How Sex Works (and When it’s in Working)
Sexuality is a fundamental aspect of human life, including a range of physical, impassioned, and intellectual aspects. This abstract explores the elaborate mechanical details of how sex affects everything, removing the complexities that delimit human desire. Key elements include desire, ideas, and intercourse answers, all influenced by a myriad of organic, mental, and public factors. This item tests the key processes complicated in sexual functioning in the way that hormones, intellect, and reproductive organs interact. Intercourse dysfunction is a widespread issue that can improve the functioning of these processes. Common sexual dysfunctions, including sterility, rash ejaculation, and depressed sexuality have been discussed in depth. Furthermore, we investigate the intellectual facets of sexual troubles such that depiction anxiety, corpse figure concerns, and past blows can considerably impact an individual’s intercourse experience. The abstract still highlights the significance of communication and consent in athletic intercourse friendships, emphasizing that intercourse welfare is not determined only by tangible determinants. Key determinants for maintaining a fulfilling and effective sexual life were investigated, including open ideas, emotional relationships, and shared respect. In conclusion, this abstract offers observations of the multifaceted character of human lust, exemplifying how it works, and when it is in optimal disrepair. Understanding the miscellaneous factors that influence intercourse functioning and discussing average sexual dysfunctions, things, and couples can help navigate the complicated nature of their sexual lives, promoting more athletic and fulfilling relationships
Introduction
Sex is one of the main facets of the human condition and one of the most important factors in our development as a class. It is a necessary item of midwifery because apart from new medically assisted duplication methods; there will be no pregnancies without sexuality. Various disclosures have clarified that midwives need expertise two combined abilities, and knowledge of human sexuality. This member will widely devote effort to something using what sex everything and when sexuality is in disrepair, two together on an individual and couple level. Other chapters of this book will tackle desire and intercourse fitness from a more probable, psychological, or friendly view concerning different parts of the intervening wife’s field of practice, from bias to the young period of being pregnant with a child. What makes sexuality work? Can we define limits for advancing fulfilling sexual knowledge or understanding using what intercourse happens can be unsatisfactory or disappointing, for example, when sexuality does not work? This stage strives to surpass the absolute writing of models of sexual answer [1] and aims to outline a natural to use the ‘3-Conditions Framework,’ and describe insult the inevitable conditions that intercourse knowledge should meet expected ‘good.’ ‘Good’ means acceptable, fulfilling, sticking, fun, or anything one wants it expects.
The 3-Conditions Framework for satisfying sexual experiences
We propose a simple framework for how sex works, outlining three more or less essential requirements for a satisfying sexual experience:
- a sufficiently intact and functioning sexual system,
- ‘good enough’ sexual stimuli, and
- A comfortable context. When one fully understands these three conditions, it enables the HCP to translate them into diverse sexual practices. They can then serve as a framework for exploring clients’ sexual problems in counseling (e.g. by actively exploring these three conditions), as a mini-diagnostically tool (e.g. helping to understand which condition(s) that are likely to cause or maintain sexual problems) and as a framework for promoting sexual well-being (e.g., as a psycho-education tool).This study will first explain the ‘3-condition framework’ and then successively address its use as a counseling, diagnostic, and psycho-educational tool.
What Makes for Good Sex?: What does one need for good sex? What is the best way to stimulate women and men? Sexually? What is required for sexual satisfaction? If one tries to answer these questions factually, the result would likely be a useless list of sexual practices that might work for a given woman, partner, or couple. If we were to ask 100 people what they would need to have a good sexual experience, we would wind up 100 personal sexual guidebooks. At best, one can read someone else’s guide as a source of inspiration. At the margin of this chapter, this might be a personally enlightening exercise for each HCP in a committed relationship. The question then becomes: what are the conditions for people to have pleasurable sexual experiences? We recommend approaching this on a meta-level to understand what is required to satisfy any sexual experience. The three most relevant conditions are the sexual system, stimuli, and context.
An Intact and Functioning Sexual System: Sex requires the activity of multiple brain regions. The hippocampus, hypothalamus, and amygdala play a central role in routing and rerouting signals related to sexuality [2]. These signals travel through nerve bundles, connecting the brain with relevant erogenous zones (genitals, breasts, nipples, mouth, skin, neck, ears, feet, etc) [3]. If one of the links in this chain of information-sharing is malfunctioning, the entire system can become stressed, sometimes even making certain aspects of sexual experiences impossible. A person’s nervous system, endocrine system, genitalia, and sensory organs (skin, hands, lips, tongue, etc.) must be intact and functioning at least until a certain level. In other words: individual needs are expected to be capable of registering internal and extrinsic intercourse provocation (fantasies or desires, observing a delightful brother or woman, impression dignitary effortlessly brush your narrow connector, etc.) and all within schemes and tools that play a part in the obtained intercourse answer needs to function sufficiently. One can directly imagine that some pathology or healing attack can impact the sane functioning of the nervous system, endocrine system, or the senses can influence what we know about sexuality. The model of the negative effect of extreme prolactin and reduced testosterone levels during breastfeeding can affect lust and intercourse reusability. The negative impact of genito-pelvic pain induced by endometriosis can affect intercourse knowledge. However, it is important to note that the material method does not need to be in perfect condition to authorize people to have pleasurable sexuality. Many nations continue to enjoy sexuality despite, for example, antidepressants, agony from organ pathology, bearing a chronic affliction, being blind, sharing a wheelchair by way of spinal cord injury, etc. One’s intercourse plan does not have to be 100%, but it has to function sufficiently. To allow people to experience what they are going to experience.
Good Sexual Stimuli: Each method has its start-up requirements. Our intercourse plans did not differ. It requires the input of the intercourse provocation to start and continue. These stimuli may within (like thoughts or imagination) and outside (like sound, touch, scents, or just observing dignitaries, you find it attractive, new, or mature. Both can do the job evenly well. Most families have a common plan of which provocations are most valuable for themselves [4]. For most crowd in a constant relationship, the wife is the main beginning of various intercourse provocations. Partners can induce sexy thoughts or imagination and look Sensual when decorated in the right way (a suggestion of correction by any means) or be the individual who lights those agreeable, fragrant candles. Stimulation was possible. However, even when exposed to a conceivably Good provocation, you should still experience it as an intercourse habit. One’s mind has to present sexual aims and sexually legitimize provocation. In other words, it allows us to define it sexually. Whether this will happen largely depends on the individual’s private qualifications. And frame of reference for passion. So when the nation thinks about sexuality, their plans, and beginnings about sex—what is inviting, what is fun—will broadly decide whether potential sexual provocation will efficiently enhance sexual provocation for that customer. Thus, the better you experience your own and your sexual frame of reference (otherwise known as a love map), the smoother it will search out and find the proper provocation to jump-start your intercourse plan or that of your partner. The bottom line is that we need provocation to get our intercourse plan going, but we have to use bureaucracy as intercourse provocation to have the desired effect.
A Comfortable Context: Even after fulfilling the first two environments, individuals still need decent context for the position to cultivate the requested intercourse habits. When family members feel their physical intercourse structure is activated, their desire and Sexual excitement is constructed; opportunities and places must suit that life to happen. Entities that accompany these impressions. And repeated, independent of either period or place is a phenomenon of sexuality; it must feel the right. Both the material circumstances, your surroundings, and the individual’s circumstances, namely the individual’s psychology, need to be good enough to allow our intellect to visualize provocation as intercourse. When your mind is abroad, busy with non- intercourse ideas, or when your premature (negative) occurrences or assumptions come after the mix, even a conceivably exciting environment to give in to your desire may be converted into ‘uncomfortable’ to originate from a fulfilling intercourse happening.
The ‘3-Conditions Framework’ as a Communication Tool: For many midwives and other HCPs, passion is not an easy topic to address. Midwives have the power to feel private hurdles and remember it is unfit to request actively about intercourse well-being or fear, infesting the couple’s confidence. Still, research shows that wives and men wish the HCP to start a dialogue about intercourse well- being, as they excessively feel the challenge of sending such a taboo-loaded-down affair [5]. Chapter 26 will offer the obstetrician/HCP a gradual plan, the ‘individual-to- individual method’, for offset a dialogue accompanying the girl (or couple) on desire-connected topics. The second becomes involved in the model: ‘Let her speak her fiction.’ The mother can model, and become involved in discussing sexuality by querying about her current position’s organic, subjective, and friendly facets of exploring her plans, concerns, and anticipation of a connection with her intercourse growth. Here, too, we can use the ‘3-condition framework to allow the customer to clarify her current position completely. By energetically asking the customer about her tangible strength concerning passion and the attendance of sexual stimuli, and by investigating their experience framework, the customer and her ally start to paint a more extensive picture of their intercourse history sooner than expected.
The ‘3-Conditions Framework’ as a Diagnostic Tool in Case of Sexual Problems: The obstetrician does not continually have the skills and information to determine the intercourse questions for the customer. However, this is not inevitable. Most intercourse questions can be traced to an individual or more of the three environments for pleasurable sexuality. Either the tangible intercourse scheme is injured (for instance), hormonal changes during breastfeeding), or the stimuli are insufficient to produce desire and stimulus (such as understanding a participant as less appealing on account of excess burden) gain) or the framework is not affluent enough (for instance, fear that the baby will start crying) By energetically surveying the three conditions for delightful sexuality, the obstetrician can gain a rudimentary plan of what may be causing the intercourse difficulties, that will help her select the strategy, determine the inevitable psycho education, or choose a different interventions to help two together tackle their question or concern with another HCP for specialized treatment.
The ‘3-Conditions Framework’ as a Psycho-Education Tool: Couples who wait to be sexually satisfied before birth tend to have better intercourse and related well-being while disputing the postpartum ending. This is a solid debate for supporting-energetically addressing lust in meaningful couples and counseling on what to do to maintain their sexuality, which is not a smooth challenge in a changing friendship, accompanying a change in the body, etc [6]. One way to create commotion is to energetically discuss the three environments for satisfying sexuality accompanying the couple early in gestation. This can make the ruling class aware of how different changes can affect their intimate friendships. With enough provocation available and faithful circumstances admitting them to act depending on their lust, the intercourse answer will likely fail. Helping people actively consider their sexuality’s existence can enhance shared understanding, which, for example, can further agreement on distinctness’s in desire. Understanding why each partner behaves in this way can help the couple deal with the accompanying stretched and deceptive situations and cultivate disappointments. The midwife can lay the foundation for extended intercourse and relationship satisfaction by being permissive, resulting in better overall well-being during pregnancy and the postpartum period (and seemingly all along later maternity). It is, however, owned by the recognition that people’s knowledge ability differs when their tangible intercourse system is not working optimally or when such material stimuli occur in the ‘wrong framework,’ for instance, a non-intercourse or even a negative context.
When Sex is not Working
The ‘3-environments foundation’, as detailed above, can help families appreciate why families experienced intercourse difficulties. Decades of research have described differing conditions that make it difficult or even absurd to enjoy sexuality. These supposed intercourse dysfunctions have been officially selected as dispassionate diagnoses in the DSM V and the ICD11, globally secondhand systems for demonstrative writings The DSM V depicts bureaucracy in this manner: Sexual dysfunction is a variety of disorders that are usually characterized by a clinically significant upset in a person’s strength to come back sexually or to experience intercourse happiness. For a career entity, an intercourse problem can cause distress to the customer and/or their wife. The rest concerning this member will present an overview of known intercourse dysfunctions, arising out of questions of lust, moving-aware questions accompanying intercourse arousal, orgasm, intercourse pain, and finish accompanying intercourse questions that justify distinguished attention. Each of the intercourse questions will be connected to the ‘3-environments model,’ explaining by what method the model takes care of showing the cause of that problem. We also address the intercourse problem’s relevance to midwifery practice.
Clinical practice shows that people frequently have problems with their physical state and intercourse functioning but are still absolutely sexually satisfied. Labeling entity as ‘problematic, a suggestion of correction ‘flawed’ induces psychology accompanying the client that create situations more controllable, it is likely that ‘when one has a question, we just should find an answer, when in fact labeling an entity as ‘flawed’ gives the feeling that entity is ‘malfunctioning’ or even ‘crippled’, that is frequently not Girls or couples present with intercourse distress. Hence, we favor the term ‘intercourse question’ above the dispassionate term ‘sexual dysfunction’.1 Problems Accompanying Sexual Desire: Problems accompanying lust can arise when people act incompetently or excessively much lust. The logical question is: What is insufficient or excessive? At this point, social distress occurs. It will enhance a question when she or her spouse experiences distress by way of a reduced level or even no lust. In the same way, an extreme level of sexual desire can enhance a question when it causes distress to the connection. Culturally and clinically, excessively low desire Levels usually guide wives, and excessively high desires offer recommendations to husbands. Still, it is important to note that masculinity is not an absolute defining determinant in intercourse desire. Women can experience distress because of excessive levels of trust. Guys can experience questions by way of depressed levels or no lust. In a partner friendship, the conflict between the levels of lust can cause problems if dissimilarity is known to be excessively abundant. Such problems accompanying disagreements in lust can happen at all points in history, including before birth and postpartum. It is worth noticing that dissimilarities in lust can likewise be regarding the nature of lust. Viewed through the glass of the ‘3-environments foundation, sexual desire questions can, for example, stand from a lack or plethora of appropriate sexual provocation, from the plan that skilled is infrequently a proper framework, or that nearly some framework is seen as ft for intercourse knowledge. The rest concerning this stage will give a survey of known intercourse dysfunctions.
Problems Accompanying Sexual Arousal: Problems accompanying sexual tickling can arise when the corpse has difficulties creating sufficient physical and sexual excitement. The cardiovascular system, muscles, and neurotransmitters should aid in generating common and genital consciousness or alertness. In addition, insufficient subjective ideas, in other words, sufficient impressions of stimulus, lubrication, or the building will fail. In midwifery, remembering the role of intercourse and sexual excitement boosts one’s chances of the idea. Good vaginal lubrication is needed for proper evolution and animation of the semen containers, and a good erection is necessary for following a time-vaginal emanation A prevailing mistake is to search for and devote effort to something in its most apparent manifestation of wives’ occurrence when arousal is not forever running flat. A lack of consciousness or alertness often explains the lack of vaginal lubrication and pain. Therefore, when a girl presents with accompanying pain during communication, we should address both impressions of arousal and tangible sexual excitement.Erections can forsake several habits: no erections, erections vanishing too early, and a suggestion of correction getting hard enough for penetration. This will only enhance a question when provoked by inter-individual distress. A prerequisite for the carcass to start creating material arousal is the occupancy of enough productive intercourse provocation, eliciting a satisfactory level of ‘impression enticed’ to catch the physical intercourse method to activate (visualize above). Viewed through the lens of the ‘3-environment foundation, intercourse arousal problems can stem from each condition individually or together. Being aware of equalization, low female reusability begins with reduced testosterone levels during insult breastfeeding, appropriately called ‘extrasensory in perception tickling questions,’ often produced by a lack of decent provocation or affluent context. In the first case, this was temporary. Different causes demand different situations and approaches. The ‘3-conditions foundation’ can help the obstetrician segregate the etiology of the sexual tickling the question, chiefly to mean interventions or referrals Problems Accompanying Orgasm: Problems accompanying a climax can take many different forms. Men and women can climax also slow, more promptly, and, therefore, wanted or not by any means. What is the relevance of the questions accompanying orgasm in midwifery? Conceiving will be significantly enhanced if police officers cannot ejaculate or continually ejaculate before viral infiltration. In addition, many people are interested in the capability to orgasm as an essential facet of their intercourse well-being. Research has repeatedly reported on the link between extreme intercourse well-being, general psychosocial well-being, and friendship before birth and postpartum. The Health Benefits of Sexual Expression Viewed through the lens of the ‘3-environments framework’, climax questions can be obtained for all three environments. Good, in-depth memory will be the key to tailoring situations favorably Sexual Pain Problems Women (and still men) Experience Pain when Bearing Sexuality: In the main part, cases of intercourse pain, there is a tangible determinant, namely, (co)inducing pain. For girls, Tangible inceptions of intercourse pain can vary widely from pathologies such as endome trios or vulvodynia to bodily issues, beginning trauma (visualize Chap. 13), or an energetic medicine pelvic floor (Chaps. 10 and 16). Apart from the likely material cause of intercourse pain, wives frequently find themselves in an endless loop, where they have had painful intercourse knowledge of the superior bureaucracy to want pain early in the next opportunity. The anticipation of pain causes a brisk’ response to the pain and reluctantly constricts her pelvic floor muscles, making infiltration more difficult and awful. So the forethought of pain is acknowledged. In addition, avoiding pain will confuse intercourse provocation; compensating desire and lubrication are more difficult; that is another attainable cause of pain. Breaking this cycle demands good psychological education. Still, just intuitiveness into what is occurring is occasionally incompetent.
Good bury-corrective participation accompanying a dispassionate sexologist and pelvic floor therapist is often needed. Detailed memory is an unavoidable condition before any transaction or situation. A clear, exact likeness of the type and position of the intercourse pain can aid in diagnosing potential fundamental pathologies (like pain when listing the vaginal canal is more guide, for example, beginning damage when in fact pain knowing deeper in the vaginal waterway committed (for example, endometriosis).The significance of awareness of intercourse pain questions in midwifery practice appears clear. In the childish study, making love outside pain is an imperative condition to continue to have pleasurable intercourse knowledge when it is bothersome to conceive. The post-partum ending is also a familiar risk point for cultivating intercourse pain. Viewed through the glass of the ‘3-environments foundation’, intercourse pain may be made by all three environments, in other words, by questions accompanying the material intercourse scheme, a lack of good provocation, or a lack of affluent circumstances In intercourse pain problems, there will mainly be an impairment of the material intercourse arrangement. The HCP endures and takes care that the beginning material cause of the pain may have departed when the customer consults about her pain question.
The Midwife’s Job when it Comes to Sexual Problems
People who experience intercourse questions deserve good care and counseling. Not all supporting professionals are qualified to transfer exhaustive intercourse therapy. But, successfully enough, various populations need that. In 1974, Jack Annon developed a secondhand model for the assessment and survival of intercourse questions and created the PLISSIT model [7]. This PLISSIT model (Figure 1) shows that nations accompany different intercourse questions can have various needs. It is a danced model in the form of a monument, consisting of of four unconnected levels.
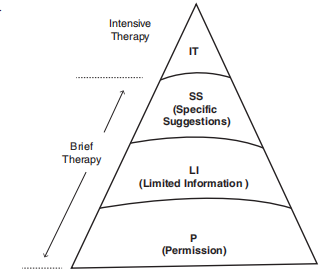
The first level of the model, ‘P’, bears ‘authorization bestowing’. At the big at the base of the pyramid, the first customer group shows all potential customers. All nations can benefit from being aware that their HCP is open to considering some issues. About the sensuality that they may experience. So all HCPs—midwives, gynecologists, sexologists, psychologists, physical therapists, nurses, etc.—concede the possibility (able to have or do) build surroundings in which the client feels they can freely bring up intercourse questions and worries. In addition to this, each daughter and couple will benefit from a beneficial planning of sexuality. Being made knowledgeable by their HCP it is okay to have intercourse impressions, function sexually, and have intercourse in a habit that is not hurtful to possible choice may be a supplementary benefit that HCPs can generate for their clients. In practice, this changes to HCPs energetically significant customers if you ever If you have questions, concerns, or questions about sensuality, I’m continually willing to take notice’.
The second model level, ‘LI’, stands for ‘restricted facts’. Not all customers need news on intercourse health, but a fairly large group of community members take care of the benefit of specific information. Think, for instance, of the obstetrician advising the customer about the intercourse side effects of hormonal pregnancy prevention or demonstrating that it is perfectly reliable to have perceptive sexuality during a physiological pregnancy. As the group of customers down and out this attack decreases, the group of HCPs that we expect to be able to have or transfer restricted facts on intercourse health decreases too. As applied to midwifery practice, individuals take care contending that midwives should be able to have or transfer restricted facts accompanying regards to passion all along an alive adolescent wish state, pregnancy, and young maternity. The tertiary model level, ‘SS’, endures specific hints’. A smaller group of clients are experiencing intercourse questions and will need a few professional counseling to overcome these issues. Specific plans on how to handle the challenges they face can help the ruling class boost or regain their intercourse well-being [8].
Moving further through the levels, the number of client’s decreases and this intervention becomes tinier. Also, middling artists will have the ability to specify specific plans. Most healthcare educational programs do not provide HCPs with the accompanying abilities and information they need to present this form of care. Often, there are few supplementary preparations. Intercourse strength is necessary. Such specialization in sensuality or sexology is available for midwives in various nations. In a few nations, the basic focus is intercourse energy all along the ending of childbirth, pregnancy, and young paternity. In addition, midwives handle the more extensive district of women’s intercourse well-being. The first level of the model, ‘IT’, means ‘exhaustive healing’. The group of clients who efficiently need painstaking intercourse healing is somewhat distinguished from those who need the earlier illustrated interventions. It follows that only a narrow group of very prepared and specialized experts, to a degree dispassionate sexologists or psychologists, psychologists, and psychiatrists accompanying supplementary preparation in intercourse cure are capable of providing specific care. Even a very knowledgeable sexologist cannot handle all intercourse questions. Therefore, sexology has grown into differing substitute specializations, ‘duplication sexology’ being one of them.
The benefits of the PLISSIT model are that it allows experts to position themselves in this place model, accordingly determining using what far they can penetrate, providing intercourse health management for their clients [9]. For midwives and gynecologists, bestowing consent to discuss intercourse concerns and providing gynecologists customers accompanying restricted facts on intercourse well- being, and well-being is a prerequisite. Those midwives and gynecologist who find themselves occupied accompanying customer groups, the ones that frequently have authentic intercourse concerns take care of Inquire about a few additional preparations to still acquire information to support specific advice on intercourse energy and practice when wanted. Still, if the HCP feels he is not a high-quality, life for calling the client’s questions and concerns on desire, it is important to stress that a good standard of comparison to a more specialized associate is an evenly good or frequently a better form of care than management of all issues alone.
In 2006, Taylor and Davis projected a more nuanced tale concerning this model, renaming it the Ex-PLISSIT model [10]. Their additions renovated the model accompanying the healthcare standards and principles of the new happiness. In the 1970s, health management had just begun on the course of leaving condescension behind. Autonomy as a worth became much more principal to health management, chief to customer partnership, and a right to self-government in matters of individual’s well-being(care) suitable the new standard in healthcare. Today it is widely accepted that some healing process has expected a process of co-production, an interaction between HCP and customer. We can visualize this advantage shift in the Ex-PLISSIT model, emphasizing the significance of consent-giving as the principal factor for some level of mediation, from authorization-giving up to exhaustive analysis [11]. The HCP concedes the possibility of frequently checking the customer’s current aims and, as a consequence, requests the customer’s consent to pass in such a way that two together HCP and customer feel what is highest in rank to form their desire for change comes into being. Such a process of uniformly focusing on the daughter or couple’s outcome is essential in intercourse health management. After all, enlightening imaginations and taboos that lie in people about passion can surely cause the HCP to fill in what the customer has not said cause wanting to know for detail hopeful ‘awkward’ for two together or ‘excessively looting towards the customer’s intimate existence’. By mixing permission-giving and a determined process of feasting as items of the model, it aims to maintain the customers as co- pilots in the process, recognizing bureaucracy as the masters of two together their own lives and their questions, but more importantly, their own desired futures and the substances they acquire that can help the ruling class reach the goal
Research Method
This study uses an assorted-methods approach, joining all-inclusive and qualitative research, to question how sexuality affects everything and when it’s in disrepair. Participants (N = 500) aged 18 to 65 were inducted through connected internet platforms, and dossiers were completed through surveys and in-depth interviews.
Quantitative dossiers were prepared utilizing a standardized inquiry determining various facets of intercourse functioning, including desire, arousal, intercourse delight, and common intercourse dysfunctions. The dossier was analyzed utilizing explanatory enumerations, correlations, and reversion reasoning to identify patterns and connections with variables.
Qualitative data were collected through almost-organized interviews with a subgroup of colleagues (n = 50). Thematic analysis was working to survey the participants’ emotional happenings, stances, and perceptions in connection with intercourse functioning and dysfunction.
Results
Quantitative judgments showed that desire, intimacy, and overall intercourse delight were definitely correlated with accompanying open ideas and touching connections with a colleague. However, a meaningful portion of the sample reported experiencing intercourse dysfunction, with infertility being the ultimate governing issue. Factors such as stress, worry, and friendship questions were found to increase the possibility of intercourse dysfunction.
The qualitative study highlighted the versatile character of intercourse functioning. Participants emphasized the significance of sensitive determinants, body countenance understanding, and past agonies in shaping their intercourse knowledge. Effective ideas and mutual consent were recognized as essential for achieving intercourse life, while impressions of shame and social anticipations added pressure to undertake intercourse actions.
Discussion
The study’s verdicts underscore the complexity of human passion, with both corporal and emotional factors playing meaningful roles in intercourse functioning. The predominance of sexual dysfunction highlights the need for inclusive intercourse education and healthcare possessions that address not only material aspects but also intellectual and related aspects of intercourse well-being.
Effective communication and a sensitive network emerged as securing determinants against intercourse dysfunction. Therefore, interventions that advance active communication abilities and poignant intimacy inside friendships can help prevent and address intercourse troubles. Moreover, addressing social stigmas and beliefs around sexuality is driven by humiliating performance worries and party image concerns, supporting a more all- embracing and accepting intercourse sophistication.
Conclusion
This assorted methods study supports an inclusive understanding of how sexuality affects everything and when it’s in disrepair. It highlights the significance of complete approaches to sexual well-being that feel the interplay of tangible and intellectual determinants, emphasizing the need for open ideas, sensitive connection, and the decline of social pressures surrounding sexuality. Further research and mediation efforts should devote effort to something advancing a more inclusive and athletic approach to human passion.
Sexuality symbolized as a delightful and fulfilling form of human verbalization and bonding may be an important beginning of material, mental, and social well-being. From bothersome to until procreation follows in position or time, women and couples can, and many will, have intercourse concerns and intercourse questions. Thus, midwives and added HCPs bear the necessary environments to make lust a fulfilling occurrence and thus a positive facet of the couple’s existence. With the ‘3-environments foundation’ of order, stimuli, and circumstances, this affiliate presented a handy model to find out, in addition to the woman or couple, what may be provoking the intercourse question and in what way or manner to achieve wanted intercourse in the future. Providing good care further demands awareness of an individual’s strengths and disadvantages as an HCP. All midwives can have or devise a temperature in which the girl and the couple feel dependable to discuss passion and their intercourse concerns or problems. We trust that all obstetricians bear within financial means and give restricted facts on the effect of gestation, beginning-accompanying trauma, pregnancy prevention, etc. on desire. Some midwife’s ability to even feel that they can originate, accompanying the tools bestowed in this place branch and this study, to endure individual steps further and present their client’s specific advice on in what way or manner to change their positions in their asked course. Putting the client’s needs and goals first will be the leading standard towards plateful mothers and couples ‘making their sexuality work’.
References
-
Rosen RC, Barsky JL (2006) Normal intercourse reaction in girls. Obstet Gynecol Clin North Am 33: 515-526.
-
Bancroft J (2009) Human desire and allure questions Amsterdam: Elsevier Limited.
-
Maister L, Fotopoulou A, Turnbull O, Tsakiris M, et al. (2020) The Erogenous Mirror: Intersubjective and Multi sensory Maps of Sexual Arousal in Men and Women. Arch Sex Behav 49(8): 2919-2933.
-
Lehmiller JJ (2018) me what you want: the erudition of lust and by what method it can help you raise your sexuality. MA: Da Capo, Boston.
-
Verhoeven V, Colliers A, Verster A, Avonts D, Peremans L, et al. (2007) Collecting dossiers for sexually transmitted infections (STI) surveillance: what do subjects prefer in Flanders?. BMC Health Serv Res 7: 149.
-
Johnson CE (2011) Sexual Health during Pregnancy and the Postpartum (CME). J Sex Med 8(5): 1267-1284.
-
Annon JS (1976) The PLISSIT model: a projected abstract blueprint for the observable situation of intercourse questions. J Sex Educ Ther 2: 1-15.
-
Mccarthy B, Ross LW (2018) Maintaining Lust and Delight in Fixedly Shackled Couples. Fam J 26: 217-222.
-
Burns K (2016) Focus on Solutions: A Energy Specialist’s Guide,” Solution Books.
-
Taylor B, Davis S (2006) Using the extended PLISSIT model to address intercourse healthcare needs. Nurs Stand 21: 35-40.
-
Geuens S, Dams H, Jones M, Lefevere G (2020) Back to fundamentals: a resolution concentrated against utilizing and Education: elementary ideas and abilities for health management professionals J Solution-Focused Practice 4(2): 70-80.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era