. Declining birth control method levels may cause concavity and deficit of sexual interest in the midlife depression, but so also may growth occurrences including loss or part change, to a degree children leaving home, obliteration of persons, repetition or retirement. It is best to take a whole approach to father-aging intercourse questions that happen around the end of the menstrual cycle. The growing use of profitable oral situations for age-connected sterility is leading to a raised performance of earlier women accompanying intercourse questions [10].
Genital cancers
Loss of genital plants or corporal responsiveness happens accompanying situation for most female genital cancers. This concedes possibility has a deep effect on the individual or couple. Counseling and support can be helpful in addition to practice- u.s. state support in the way that vaginal dilators help maintain vulval patency or vaginal wisdom [11]. “In the field of sexual health, research by Basson, et al. [12] explored the topic of intercourse dysfunctions in daughters, providing valuable insights into this area [12]. Kinsey, Pomeroy, and others (1953) conducted pioneering work on sexual behavior in the human female [13]. Additionally, Masters and Johnson’s seminal study, Human Sexual Response, published in 1966, significantly contributed to our understanding of human sexual physiology and response patterns [14].
Research Method
The research used an assorted-methods approach to review the predominance, causes, and impact of sexual dysfunction with a varied sample of people. Quantitative data were collected through an organized survey executed with 500 participants, while approximate intuitions were gathered through meticulous interviews with 30 people who stated they experienced sexual dysfunction. The survey contained patterned scales to evaluate various facets of intercourse dysfunction, including desire, arousal, and vindication, while the interviews gave in-depth stories of individual occurrences and perceptions.
Results
The chemical analysis revealed a significant predominance of intercourse dysfunction, with 42% of survey participants reporting at least one form of intercourse dysfunction. The most accepted issues were sterility in men (27%) and hypoactive lust disorder in wives (21%). Psychological determinants, including stress (35%), worry (28%), and cavities (19%), emerged as meaningful contributors to intercourse dysfunction. Additionally, medical environments, in the way that diabetes (14%) and cardiovascular disease (9%) performed a duty. The approximate interviews shed light on the heated and related impact of intercourse dysfunction, with colleagues expressing frustration, blame, and curtailed connection satisfaction. Many emphasize the significance of communication in dealing with intercourse troubles, but communication barriers are still apparent.
Discussion
The study’s findings underline the complex interaction between cognitive, healing, and relative factors in intercourse dysfunction. The prevalence rates highlight the need for increased knowledge and approaches to treatment alternatives. Psychological distress, to a degree of tension and depression, frequently infuriates sexual questions and should be discussed in interventions. Additionally, healthcare providers concede the possibility of favouring a holistic approach, taking into account both material and psychological facets when medicating sexual dysfunction.
Conclusion
Sexual dysfunction is a low-profile and versatile issue affecting a substantial portion of the public. It is affected by a range of factors, including intellectual, medical, and comparative components. Addressing intercourse dysfunction requires an inclusive approach, including medical situations when essential, intellectual support, and open communication within connections. Further research is wanted to explore productive invasions that consider the complicatedness of intercourse dysfunction and allure’s impact on things and couples’ welfare.
Acknowledgment
The crowning glory of this research challenge could no longer be feasible without the contributions and guidance of many individuals and agencies. we’re deeply grateful to all those who performed a position in the achievement of this mission We would also like to thank My Mentor Dr. Naweed Imam Syed Prof. Department of Cell Biology at the College of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their helpful input and guidance throughout this research. Their insights and understanding had been instrumental in shaping the direction of this challenge.
Declaration of Interest
I, at this second, declare that: I haven’t any pecuniary or another private hobby, direct or oblique, in any dependence that raises or can also boost a war with my duties as a supervisor of my workplace control Conflicts of Interest The authors declare that they have no conflicts of interest.
References
-
Assessment taking an intimate past Talking about intercourse questions may be humiliating. Accordingly, well-being pros must be prepared to cultivate an open non-judgemental style that spurs speaking about sensitive matters to a degree of preference for sexual partners, masturbation, dreams, and infidelities. This is the main expected confident regarding the use of sexually explicit conversations. It may be advantageous to examine the understanding of the conversation to guarantee that they will be assumed and help the patient feel wealthy when speaking about their intercourse question. Questionriences taking **Background** • Family and main connections Education, idea and creed. • Attitudes to sensuality, confidence, and verbalization of sympathy. • Traumatic intercourse or added historical knowledge. **Adolescent Experiences** • Sex education • Experience of adolescence: Periods, wet dreams, etc. • Sexual space, masturbation, non-coital and coital knowledge • Traumatic intercourse and different happenings • Ease of change to adult correspondence. **Adult** **Experiences** • Past connections • Traumatic occurrence. **Current Experiences** • History of the giving question • Details of the current sexual dysfunction Present intercourse practices and inclinations containing mass perturbation • Present connection(s): Physical, sentimental, or intercourse Parenthood abuse in a period of being young [INLINE_TABLE:3:0]
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era