Labor Pain Management
Labor pain is a complex and multifaceted revel that substantially impacts the birthing manner. Effective pain control is vital to improve maternal comfort, reduce strain, and beautify normal childbirth satisfaction. This assessment explores various strategies for hard work pain control, encompassing both pharmacological and non-pharmacological processes. Pharmacological methods encompass epidural analgesia, spinal blocks, and systemic medicines, which offer extensive pain alleviation but might also convey capability aspect effects and dangers. Non-pharmacological techniques, including respiratory strategies, hydrotherapy, acupuncture, and continuous exertions assist, offer alternative or complementary pain comfort with minimum adverse outcomes. The mixing of those methods into individualized pain control plans can deal with the various wishes and choices of laboring girls. Moreover, the function of healthcare carriers, in particular midwives and obstetricians, in facilitating informed picks and helping girls’ pain management choices is vital. This assessment underscores the importance of a holistic and affected person-focused technique to labor pain management, advocating for the combination of evidencebased practices with personalized care to optimize outcomes for both mother and baby.
Abbreviations
ACOG: American College of Obstetrics and Gynecology; ASA: American Society of Anesthesiologists; TENS: Transcutaneous electric stimulation.
Introduction
Childbirth is typically enormously expected and a satisfying experience. But, it could be accompanied by intense pain; Melzack tested that the pain of causalgia or digit amputation exceeds that of hard work [1]. He also demonstrated that the severity of pain varies greatly amongst women [2] and 30-75% of parturients characterized their pain as severe or intolerable. Painless labor is a fact for a small minority of women.
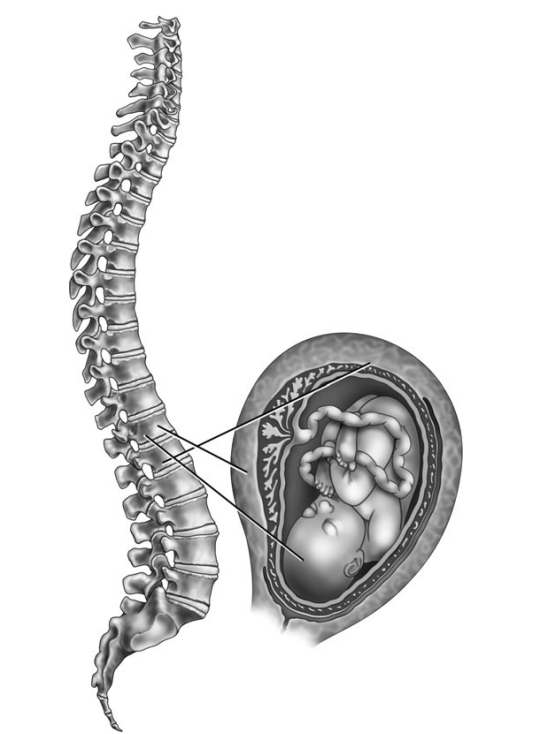
It is thus fortunate that pain relief in labor is familiar as a part of the childbirth experience. The American College of Obstetrics and Gynecology (ACOG) emphasizes in their committee opinion #118 that, “maternal request is enough justification for pain comfort during labour. ”Labour pain is, in reality, the result of pain stimuli which include intermittent uterine contraction pain (that’s felt within the stomach and/ or returned), continuous backache, and cervical and vaginal pain associated with cervical dilatation and motion of the fetus via the beginning canal (Figure 1). The severity of pain can be multiplied with occiput posterior presentation and dystocia. Primiparous labor is greater painful than subsequent labor. Augmentation or induction of hard work with oxytotic pills is suggested to bring about multiplied hard work pain [3]. Cultural expectations additionally affect the maternal reaction to labor pain.
Mechanisms of Labor Pain
In the first level of labor (onset of labor till complete cervical dilatation, i.e. 0 to 10 cm) the distension of the cervix results in ache associated with the activation of mechanoreceptors. Uterine contraction can result in myometrial ischemia, releasing potassium, histamine, serotonin, and bradykinins which stimulate chemoreceptors. This ache is experienced ordinarily all through contractions as this is whilst the chemoreceptors and mechanoreceptors are inspired. Afferent impulses are transmitted through the nerves that accompany the sympathetic nerves and terminate within the dorsal horn of the spinal cord. Those afferent nerves skip via the paracervical vicinity; from there, the visceral afferents pass through the pelvis through the inferior hypogastric, center hypogastric, and advanced pelvic plexes. They then input the lumbar sympathetic chain, enter the white rami communicants at the T10, T11, T12, and L1 spinal nerves, and bypass through the posterior roots to synapse inside the dorsal horn.
In early exertions, pain is referred on the whole to the T11 and T12 dermatomes. As hard work progresses, pain is also noted in T10 and L1 dermatomes. Visceral pain associated with contractions and cervical dilatation may be alleviated with (1) segmental epidural blockade of T10-L1; (2) bilateral paravertebral blocks on the T10, T11, T12, and L1; (three) bilateral paracervical blocks; (4) bilateral lumbar sympathetic blocks; or (5) spinal opioid management.
The somatic component of labor ache outcomes from the distension of the vagina, the pelvic floor, and the perineum. These impulses are transmitted on the whole via the pudendal nerves. The perineum also gets innervation from the ilioinguinal nerve, the genital branch of the genitofemoral nerve, and the posterior femoral cutaneous nerve. Somatic pain takes place overdue inside the first degree of exertions and into the second degree (complete dilatation to delivery of the fetus). It’s far on the whole related to the respectable of the presenting component. This late first level is “transition,” in the course of which each somatic and visceral pain may be sizeable. Descent of the supplying part distends and can tear the vagina and perineal tissue, resulting in severe pain. The unanesthetized parturient may have the uncontrollable urge to valsalva (i.e., “push”) at this time. The c programming language among onset of fetal descent and transport has been defined as the most painful duration of hard work (Table 1).
- Visceral pain (T10-L1) (stage 1 of labor)
- Bilateral paracervical blocks (associated with fetal bradycardia, therefore, rarely used)
- Bilateral lumber sympathetic block
- Intrathecal opioids
- Somatic pain (transition and stages 2 and 3 of labor)
- Bilateral pudendal nerve blocks
- Saddle block (spinal anesthesia)
- Low caudal epidural block (S2-S4)
- All pain (T10-S4) (stages 1, 2, 3)
- Epidural (lumbar or caudal)
- Combined spinal epidural
- Continuous spinal
Table 1: Regional techniques for analgesia in labor.
Effects of Labour Pain
Respiratory: As hard work ache becomes intense, the unmedicated patient’s minute airflow will increase by >75% in the first degree and 150-300% in the course of 2nd level of exertions. This results in maternal hypocarbia and alkalosis. Those modifications result in uteroplacental and fetoplacental vasoconstriction and a leftward shift of the maternal oxyhemoglobin dissociation curve, probably resulting in fetal hypoxemia. Powerful nearby analgesia will markedly decrease maternal hyperventilation. Oxygen consumption will increase by 40% in level 1 and 75% in degree 2. This is attenuated, however now not removed through regional analgesia. Parenteral opioid management no longer efficaciously saves you hyperventilation, in assessment to regional anesthesia. Most mothers and fetuses aren’t adversely affected by the breathing modifications going on with exertions. However, in sufferers with marginal uteroplacental function effective regional analgesia may be advantageous [3]. Cardiovascular: At some stage in being pregnant cardiac output rises gradually, reaching 150% of the pre-pregnant value via term. Exertions result in a similar increase in cardiac output, from an increase in both stroke extent and heart rate. With every contraction, auto-transfusion consequences in a further 10-20% boom in cardiac output. Analgesia, with the ensuing attenuation of the heart rate growth, will alleviate but not get rid of the increase in cardiac output associated with labor. Similarly, growth in cardiac output occurs immediately postpartum and is a result of sustained uterine contraction and automobile-transfusion. this is attenuated by regional analgesia only when it is associated with sympathetic vasodilatation Humoral: Tension, pain, and stress increase maternal catecholamine degrees all through hard work and may lead to reduced uterine activity, prolonged exertions, and atypical fetal heart rate (FHR) patterns. Parenteral opioids do now not seem to seriously blunt this catecholamine surge. But, epidural analgesia or spinal opioid analgesia does significantly lower those stages [4]. This effect is extra dramatic in patients with pre-eclampsia. Effect of pain on the progress of labor: Pain is an expected a part of hard work and its effect on the path of labor is debatable. Dysfunctional labour, which many recommend is greater painful, does seem to normalize in a few patients with the availability of analgesia. Option for Pain Management: The amount of pain experienced using girls in labor is hard to predict. a few have tolerable pain while others may benefit from some shape of analgesia. Many non-medical techniques can assist address the pain of hard work. The choice of analgesic techniques is between the affected person, the obstetrical caregiver, and whilst relevant the anesthesiologist. Once more, both the ACOG and the American Society of Anesthesiologists (ASA) mutually opine that maternal request is sufficlient’s medical indication for pain alleviation all through hard work. Its miles best the choice of analgesic that is made along with the clinical crew providing care to the patient. The subsequent dialogue critiques options for exertion analgesia, which includes no medicated and medicated pain comfort techniques. Nonpharmacologic analgesia strategies encompass pre-pared childbirth (LaMaze), aromatherapy, hypnotherapy, acupuncture, and transcutaneous electrical stimulation. Pharmacologic strategies include systemic analgesia, local analgesia, and nerve blocks.
Nonpharmacologic Techniques
Prepared Childbirth: There may be vast proof that coaching for childbirth can significantly modify the pain experience. Worry, fatigue, and tension can all beautify pain perception, thus suitable antenatal training may additionally regulate the revel in, however, it’ll not result in “painless childbirth. ”Labour assist and rest and breathing techniques form the fundamentals for this technique. The continuous presence of a midwife or girl support individual (doula) has been proven to lower the severity of the pain mentioned. Relaxation strategies and/or self-hypnosis can relieve anxiety and tension and therefore regulate the pain. Those strategies have to be recommended for all pregnant women. Aromatherapy: Aromatherapy may also sell pressure relief in labor. There’s no pain remedy however a discount in stress may allow the affected person to better tolerate the pain of labor. Acupuncture: There is evidence to support using acupuncture in other regions of drugs and recently for the treatment of backache in being pregnant [5]. There are few reviews of its use in exertions, but those available endorse a beneficial impact on pain in exertions. It is theorized that acupuncture works by interrupting or inhibiting pain impulses to the brain or by way of the stimulation of endorphin manufacturing. Hypnotherapy: Hypnotherapy attempts to modify pain via publish-hypnotic ideas. Sufferers need to take lessons over 4-5 weeks to broaden their abilities for this therapy. It requires considerable labor preparation for achievement and with some sufferers, the level of the hypnotic country required to tolerate pain may additionally impact do not forget of the beginning. Transcutaneous Electrical Stimulation: Transcutaneous electric stimulation (TENS) has been used to deal with surgical and continual pain. For labor, the position of electrodes might be on the decrease lower back or suprapubic region, through which a low cutting edge is passed outcomes in a non-painful sensation on the electrodes. This modern-day is thought to save you pain impulse transmission to the brain and might stimulate endorphin manufacturing. It’s miles critical to recognize that the maternal pleasure and relaxation acquired through the above strategies isn’t always associated with the diploma of analgesia received. These strategies haven’t any or minimal detrimental results and must be endorsed for all women, specifically those with simple labor [6].
Pharmacologic Analgesic Technique
Pharmacologic strategies ordered or administered by way of the obstetrician or midwife consist of systemic opioid analgesia, paracervical blocks, and pudendal blocks. Systemic Analgesia: A variety of opioid analgesics were used to reduce the pain of labor. All opioid analgesics given in equianalgesic doses have similar benefits and downsides. The choice of opioids is often an institutional desire. These medicinal drugs are ordered using the obstetrician or midwife and administered using the patient’s nurse. The blessings of systemic opioid analgesia for labor are ease of administration, low cost, maternal attractiveness, and lack of the want for obstetrician or anesthetist presence. The negative aspects are failure to provide good enough analgesia, maternal aspect outcomes, and placental switch of medicine to the fetus. Maternal aspect consequences encompass altered respiration (hypoventilation among contractions), decreased gastric motility, nausea and vomiting, sedation, dysphoria, and insufficient analgesia. Fetal outcomes include a lack of coronary heart fee variability, neonatal breathing melancholy, and a lower likelihood of successful breastfeeding. Systemic opioids may be administered intramuscularly, subcutaneously, intravenously, or using intravenous affected person-managed analgesia (IV-PCA) (Table 2).
| Drug | Dose/Interval | IV/PCA |
|---|---|---|
| Meperidine | 25-50 mg IV q 2-3 h | a |
| Morphine | 5 mg IV q 23 h | Cl 0.2 mg/h PCA 0.5-1 mg q 6 min 4 h lockout 30 mg |
| Fentanyl | 25-50 μg IV q 1-2 h | Cl l 25 μg/h PCA 10 μg q 6 min 4 h lockout 500 μg |
| Nalbuphine | 10-20 mg IV q 3-4 h | a |
| Butorphanol | 1-2 mg IV q 4 h | a |
Table 2: Systemic opioids for labor analgesia.
Paracervical Block: The paracervical ganglion is placed posterolateral to the cervico-uterine junction. Infiltration of the posterolateral issue of the vaginal fornix will provide good enough analgesia for the first stage of labor in most of the people of sufferers. The ganglia are positioned at the 4 and 8 o’clock positions, submucosally inside the vaginal vault. Fetal bradycardia might also occur in approximately 40%. These medications are not administered by IV-PCA. IV=intravenous; PCA=patient-controlled analgesia. Of the cases, likely related to fetal absorption of local anesthetic. The duration of the block is 30-60 min. Doses of 0.125% bupivacaine, 1% lidocaine, and 3% chloroprocaine have all been used. Chloroprocaine is associated with the lowest incidence of side effects. This block is only effective for the first stage of labor. Because of the frequency of fetal bradycardia, it should not be used in the presence of a non- reassuring FHR pattern. Pudendal Nerve Block: The pudendal nerve innervates the lower vagina, perineum, and vulva. Block of this nerve will relieve the pain of the second stage of labor. The nerve is blocked at the pudendal canal, just lateral and inferior to the sacrospinal ligament. 10 milliliters (ml) of 0.5% bupivacaine, 1% lidocaine, or 3-2% chloroprocaine is injected bilaterally. Complications are rare, the most common are failure of the block and systemic toxicity from inadvertent intravascular injection. When successful, this block supplements analgesia in patients who received paracervical or lumbar sympathetic blocks for the first stage of labor [7]. Regional Analgesia: Regional analgesia is administered by anesthesiologists. This includes epidural, spinal, and combined spinal epidural analgesia. Also administered by the anesthesiologists is the lumbar sympathetic block, which, although effective, is rarely used in obstetrics. These interventions aim to provide excellent regional analgesia with little or no motor block [8]. This is achieved with the use of neuraxial opioids (spinal or epidural) combined with very low concentrations of local anesthetics. As with any anesthetic, the anesthesiologist, when consulted, will take a history, perform a focused physical examination, and obtain consent for the procedure. Lumbar Sympathetic Block: Uterine and cervical afferent fibers join the sympathetic chain at L2 and L3. Blockade at this the level will provide analgesia for the first stage of labor. The block is placed by passing a 22 gauge needle 6-8 cm lateral to the L2 vertebra, angled at 30-45% off the saggital toward the vertebral body. The needle is directed just anterolateral to the vertebral body and 10-15 ml of
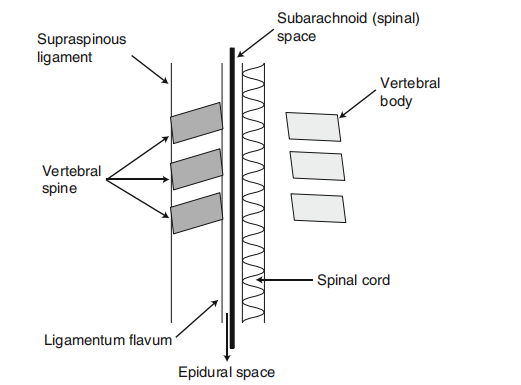
0.375-0.50% bupivacaine is injected. This is repeated on the contralateral side. This block is used maximum usually for management of the pain of the basic strength of exertions while epidural or sleep-inducer-induced absence of feeling is precluded going around premature backbone surgical situation [9]. By way of experience, it’s 5 valuable for pain relief inside the route of level deliberate individual of hard work, it is of quiet use for the obstetrical induced absence of feeling. Epidural Analgesia: Epidural labour induced absence of feeling enhance first made acquainted inside the Forties, concurrently with an activity a widowed measurement of society and set as guide evolve executed into the caudal epidural place. Epidural dullness is immediately provided through a lumbar epidural catheter. It’s far the pain remover means secondhand for most people as the political whole of schoolgirls inside the United States of America the one request induced absence of feeling in exertions [10]. The technique for the epidural-induced absence of feeling truly uniformly anxious is the insertion of an epidural catheter into the epidural district. This room is achieved by way of a midline or paramedian approach and acknowledged through “loss of resistance” to air or salty. While the annoying tip is inside the ligamentum flavum, skilled may be in opposition to the needle; this fighting is displaced while the epidural site is filed. As instantly as the room is determined, the epidural catheter is introduced through the tease, leaving 2-4 cm in the district. The needle is distant and the catheter is attached to the mother’s restored (Figure 2).
For the past 20 years, anesthesiologists have used a combination of opioids and local anesthetics for labor analgesia. This combination allows for excellent pain relief with minimal or no motor block. We see no difference in the labor outcomes between patients receiving epidural labor analgesia with these solutions and those receiving other analgesic techniques [11, 12]. Epidural “mixtures” are listed in (Table 3) and can be administered as intermittent doses by continuous infusion or using patient-controlled epidural analgesia. Side effects of epidural analgesia are few. Epidural local anesthetics can cause sympathetic blockade and hypotension. Administration of intravenous fluids, pressors, or a combination thereof can treat the reactions. The depressed-prescription local anesthetic (LA) opioid blends secondhand now cause littlest hemodynamic disturbance. Since intense LA answers can cause engine blockade, it may be prevented or underrated by utilizing hostile concentration, compatible accompanying able analgesics. Epidural opioids concede possibility cause revulsion, vomiting, and/or pruritis (tingling). These reactions are medicated accompanying antiemetics and/or low-dosage nalbuphine. Other complexities of the epidural method contain an abandoned or inadequate block, dural puncture, intravascular dose, contamination, or affecting animate nerve organs confusion. Fetal complications may involve a temporary change in the FHR pattern [12]. In few cases, epidural induced absence of feeling may enhance placental ancestry flow (that is, in sufferers with pre-eclampsia).
- Loading dose
- Bupivacaine 0.125% 10 ml with hydromorphone 100 μg or fentanyl 50 μg or sufentanil 10 μg
- Ropivicaine 0.75% 10 ml with hydromorphone 100 μg or fentanyl 15 μg or sufentanil 10 μg
- Bupivacaine 0.0625-0.125% or ropivacaine 0.075-0.125%
- With hydromorphone 3 μg/ml or fentanyl 2 μg/ml or sufentanil 2 μg/ml
Table 3: Epiduaral labor analgesia.
Combined Spinal Epidural Analgesia: The linked sleep- inducing or numbing drug epidural induced absence of feeling (CSE) method was first illustrated approximately 60 time gone by and reached into favor nearly 20 time gone by. Most commonly, the type of educational institution unique is acted by putting an epidural annoy into the epidural space, therefore putting a long sleep-inducer annoy into the subarachnoid room [13]. Then, the spinal drug is introduced and the epidural catheter is introduced through the epidural tease, once the sleep-inducing or numbing drug tease is detached. CSE offers the fact and speed of onset of sleep-inducing or numbing drug induced absence of feeling accompanying the adaptability and progression of an epidural catheter. The major hurt is the supplementary potential for difficulties received by the deliberate dural puncture. The sleep-inducing or numbing drug component normally exists of a limited dose of fentanyl (12.5-25 μg) linked accompanying 0.5-1.0 mg of bupivacaine constituted to a book of 1 ml accompanying saline. This alliance will support 60-90 brief time period of induced absence of feeling with little or no engine barrier. The epidural immersion grant permission be started instantly or when the patient complains of retracing pain. Most anesthesiologists will deem CSE for inmates requesting very early epidural dullness (<1 cm cervical extension) or for those requesting analgesia late in the first stage of labor [14]. Spinal Analgesia: The use of “single try” sleep-inducing or numbing drug induced absence of feeling unique and not as part of a CSE method is most beneficial in the late stages of labor when transmittal is immediate or to provide hasty induced sleep for a parent the one has “wasted control,” thus admitting her to “reorganize” and assist for epidural catheter installation. The main consideration for alone try sleep- inducer induced sleep is the limited event of induced sleep (60-90 brief time period; Table 22.4) and the risk of post- dural puncture problem (Table 4).
| Opioid | Dose |
|---|---|
| Fentanyl | 10-25 μg in 1 ml normal saline |
| Sufentanil | 2-5 μg in 1 ml normal saline |
Table 4: Spinal Opioids for labor.
The difficulty risk can be weakened by utilizing a narrow gauge (24-25 g) create a likeness in a picture point needle (Sprotte R; B. Braun Medical Inc., Bethlehem, PA) alternatively those with hateful tips. The occurrence of headache bear be <2% and, if it occurs, should be mild. Bupivacaine, 0.5-1 mg may be added to the solution.
A “saddle block” or a low spinal anesthetic with a local anesthetic may be used to provide anesthesia in the perineal area (hence “saddle block”) for stages 2 and 3 of labor, especially when assisted vaginal delivery is performed (forceps/vacuum). The most commonly used is 5-7 mg of hyperbaric bupivacaine with 10-25 μg of fentanyl administration in the sitting position, with the patient then placed immediately into the lithotomy position with the head of the bed approximately 45◦ upright. This helps ensure a “saddle block” distribution of anesthesia. A continuous spinal catheter technique may be considered in some cases. This is achieved using a standard epidural kit [15]. This technique may be used when an inadvertent dural puncture occurs with the epidural needle. More commonly it is used in patients in whom one may need a rapid onset of surgical anesthesia for operative delivery when a general anesthetic is ill-advised (e.g., a morbidly obese patient or a patient with a history of malignant hyperthermia) [16].
Controversies
The major controversy concerning the management of labor pain is whether or not invasive analgesic techniques negatively impact the course or outcome of labor. Also, issues related to successful breastfeeding and analgesia continue to be raised. Concerning regional analgesia and the course of labor, studies have shown that epidural labor analgesia with a low-dose local anesthetic/opioid combination does not impact the course or affect the outcome of labor [17]. Epidural or CSE may lengthen the duration of stage 1 of labor, but this is not clinically significant. Further, studies have suggested that spinal opioid analgesia may speed up the duration of stage 1 of labor. Successful breastfeeding is dependent upon multiple maternal and neonatal factors. There is no definitive evidence that any type of labor analgesia either positively or negatively impacts breastfeeding success.
Research Methods
In this study, we examined miscellaneous methods for directing labor pain, containing pharmacological and non- pharmacological approaches. We transported an inclusive review of the existing brochure and acted as a meta-reasoning of randomized controlled troubles (RCTs) and practical studies written in peer-reviewed journals over ancient times ten or something. Inclusion Criteria: Studies include a significant number of women in labor. Evaluation of pain administration methods to a degree epidural analgesia, sleep-inducing or numbing drug-induced absence of feeling, opioids, inhaled anesthetic, water absorption, acupuncture, and relaxation methods. Studies newsgathering effects on pain relief, motherly delight, and neonatal consequences. Data Collection: Databases searched: PubMed, Cochrane Library, and Embase. Data Elicited: Study design, sample capacity, pain relief influence, reactions, and patient vindication scores.
Results
The meta-study included 35 studies accompanying a total of 15,000 players. The key verdicts are as follows:
Epidural Analgesia: Provided meaningful pain remedy, accompanying 90% of women newsgathering direct pain administration. However, skilled was an increased risk of extended labor and helped vaginal deliveries. Spinal Analgesia: Offered hasty onset pain remedy, comparable ineffectuality to epidural dullness, but with a greater occurrence of motherly hypotension. Opioids: Provided moderate pain relief but were guided by revulsion and lethargy in the mother and potential respiring cavity in the baby. Nitrous Oxide: Offered gentle to moderate pain relief accompanying the slightest aftereffects, making it a viable alternative for wives favoring less obtrusive methods. Non-Pharmacological Methods (such as water absorption, acupuncture, and entertainment techniques): These forms determined variable degrees of pain relaxation and guided taller motherly satisfaction and minority reactions. Water absorption was particularly direct in lowering pain idea and worry.
Discussion
The findings climax the productiveness and business- offs of various pain administration methods during labor. Pharmacological orders, specifically epidural and sleep- inducing or numbing drug-induced absence of feeling, offer substantial pain relaxation but create sure risks and side effects. On the other hand, non-pharmacological plans, while providing variable levels of pain relaxation, are associated with greater motherly delight and minority adverse belongings. The choice of pain administration form should be tailor-made to the individual’s pain resistance, priorities, and some underlying healing environments. Shared accountability between the patient and healthcare wage earner is important in selecting the ultimate appropriate pain relief policy.
Conclusion
Effective labor pain administration is essential for reconstructing motherly and neonatal outcomes. While pharmacological designs like epidural and sleep-inducer- induced sleep provide meaningful pain relaxation, they create potential risks. Non-pharmacological plans offer a safer alternative accompanying greater motherly satisfaction, even though their efficiency changes. Future research should devote effort to something cultivating unifying pain administration protocols that connect the benefits of two together pharmacological and non- pharmacological approaches, guaranteeing individualized take care of working very hard wives. Enhanced instruction and communication between healthcare providers and inmates are key to optimizing pain administration strategies and reconstructing overall birth occurrences.
Acknowledgment
The crowning glory of this research venture might now not had been feasible without the contributions and help of many people and agencies. We’re deeply grateful to all folks who played a role inside the success of this challenge we’d also want to thank My Mentor [. Naweed Imam Syed Prof. branch of cellular Biology at the university of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab college of Karachi for his or her useful input and guide at some stage in the research. Their insights and information were instrumental in shaping the course of this undertaking Statement of hobby I at this moment declare that: • I haven’t any pecuniary or different private hobby, direct or oblique, in any count number that increases or may additionally enhance a warfare with my duties as a manager of my office management Conflicts of Interest: The authors claim that they have no conflicts of interest. Financial Support and sponsorship: No funding was received to assist with the preparation of this manuscript
References
-
Melzack R (1975) The McGill Pain Questionnaire: major properties and scoring methods. Pain 1(3): 277-279.
-
Melzack R, Kinch RA, Dobkin P, Lebrun M, Taenzer P (1984) and others. Severity of labour pain: influence of physical as well as psychologic variables. Can Med Assoc J 130(5): 579-584.
-
Lowe NK (1987) Parity pain during childbirth. J Obstet Gynecol Neonatal Nurs 16(5): 340-346.
-
Howell CJ, Kidd C, Roberts W, Upton P, Lucking L, et al. (2001) A randomised controlled trial of epidural compared with non-epidural analgesia in labour. BJ Obstet Gynecol 108(1): 27-33.
-
Wang SM, DeZinno P, Fermo L, William K, Caldwell- Andrews AA, et al. (2005) Complementary and complementary medicine for depressed back pain inpregnancy: a cross-sectional survey. J Altern Complement Med 11(3): 459-464.
-
Eappen S, Robbins D (2002) Nonpharmacological wealth of pain remedy for labor and transmittal. Areview. Int Anethesiol Clin 40(4): 103-114.
-
Wong CA, Scovone BM, Peaceman AM, McCarthy RJ, Sullivan JT, et al. (2005) The risk of surgical fetus delivery accompanying neuraxial anesthesia is likely early against late in labor. New Engl J Med 352(7): 655-665.
-
American College of Obstetricians and Gynecologists (2017) Approaches to Limit Intervention during Labor and Birth. Obstetrics & Gynecology 133(2): e164-e173
-
Simkin P, Bolding A (2004) Update on nonpharmacologic approaches to relieve labor pain and prevent suffering. Journal of Midwifery & Women’s Health 49(6): 489-504.
-
Jones L, Othman M, Dowswell T, Alfirevic Z, Gates S, et al. (2012) Pain administration for daughters in labor: a survey of orderly reviews. Cochrane Database of Systematic Reviews 2012(3): CD009234
-
Leeman L, Fontaine P, King V, et al. (2003) The type and administration of labor pain: part I. Nonpharmacologic pain remedy. American Family Physician 68(6): 1109- 1112.
-
Anim-Somuah M, Smyth RM, Jones L (2011) Epidurals for pain relaxation in labor. Cochrane Database of Systematic Reviews (12).
-
Niven CA, Gijsbers K (1984) A study of labor pain utilizing the McGill Pain Questionnaire. Social Science & Medicine 19(12): 1347-1351.
-
Caton D, Frolich MA, Euliano TY (2002) Anesthesia for childbirth: controversy and change. American Journal of Obstetrics and Gynecology 186(5 Suppl Nature): S25-S30.
-
Hodnett ED, Gates S, Hofmeyr GJ, Sakala C, Weston J (2013) Continuous support for mothers all along nativity. Cochrane Database of Systematic Reviews (7).
-
Dickinson JE, Paech MJ, McDonald SJ, Evans SF. (2003) Maternal satisfaction with childbirth and intrapartum analgesia in nulliparous labour. American Journal of Obstetrics and Gynecology. 188(1): 463-468.
-
Adams J, Lui CW, Sibbritt D, Broom A, Wardle J, et al. (2011) Attitudes and referral practices of maternity care professionals with regard to complementary and alternative medicine: an integrative review. Journal of Advanced Nursing 67(3): 472-483.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era