Postoperative Evaluation of Patients Operated with the New Technique for Stress Urinary Incontinence
Objectives: Our study aims to bring a new perspective to stress urinary incontinence surgery. Material and Methods: 300 female patients diagnosed with stress incontinence urodynamically between January 2013 and 2023 were included in the study. The complete recovery status of the patients after the operation was examined. Our study is based on a new surgical technique. Preoperative evaluation included history, physical examination, stress test, 1-hour pad test, urine culture, 7-day voiding diary, residual urine measurement, and urodynamic examination. In postoperative evaluation, intraoperative and postoperative complications such as stress test, 1-hour pad weighing test, operation time, urinary tract infection, urination problems, de novo urgency symptoms, and urinary retention were taken into consideration. SPSS (IBM SPSS for Windows, Ver.26) statistical package program was used for the statistical analysis of our study. Results: The average age of the patients is 46.19. The average duration of stress incontinence in patients is 6.85 years. Incontinence was observed in 6 patients after the operation. Complete cure was achieved in 294 of the patients and it was found to be statistically significant (p=0.000). The success rate of the method was found to be 98% in our study. The changes in the stress test and Q-type test results before and after the operation were found to be statistically significant (p=0.000). The changes detected in the postoperative pad test were found to be statistically significant (p=0.004). Urinary retention was observed in 12 patients due to the operation. Conclusion: The success of our operation is quite high compared to the literature. It is an effective and safe method in the treatment of stress incontinence.
Abbreviations
AUA: American Urological Association; MMK: Marshall Marchetti Krantz; BMI: Body mass index; TVT: Tension- free tapes; MUS: Mid-urethral slings; FDA: Food and Drug Administration.
Introduction
Urinary incontinence is defined by the International Continence Society as ‘involuntary loss of urine that is a social or hygienic problem’. In community studies, it is estimated that 20-30% of women are affected, but only 7-12% perceive it as a problem [1].
Stress urinary incontinence treatment was updated again by the American Urological Association (AUA) in the panel convened in 2011, by evaluating large meta-analyses [2].
Accordingly, the first step of stress incontinence treatment is conservative treatments consisting of behavioral treatments, drug therapy, and pelvic floor exercises. For patients who cannot benefit from this step, the most appropriate alternative for the patient should be chosen among surgical treatment options. Surgical methods used today in the treatment of stress incontinence are retropubic suspensions (open and laparoscopic Burch operation), sling operations, of which many types have been described, periurethral injections, and artificial urinary sphincter applications [2]. The most well-known retropubic urethropexy procedures are Marshall Marchetti Krantz (MMK) and Burch operations. MMC cystourethropexy is based on the transabdominal suspension of the vesicourethral junction or bladder neck to the periosteum of the symphysis pubish [3] .
Our practice is to place a non-absorbable 2/0 polyester suture under the vesicourethral junction transvaginally. It should not be confused with the classic Kelly plication. In the classic Kelly plication, the pubocervical fascia under the bladder neck is brought closer to the midline and plicated, and the bladder neck and proximal urethra are lifted and supported. Absorbable sutures are preferred [4].
The prominent advantages of our technique are the use of non-absorbable sutures, the placement of sutures in the vesicourethral junction, the use of solid tissues such as muscle fascia, and the fact that all these procedures are performed transvaginally, unlike the MMK operation.
Materials and Methods
Place and Time of Research
Our research was conducted at Uşak University Training and Research Hospital, Department of Gynecology and Obstetrics, between January 2013 and January 2023. Our study is a prospective clinical study on a new technique in incontinence surgery.
Research Population and Sample
The population of the research consists of patients who underwent surgery in our hospital with the diagnosis of stress urinary incontinence between January 2013 and January 2023. Our study was planned on 319 female patients. However, 2 of our patients died due to myocardial infarction and 1 patient died due to cerebrovascular accident. 16 patients included in the study were excluded from the study because their last follow-up data could not be accessed. Our study was conducted with a total of 300 patients. Our study was conducted on female patients over the age of 18. Patients who were diagnosed with stress incontinence and gave consent for the operation were included in the study. Patients who were not diagnosed with stress incontinence and did not consent to the study were excluded from the study.
Study Design
The patients to be included in the study were examined in terms of age, body mass index (BMI), mode of delivery, comorbidities, previous gynecological operations, urogynecological operations, pelvic organ prolapse, and presence of stress urinary incontinence. Preoperative evaluation included history, physical examination, stress test, 1-hour pad test, urine culture, 7-day voiding diary, residual urine measurement, and urodynamic examination. In postoperative evaluation, intraoperative and postoperative complications such as stress test, 1-hour pad weighing test, operation time, urinary tract infection, urination problems, de novo urgency symptoms, and urinary retention were taken into consideration. 1-hour pad test: After the pad, whose weight was measured with a Desis (model NHB) brand scale, was placed in the woman’s underwear, the woman was asked to drink 500 cc of water within 15 minutes. Walking and going up and down stairs in the following 30 minutes, and the last 15 minutes of 1 hour; He was told to squat and stand up 10 times, cough 10 times, run in place for 1 minute, pick up an object from the ground 5 times, and wash his hands with cold water for 1 minute. At the end of this period, the weight of the pad was measured and the difference with the initial pad weight was taken, and the result was interpreted according to the guide.
This amount was classified as mild if less than 2 grams, moderate if it was between 2-10 grams, severe if it was between 10-50 grams, and very severe if it was 50 grams or more [2]. Urodynamic tests were performed to detect patients with urge incontinence. In the stress test, it is observed whether urine escapes from the urethra by straining and coughing while the bladder is full. In our clinic, we perform this test when the bladder is filled with approximately 250 cc of liquid. In patients in whom urine leakage is not detected in the lithotomy position, the test must be repeated while standing. Additionally, if there is leakage, it is observed whether the leakage stops when the anterior vaginal wall is supported without obstructing the urethra (Marshall test). Continuation of urinary incontinence with this maneuver is a finding in favor of internal urethral sphincter defect (1-3).
Q Tip test allows us to objectively evaluate the effectiveness of the anatomical support of the tissues around the urethra and the degree of mobility of the bladder neck and proximal urethra. A cotton-tipped swab is pushed through the urethra into the bladder. Then the patient is forced to push. If the angle created in the horizontal plane by straining is >300, it is thought that the anatomical support of the bladder neck is reduced. The hypermobile urethra is mentioned [3, 4]. Patients diagnosed with pure stress incontinence were included in the study. Patients diagnosed with Mixed Type incontinence (Urge incontinence+stress incontinence) were treated and excluded from the study for study safety. Urodynamics was mainly performed to diagnose patients with Urge and Mixed incontinence. For study safety, patients diagnosed with pelvic organ prolapse that would require surgical repair were not included in the study. Postoperative patients were followed for 24 months. For follow-up, patients were called, and examinations were performed on the first 10th day after the operation, in the first 1 month, in the first 3 months, and thereafter at 6-month intervals for 2 years. In the Kaplan technique, which is a new technique, the surgery was performed under spinal anesthesia, in the dorsal lithotomy position, with a transvaginal incision. The patients who were operated on were not catheterized and underwent surgery after checking the presence of urine in the bladder via ultrasound. Before the procedure, to test the success of the procedure, the patient was made to cough and urine leakage was observed. In the Kaplan technique, which is a new technique, a 2-3 cm long incision is made vertically in the vagina, as if making an anterior colporrhaphy, by holding the urethra with an allis clamp, leaving a safe area of 1.5-2 cm.
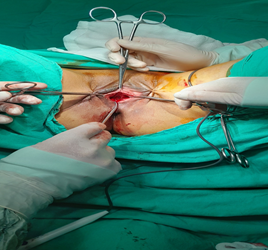
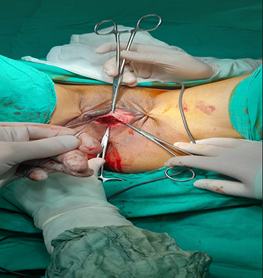
The tissues between the vagina and the bladder were dissected with sharp and blunt dissections to the right and left, towards the pubic bone, at 45o to the vertical incision. Dissection continued until the right and left pubic bones on both sides were found. After both pubic bones were located, both iliococcygeal muscle fascias were found and a 2/0 non-absorbable polyester suture was placed (Figure 1). The sutures were pulled with force before tying the knot under the vesicourethral junction, and a strength test was performed so that the patient could move. It was considered healthy when it was seen that there was no breakage, breakage in the sutures, or rupture in the tissue and the patient was moving. For the sutures that broke off from the tissue during the durability test, it was assumed that the iliococcygeal muscle fascia did not pass through and suturing was performed again. Both polyester sutures that passed the durability test were tightly tied together to act as a hammock under the urethra and bladder junction. After the procedure, the patient was made to cough again and when it was observed that there was no urine leakage, the operation was considered successful. When it was observed that there was no urine leakage after the procedure, a 14- 16 French catheter was inserted to ensure that the urethra was not narrowed thoroughly. The operations of the patients whose catheter was easily inserted were terminated, but the patients who encountered resistance while inserting the catheter were re-sutured. Finally, the vaginal vertical incision was sutured with continuous primary suturing with 2/0 absorbable polyglactin and the operation was terminated. The objective cure was determined by stress testing and pad testing. Patients with negative stress tests and 24-hour pad tests (<10g/24 hours) were considered cured. Patients with a decrease of more than 50% in the pad test were considered to have improved. Results other than this were considered unsuccessful, even if there was an improvement compared to the preoperative situation. Images of the surgery are given in Figure 1 & Figure 2. Patients were monitored for postoperative retention, frequent urination, feelings of urgency, pain, and dyspareunia. Possible complications were recorded.
Statistical Analysis
SPSS (IBM SPSS for Windows, Ver.26) statistical package program was used for the statistical analysis of our study. For comparison of patients’ general characteristics, the χ2 test or Fisher’s exact test was used for categorical variables and the Mann-Whitney U test for continuous variables. Statistical significance was considered P <0.05. Bonferroni correction was used where necessary to adjust for multiple comparisons.
Ethics Committee Approval
Permission for our research was received from the Clinical Research Ethics Committee of Uşak University Faculty of Medicine, Date: 08.06.2023, Decision No: 125- 125-02. Necessary informed consent was obtained from the patients included in the study. Our study was conducted according to the principles stated in the Declaration of Helsinki.
Results
The age range of the patients included in the study varies between 26 and 74 years. The average age is 46.19 years. The duration of stress incontinence in patients varies between 2-15 years. The average duration of stress incontinence was found to be 6.85 years. General characteristics of the patients are given in Table 1.
Incontinence was observed in 6 patients after the operation. Complete cure was achieved in 294 of the patients and it was found to be statistically significant (p=0.000). The success rate of the method was found to be 98% in our study. The changes in the stress test and Q-type test results before and after the operation were found to be statistically significant (p=0.000). The changes detected in the postoperative pad test were found to be statistically significant (p=0.004). No intraoperative complications related to the operation were observed. Urinary retention was observed in 12 patients after the operation. Frequent urination, feelings of urgency, pain, and dyspareunia were not observed. Postoperative findings are given in Table 2.
| Age (Years) | Minimum- Maximum | Mean(N) |
|---|---|---|
| 26-74 | 46.19 | |
| BMI | 21-35 | 26.16 |
| Birth Number | 02-Jun | 3.12 |
| Incontinence Duration (Years) | Feb-15 | 6.85 |
| Pad Test (Gram) | 45-150 | 67.53 |
| Menopause | Yes | 102 |
| No | 198 | |
| Total | 300 | |
| Stress Test | Positive | 300 |
| Negative | 0 | |
| Total | 300 | |
| Q Tip Test | Positive | 300 |
| Negative | 0 | |
| Total | 300 | |
| Mode of Deliveries | Number (N) | Percent (%) |
| 181 | ||
| 119 | ||
| Previous Operation Gynecologic | Number (N) | Percent (%) |
| 35 | 11.7 | |
| 48 | 16 | |
| 37 | 12.3 | |
| 58 | 19.4 | |
| 122 | 40.6 | |
| 300 | 100 | |
| Previous Operations Ürogynecologic | Number (N) | Percent (%) |
| 0 | 0 | |
| 300 | 100 | |
| Pelvic Organ Prolapse Evaluation | Number (N) | Percent (%) |
| 0 | 0 | |
| 100 | 100 |
Table 1: General Characteristics.
BMI: Body Mass Index, CS: Sezaryan Doğum, VD: Vajinal Doğum. Table 1: General Characteristics.
| Number (N) | Percent (%) | p | ||
|---|---|---|---|---|
| Complication | Urinary Retention | 12 | 4 | 0.000* |
| Frequent Ürination | 0 | 0 | ||
| Sensation of Urgent Urination | 0 | 0 | ||
| Pain and Dyspareunia | 0 | 0 | ||
| Total | 12 | 4 | ||
| İncontinence | Yes | 6 | 6 | 0.000* |
| No | 294 | 294 | ||
| Total | 300 | 300 | ||
| Stress Test | Positive | 6 | 6 | 0.000* |
| Negative | 294 | 294 | ||
| Total | 300 | 300 | ||
| Q Tip Test | Positive | 6 | 6 | 0.000* |
| Negative | 294 | 294 | ||
| Total | 300 | 300 | ||
| Pad Test (Gram) | Minimum | 0 | 0.004* | |
| Maximum | 30 | |||
| Mean | 1.24 |
Table 2: Postoperative Findings.
*A value of P<0.05 was considered significant within the 95% confidence interval. Table 2: Postoperative Findings.
Discussion
Urinary incontinence is an important sociocultural health problem with a high prevalence. Considering that quality of life is becoming increasingly important and average life expectancy is increasing, SUI treatment will become even more valuable in the coming years as the number of geriatric individuals increases [5].
Today, mid-urethral slings (MUS) are considered the gold standard in the treatment of SUI [5]. This notion is supported by a large population-based cohort analysis by the National Health Service in England, which demonstrated a low removal rate of 3.3% and a low failure rate of 4.5% after 9 years of follow-up in more than 90,000 women receiving MUS [6].
However, controversy has arisen regarding complications associated with surgical incontinence procedures, leading to several court cases against the use of vaginal slings and tapes in the United States, Canada, the United Kingdom, and some European countries [7, 8].
For this reason, minimally invasive surgeries that do not use mesh have an important place. Again, mid-urethral slings can be made from the vagina without the use of minimal mesh, which is a great convenience for the patient and the physician. Our study is completely vaginal and minimally invasive. In addition, not using mesh is a great advantage for the patient and the surgeon.
More than 25 years ago, Ulmsten et al. A new type of surgery for stress urinary incontinence in women was introduced. It revolutionized the surgical treatment of stress incontinence. A tension-free alloplastic sling (preferably made of polypropylene) implanted under the middle third of the urethra and removed behind the pubic bone stabilizes the pubourethral ligaments and suburethral fascial structures [9, 10].
In our method, there is a surgery that works with the same logic but does not use mesh. Therefore, mesh-related complications are prevented. As for effectiveness, Ulmsten et al. While the success rate in the method he described was 78%, it was found to be 98% in our method [9, 10].
The support of the urethra depends on its fascial connection to the pelvis of the tendinous fascia arch and its connective tissue connection to the pubis [11]. It should be remembered that tension-free tapes and colposuspension target urethral hypermobility, while bulking agents, autologous fascia straps, and artificial sphincter muscles focus on intrinsic sphincter insufficiency [12].
The potential of laser therapy cannot be evaluated with certainty at this time. This technique needs further study [13].
For several decades, transvaginal tension-free tapes (TVT) have become an established treatment for female SUI. Comparable results were observed between colposuspension and TVT implantation [14].
However, transvaginal access causes side effects that affect sexuality, and implantation of nonabsorbable slings or MESH may cause complications due to material stiffness or tissue erosion. That’s why the US Food and Drug Administration (FDA) has issued a warning. This led to a change in surgical strategies for women and led to a revival of classical surgical techniques such as colposuspension [15, 16].
Our study is designed to recreate anatomical support without using MESH. Additionally, it does not cause sexual activity problems in patients. Patients can return to their social lives earlier.
Tension-free vaginal tape (TVT), one of the most widely used methods in the surgical treatment of stress urinary incontinence in women, was developed in 1990 by Ulmsten and Petros within the scope of integral theory. The cure rate of TVT operation has been reported between 66% and 91% [17, 18].
In our study, our cure rate was found to be 98%. A high cure rate was found compared to the methods in the literature. As it was observed that the perioperative complications of TVT (bladder perforation, bowel, and major vascular injuries) were mostly due to penetration into the retropubic space, the need to develop alternative techniques to TVT arose. The Transobturator technique, developed by Delorme in 2001 to reduce morbidity, has advantages such as avoiding the Retzius area and working in limited proximity to the peritoneal cavity [19].
In our study, urinary retention was observed in 12 patients. Since our follow-up period was 2 years, we may not have been able to detect long-term complications.
The needleless technique, one of the newest methods used in the surgical treatment of stress urinary incontinence, is a minimally invasive mid-urethral sling surgery that uses a polypropylene mesh and does not require the use of any needles or guides. Preserving the tension-free concept with the needleless technique is aimed at avoiding major complications that may occur during the passage of the needles used in sling surgeries. In surgeries such as TVT and TOT, bladder rupture, obturator nerve damage or vascular injuries may occur during the needle’s passage through the trans-obturator route. Needleless is a new method developed to reduce these possible complications [20].
Not entering the Retzius space and the pelvic cavity are two important advantages of the procedure. This is why no complications were observed in our study. 80-90% of women who undergo retropubic or transobturator sling procedures improve or are treated for their stress incontinence symptoms after surgery. Single-incision sling procedures are relatively new and success rates are still being monitored [20]. The success rate of our study was found to be 98%. However, multicenter studies with a larger patient population are needed. A 63-97% subjective and 59-100% objective cure rate has been reported for Burch colposuspension [21, 22, 23]. A subjective cure rate of 72-100% and an objective cure rate of 71-100% have been reported for the Marshall- Marchetti-Kranz operation [24, 25, 26, 27]. Subjective success rates of 50-97% and objective success rates of 40-93% have been reported for needle suspension surgeries [28, 29, 30, 31]. Subjective success rates of 60-100% and objective success rates of 78- 100% have been reported for sling operations [32, 33, 34]. The general subjective success rate of periurethral injections varies between 30-95% and the objective success rate varies between 31-70% [35, 36, 37, 38].
High success rates are achieved with appropriate methods in the treatment of SUI that have been correctly diagnosed with current methods. However, there is still some confusion in evaluating the results of surgical interventions for SUI. Some researchers use terms such as “improvement” when giving their results, but the definition of this improvement is different for each researcher. Moreover, when talking about the success of the operation, is the most important criterion to be based on the objective success rate determined by physical examination and urodynamic tests? Is it the subjective success rate determined by the patient’s statement? Or is it the patient’s satisfaction with the postoperative continence status? There is no consensus that it is. In our study, the cure rate was determined based on objective data.
Conclusion
Our study aimed to draw attention to an effective method in the treatment of SUI. The success rate of our study is quite high compared to the literature. The absence of complications during and after the operation is very advantageous for this method. We think that our study will contribute to the literature.
References
-
Grother CW, Shaw C, Perry SI, Dallosso SM, Mensah FK (2001) Epidemiology (Europe). In: Cardozo L, Staskin D (Eds.), Textbook of Female Urology and Urogynaecology, Isis Medical Media Oxford pp: 21-35.
-
Dmochowski RR, Blaivas JM, Gormley EA, Juma S, Karram MM, et al. (2010) Female Stress Urinary Incontinence Update Panel of the American Urological Association Education and Research, Inc; Whetter LE. Update of AUA guideline on the surgical management of female stress urinary incontinence. J Urol 183(5):1906-1914.
-
Tanagho EA (1976) Colpocystourethropexy: the way we do it. J Urol 116(6): 751-753.
-
Riggs JA (1986) A review of two operative procedures with long-term follow-up. Obstet Gynecol 68(1): 98-105.
-
Zacche MM, Mukhopadhyay S, Giarenis I (2019) Changing surgical trends for female stress urinary incontinence in England. International urogynecology journal 30(2): 203-209.
-
Gurol-Urganci I, Geary RS, Mamza JB, Duckett J, El- Hamamsy D, et al. (2018) Long-term Rate of Mesh Sling Removal Following Midurethral Mesh Sling Insertion Among Women With Stress Urinary Incontinence. JAMA 320(16): 1659-1669.
-
Dyer O (2016) Johnson and Johnson face a lawsuit over vaginal mesh devices. BMJ 353: i3045.
-
Keltie K, Elneil S, Monga A, Patrick H, Powell J, et al. (2017) Stres üriner inkontinans için vajinal mesh prosedürlerini takip eden komplikasyonlar: 92.246 kadın üzerinde 8 yıllık bir çalışma. Bilimsel raporlar 7(1): 12015.
-
Ulmsten U, Johnson P, Petros P (1994) Intravaginal slingplasty. Zentralblatt fur Gynakologie 116(7): 398- 404.
-
Ulmsten U, Petros P (1995) Intravaginal slingplasty (IVS): an ambulatory surgical procedure for the treatment of female urinary incontinence. Scandinavian journal of urology and nephrology 29(1): 75-82.
-
DeLancey JO (1988) Structural aspects of the extrinsic continence mechanism. Obstet Gynecol 72(3Pt1): 296- 301.
-
Hofmann R, Wagner U (2014) Inkontinenz- und Deszensuschirurgie der Frau. In: 2nd (Edn.), Springer; Heidelberg, Germany.
-
Pergialiotis V, Prodromidou A, Perrea DN, Doumouchtsis SK (2017) A systematic review on vaginal laser therapy for treating stress urinary incontinence: Do we have enough evidence?. Int Urogynecol J 28: 1445-1451.
-
Ward KL, Hilton P (2004) UK and Ireland TVT Trial Group. A prospective multicenter randomized trial of tension-free vaginal tape and colposuspension for primary urodynamic stress incontinence: two-year follow-up. Am J Obstet Gynecol 190(2): 324-331.
-
Deng DY, Rutman M, Raz S, Rodriguez LV (2007) Presentation and management of major complications of mid-urethral slings: Are complications under-reported? Neurourol Urodyn 26(1): 46-52.
-
FDA (2011) UPDATE on Serious Complications Associated with Transvaginal Placement of Surgical Mesh for Pelvic Organ Prolapse: FDA Safety Communication.
-
Petros PE, Ulmsten UI (1990) An integral theory of female urinary incontinence. Experimental and clinical considerations. Acta Obstet Gynecol Scand Suppl 153: 7-31.
-
Sharifi-Aghdas F (2005) Surgical management of stress urinary incontinence. Urol J 2(4): 175-182.
-
Delorme E (2001) Transobturator urethral suspension: mini-invasive procedure in the treatment of stress urinary incontinence in women. Prog Urol 11(6): 1306- 1313.
-
Navazo R, Moreno J, Hidalgo C, Herraiz MA, Vidart JA, et al. (2009) Contasure Needleless: a single incision tot for the surgical treatment of stress urinary incontinence. Arch Esp Urol 62(9): 719-723.
-
Shull BL, Baden WF (1989) A six-year experience with paravaginal defect repair for stress urinary incontinence. Am J Obstet Gynecol 160: 1432-1440.
-
Sand PK, Bowen LW, Ostergard DR (1988) The effect of retropubic urethropexy on detrusor stability. Obstet Gynecol 71: 818-822.
-
Bergman A, Coonings PP, Ballard CA (1989) Primary stress urinary incontinence and pelvic relaxation: prospective randomized trial comparison of three different operations. Am J Obstet Gynecol 161(1): 97- 101.
-
Park GS, Miller EJ (1988) Surgical treatment of stress urinary incontinence: a comparison of Kelly plication, Marshall-Marchetti-Kranz, and Pereyra procedures. Obstet Gyencol 71(4): 575-579.
-
Kish RH (1979) The Kish urethral illuminating catheter. J Urol 121: 43-44.
-
Milani R, Scalambrino S, Quadri G (1985) Marshall- Marchetti-Kranz procedure and Burch colposuspension in the surgical treatment of female urinary incontinence. Br J Obstet Gynecol 92: 1050-1053.
-
Henriksson L, Ulmsten U (1978) Urodynamic evaluation of the effects of abdominal urethrocystopexy and vaginal sling urethroplasty in women with stress incontinence. Am J Obstet Gynecol 131(1): 77-82.
-
Shah PJR, Holder PD (1989) Comparison of Stamey and Pereyra-Raz bladder neck suspensions. Br J Urol 64(5): 481-484.
-
Roberts JA, Angel JR, Thomas R (1981) Modified Pereyra procedure for stress incontinence. J Urol 125(6): 787- 789.
-
Mundy AR (1983) A trial comparing the Stamey bladder neck suspension with a colposuspension for the treatment of stress incontinence. Br J Urol 55(6): 687-
-
Stamey TA, Schaeffer AJ, Condy M (1975) Clinical and roentgenographic evaluation of endoscopic suspension in the vesical neck for urinary incontinence. Surg Gynecol Obstet 140: 355-360.
-
Henriksson L, Ulmsten U (1978) Urodynamic evaluation of the effects of abdominal urethrocystopexy and vaginal sling urethroplasty in women with stress incontinence. Am J Obstet Gynecol 131(1): 77-82.
-
Kersey J (1983) The gauze hammock sling operation in the treatment of stress incontinence. Br J Obstet Gynecol 37: 213-219.
-
Jarvis GJ, Fowlie A (1985) Clinical and urodynamic assessment of the porcine dermis in the treatment of genuine stress incontinence. Br J Obstet Gynecol 92(11): 1189-1191.
-
Lil KB, Bal AJ, Fenelet RCL (1983) Periurethral teflon injection. Br J Urol 55: 208-210.
-
Appel Ra, Rice JD (1998) Periurethral polyteflon injection for urinary incontinence in women. J Urol 139: 270A.
-
Kieswetter H, Fischer M, Wober L, Flamm J (1992) Endoscopic implantation of collagen for the treatment urinary incontinence. Br J Urol 69: 22-25.
-
Schulman CC, Simon J, Wespes E, Germau F (1984) Endoscopic injection of Teflon to treat urinary incontinence in women. Br Med J 288(6412): 192-194.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era