Strategic Assessment of Rational Drugs use in Tertiary Care Hospital Peshawar, Pakistan
Background: Rational drugs are safe, effective and medico-socio-economical for the patients. The rational use of drugs required to achieve the optimal state of the patient by community affordable cost, the “WHO†indicator for rational drug use is consists of three indicators includes prescription indicator, patient care indicator and facility indicator. Methods: The study carried out in Tertiary care hospital in order to assess the WHO†indicators include Prescription indicator, patient care indicator and facility indicator. Results: The concurrent quantitative study of 202 patients carried out in Tertiary Care Hospital in which 111 (54.9%) were male and 91 (45.1%) were female. The (WHO) facility indicator utilized for patient drugs use, which is consists of 3 main indicators in which first indicator is about the prescriber indicator in which slight deviations found in which average number of drugs prescription was 5.1 (S.D 3.3), drugs with generic name in percent per encounter were 4 (0.38%) in which (S.D 99.62%), antibiotics and injectables were respectively (18.7%), (34.6%) and drugs from EDL were (81.8%), second indicator is patient care indicator which also deviates includes total time for consultation which was 5 minutes (S.D 25 min), second is about total dispensing time was 50 seconds (S.D 10 seconds), third is about percent of drugs proper dispensed was 71% (S.D 29%) and percent of patients discharged with proper knowledge regarding the drugs doses was 48% (S.D 52%) and the third one is facility indicator which is completely followed, while the rest of two slightly deviates, thus it should be followed completely to achieve the rational use of drugs in order to achieve optimal therapeutic outcomes. Conclusion: The current study concluded that the “WHO†indicators are the standard for rational use of drugs these should be utilized in every health care facility in order to achieve optimal patient therapeutic outcomes.
Introduction
According to “World Health Organization” Rational drug use means “Patients receive medications appropriate to their clinical needs, in doses that meet their own individual requirements, for an adequate period of time, and at the lowest cost to them and their community” [1]. The Australian Health Ministry defined the rational drugs use in 6 rights which includes right drug for right patient in right dose at right route in right time with right documentation [2, 3].
The rational drugs are quintessential for patient because they are medico-socio-economical [4]. Medication errors are the third leading cause of death in United State than cancer and cardiac diseases [5]. It is documented that worldwide the 50% of population unable to take correct drugs and half of the drugs prescribed and dispensed inappropriately. For these errors reduction and enhancement of rational drugs use the World Health Organization generated the guidelines [3] includes:
Prescription Indicator
- Average drugs per encounter
- Percent drugs with generic names
- Percent antibiotics per encounter
- Percent injections per encounter
- Percent drugs from EDL
Patient Care Indicator
- Total consultation time
- Total dispensing time
- Percent drugs proper dispensed
- Percent patients correct knowledge about doses
Facility Indicator
- Availability of EDL/ formulary [6].
- In developed countries these guidelines for rational use of drugs regularly conducted [7]. The reciprocal of rational is irrational use, the irrational practice not only rises the financial budget of the health care but also aggravate the challenges for emergence of bacterial resistance [8], inappropriate therapy and adverse effects [9]. This study conducted in Tertiary Care Hospital Peshawar, Pakistan. To utilize this guideline in order to achieve the rational drugs use.
Materials and Methods
Study Design and Setting
The two months concurrent quantitative study of 202 patients carried out in Tertiary Care Hospital Peshawar, Pakistan.
Inclusion and Exclusion Criteria
All of the patients included in this study randomly those patients excluded includes:
- OPD patients
- Patients on monotherapy
- Incomplete prescription detail of the patients.
Data collection and Sample Size
The total of 202 patients case histories analyzed, the “World Health Organization in 1985 in Nairobi, Kenya” recommended thirty prescriptions per facility for sampling” in this study the data collected from January to February 2019. The data collected prior to official permission from director of the Hospital and Pharmacy Manager. The data collectors educated and guided ethically and socially from university prior to data collection.
Data Analysis
After collection the data analyzed via “Microsoft Excel 2007 version” and “Graph Pad Prism 5” (x86) for graphical presentation and tabulation of the data, and the data collected by “World Health Organization” indicator on the name “How to Investigate drug use in health facilities 1993” as shown in the Table 1.
| Indicator | Obtained Result | Ideal Value | Standard Deviations |
|---|---|---|---|
| Prescriber Indicator | |||
| Average drugs per encounter | 5.1 | 1.6-1.8 | 3.3 |
| % drugs with generic names | 4 (0.38%) | 100% | 99.62% |
| % antibiotics per encounter | 18.70% | 20-26% | 7.30% |
| % injections per encounter | 34.60% | 13-24% | -10.60% |
| % drugs from EDL | 81.80% | 100% [10] | 18.20% |
| Patient Care Indicator | |||
| Total consultation time | 5 min | 30 min | 25 min |
| Total dispensing time | 50 sec | 60 sec | 10 sec |
| % drugs proper dispensed | 71% | 100% | 29% |
| % patients correct knowledge about doses | 48% | 100% | 52% |
| Facility Indicator | |||
| Availability of EDL/ formulary | Yes | Yes/No | 00 [6, 9] |
Table 1: “WHO” rational drugs use indicator. *EDL = Essential drug list.
Ethical Approval and Consent Format
This study carried out in Tertiary Care Hospital on permission of official hospital authorities, on the completion of clerkship data the Hospital Director and Manager Pharmacy department issued the certificates, the patient consent was also made on “Helsinki Principles for ethics followed by the author” [11].
Results
The two months study includes 202 patients in which 111 (54.9%) were male and 91 (45.1%) were female, which is graphically presented in Figure 1.
Prescription Indicator
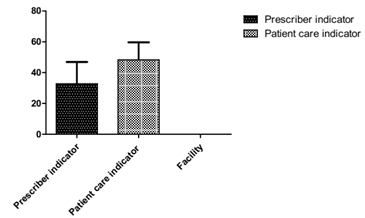
The average number of drugs per prescription was 5.1 (S.D 3.3). The drugs with generic name in percent per encounter were 4 (0.38%) in which (S.D 99.62%). The antibiotics and injectable were respectively (18.7%), (34.6%) and drugs from EDL were (81.8%) as shown in the Table 1 & Figure 2.
Patient Care Indicator
The “World Health Organization” have kept the standard for patient care in which first portion is total time for consultation which was 5 minutes (S.D 25 min), second is about total dispensing time was 50 seconds (S.D 10 seconds), third is about percent of drugs proper dispensed was 71% (S.D 29%) and percent of patients discharged with proper knowledge regarding the drugs doses was 48% (S.D 52%) and detail is given in Table 1 & Figure 2.
Facility Indicator
This indicator includes the availability of Formulary or “EDL” that was present and indicate in the form of “yes” as shown in the Table 1 & Figure 2.
Discussion
According to “WHO” the ideal number of drugs per encounter is 1.6-1.8 [6, 12], similar studies carried out in Iran where the 3.5 drugs [13] and in Pakistan 7.05 drugs per encounter by Hussain [3] and in Karachi found 4.5 drugs per encounter in 2001 [14] in a similar way our study purports 5.1 drug per encounter that is lesser than Pakistan and higher than “WHO” and Iran [13], this high proportion of drugs in prescription purports Polypharmacy (use of many medications per encounter than the standard recommended limit or unnecessary drugs than requirement) [15, 16]. The “WHO” documented that all of the drugs should be prescribed on generic name, on this indictor the Hussain et al conducted the study in 2017 in Pakistan in which they do not found any drug on generic name [3] and Aqeel, et al. in Pakistan in four facilities in which lower range was 4.81% and higher was 39.5% [9] in a similar way in our study the generic drugs per encounter were 0.38% which is higher than Hussain et al but lesser than Aqeel, et al. The “World Health Organization” documented that percent of antibiotics will be (20-26%), injectables will be (13-24%) and drugs from “EDL” will be 100%, similar type of study carried out by Hussain et al regarding antibiotics were (17.1%), Aqeel study indicates lower limit (6.6% and higher limit was 90%) in a similar way in our study antibiotics were in range 18.7%, injectables were (49.93%) in Hussain et al study, in Aqeel et al (16.6% was lower limit and 90% was higher), in Tanzania (19%) [17] while in India (3.9%) [18], no drugs in Hussain et al and Aqeel, et al. from “EDL” in our study 81.8% drugs prescribed from “EDL” that is much higher ratio.
The patient care indicator is standard recommended by “WHO” mention in Table 1. In a similar way the study conducted by Aqeel et al in Pakistan in 2016, in which higher consultation time was 6.5 minutes and lower was 2.1 in a similar way in our study this time was 5 minutes and deviates 25 minutes from standard. The dispensing time recommended by “WHO” is 60 seconds similar type of study conducted by this indicator by Aqeel et al in which higher range was 57.5 seconds and lower range was 47.8 seconds in a similar way in our study this time was 50 seconds.
The “WHO” recommended that all the drugs should be properly dispensed and proper knowledge regarding the drugs doses, this indicator utilized by Aqeel et al in four facilities in which they found lower range 50% and higher range 84.6% in term of proper dispensed and regarding proper knowledge the lower range was 16.6% and higher range was 100% in a similar way in our study 48% patients got knowledge regarding the doses. The “WHO” recommended that the Essential drug lists should be available in all facilities, similar type of studies conducted by Aqeel et al in Pakistan in four facilities in which EDL was available with 3 out of 4 [9, 19] in a similar way in our study the indicator was available.
Conclusion
The “World Health Organization” standard is utilized for rational drugs use in developed countries. Prescription is the key component and is written order by Physician to dispensing Pharmacist to dispense medications, then dispensing starts, after that the dispensed products administered into the patient, if the prescription write wrong the whole pathway will be going wrong ultimately the wrong medications will reach to the patients and will loss of patient therapeutic outcome. The result of this two months study of 202 patients indicates that the (WHO) indicators in Tertiary Care Hospital were not up to the mark to improve the overall health status of the patients and rational use of medications. The use of these indicators can effectively decrease the irrationality and increase the rational use of drugs in specific facility.
Conflict of Interest
Nil
Acknowledgement
None
Limitations
This study was limited to only one Tertiary Care Hospital, the study may conduct in various hospitals in order to improve the overall health status and rational use of drugs.
Recommendations
The authors recommended the “WHO indicators and EDLs” for patient therapy as well as for reduction of the burden from the shoulders of Physicians appoint the competent clinical experts mean Clinical Pharmacists, these two steps will effectively decrease irrationality and will improve rational use of drugs.
References
-
(2002) WHO, Promoting rational use of medicines: core components, World Health Organization Geneva.
-
(2002) Australia, The six rights of safe medication administration, Government of Western Australia Department of Health.
-
Hussain H, Kifayatullah SK, Ahmad S, Khan A, Ullah A (2017) Assessment of prescription pattern and prescription errors using the World Health Organization drug use indicators in Lady Reading Hospital Peshawar. Pakistan: a retrospective study. Khyber Med Univ J 9(4): 181-184.
-
Singhal KC (2007) Pharmacology laboratory manual, Pharmacy and Clinical Pharmacology, 2nd (Edn.), CBS publishers and distributors 2: 6-7.
-
Makary MA, Daniel M (2016) Medical error the third leading cause of death in US. BMJ, pp: 1-5.
-
WHO (1993) How to invistigate drug use in health facilities, selected drugs use indicators, s2289e.
-
Austvoll-Dahlgren A, Aaserud M, Vist G, Ramsay C, Oxman AD, et al. (2008) Pharmaceutical Policies: effects of cap and co-payment on rational drug use. Cochrane Database system Rev 23(1).
-
Ahmad A, Khan MU, Patel I, Maharaj S, Pandey S, et al. (2015) Knowledge attitude and practice of B.Sc Pharmacy studetns about in Tridad and Tebago. J Res Pharm Pract 4(1): 37-41.
-
Aslam A, Khatoon S, Mehdi M, Mumtaz S, Murtaza B (2016) Evaluation of Rational Drug Use at Teaching Hospitals in Punjab, Pakistan. Journal of Pharmacy Practice and Community Medicine 2(2): 54-57.
-
Sunny D, Roy K, Benny SS, Mathew DC, Naik JG, et al. (2019) Prescription Audit in an Outpatient Pharmacy of a Tertiary Care Teaching Hospital-A Prospective Study. J Young Pharm 11(4): 417-420.
-
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, et al. (2015) Empagliflozin, Cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 373(22): 2117-2128.
-
Joshi MP, Sugimoto T, Santoso B (1997) Geriatric Prescribing in the Medical Wards of a Teaching Hospital in Nepal. Pharmacoepidemiology Drug Safety 6(6): 417- 421.
-
Cheraghali AM, Nikfar S, Behmanesh Y, Rahimi V, Habibipour F, et al. (2004) Evaluation of availability, accessibility and prescribing patterrn of medicines in the Islamic Republic of Iran. East Mediterr Journal 10(3): 406-415.
-
Das N, Khan AN, Badini ZA, Baloch H, Parkash J (2001) Prescribing practices of consultants at Karachi, Pakistan. J. Pak Med Assoc 5(2): 74-77.
-
Hajjar ER, Cafiero AC, Hanlon JT (2007) Polypharmacy in elderly patients. Am J Gariatric Pharmacotherpy 5(4): 345-351.
-
Schuler J, Duckelmann C, Beindl W, Prinz E, Michalski T, et al. (2008) Polypharmacy, inappropriate prescribing and adverse drugs in Austria. Wien Klin Wochenschr 120(23): 713-714.
-
Massele AY, Nsimba SE, Rimoy G (2001) Prescribing habits in church-owned primary health care facilities in Dar ES Salaam and other Tanzanian Coast regions. East Afr med J 78(10): 510-514.
-
Hazra A, Tripathi SK, Alam MS (2000) Prescribing dispensing activities at the health facilities of a non- government organization. Nat Med J India 13(4): 177- 182.
-
Anker M, Fresele D, Hozerzil H (1993) How to investigate drug use in Health facilities WHO/DAP.
- Evaluation of Skin Aging Preventive Effects of Cherry Blossom Petal Extracts Through Antioxidant and Anti-Glycation Activities
- Is Cell Death Responsible for False Positive Results of In Vivo Comet Assay?
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism