The Long-Term Effects of Eccentric Exercise Vs. Extracorporeal Shockwave Therapy in Athletes Aged 18-50 with Lower Extremity Tendinopathy: A Meta-Analysis and Systematic Review
Background: Establishing the most effective treatments for patellar tendinopathy (PaT) is critical because of its high prevalence in as an orthopedic condition, particularly in jumping athletes. Two increasingly popular and researched therapy interventions are extracorporeal shockwave therapy (ESWT) and eccentric exercise (EE). Yet it has not been established how the two compare to each other. Objective: The purpose of this study was to compare via meta-analysis the long-term effects of EE on both pain and function to those of ESWT in athletes with PaT and to also compare with a systematic review the same PICO components with the addition of Achilles Tendonopathy (AT). Data Sources: Search procedures followed PRISA guidelines using the PubMed, CINAHL, and Cochrane Library databases. Study Selection: Athletes ages 18-50 years, PaT for >3 months, EE, ESWT, Visual Analog Scale (VAS) measuring pain, Victorian Institute of Sport Australia – Patella (VISA-P) measuring function. Results: A fixed effects model was used to compare the interventions. Eccentric Exercise was found to have very large effect sizes of 2.363 (1.075, 3.651) and 18.790 (8.604, 28.977) for improving pain and function respectively when compared with extracorporeal shockwave therapy. Conclusion: Eccentric exercise is the treatment of choice for athletes with patellar tendinopathy, while extracorporeal shockwave therapy is a viable secondary option for patients that fail to respond to eccentrics alone.
Introduction
Tendinopathies are among the most prevalent type of overuse injuries to occur in sports. [1]. Common sites for tendinopathy include the Achilles tendon (AT), extensor tendon of the forearm, rotator cuff tendon, and patellar tendon [2]. Patellar Tendinopathy (PaT) is a prevalent orthopedic condition for recreational and elite athletes [3]. Athlete overall prevalence of PaT is 14.2% [4, 5] and is particularly high in jumping sports such as basketball, volleyball, and soccer, which involve excessive running, jumping, and directional changes [5, 6]. Prevalence rates for tendinopathies as a whole are as high 45% in some sports [5]. Patellar tendinopathy leads to impairment of functional activities such as stairs, squats, stand to sit, and prolonged siting7 and it can impact an athlete as much as an acute knee injury [5].
Causative factors for the condition are hard playing surfaces, high frequency of training sessions with repetitive eccentric movement, and decreased hamstring and quadriceps flexibility [6, 7, 8, 9]. Additional proposed risk factors include: increased weight, increased BMI, increased waist-to-hip ratio, leg-length discrepancy, lower arch height of the foot, and decreased quadriceps strength [10]. Patellar tendinopathy is commonly characterized by chronic load-dependent pain at the inferior pole created by fibril degeneration and mechanical failure [3].
There are 2 types of PaT, reactive (RPaT) and degenerative patellar tendinopathy (DPaT). Neither involve an inflammatory process. However, RPaT, is the patellar tendon’s response to a rapid increase in loading or training frequency with swelling and subsequent pain, and it can progress to DPaT [11].
Degenerative patellar tendinopathy occurs over several months and the structure becomes tangled and disorganized, leading to advanced matrix breakdown and increased risk of rupture [11, 12]. Mucoid degeneration is a loss of structural integrity within the tendon in which healthy tissue is replaced by gelatinous mucoid ground substance [13]. In addition, fibrocartilaginous metaplasia takes place [14, 15, 16].
Another feature seen in DPaT is an increased amount of fibroblasts, which leads to increased cellularity [14, 15].
The new cells do not lay down as tight parallel collagen bundles, but are separated by the increased amounts of mucoid ground substance. Collagen appears disorganized and discontinuous, which leads to the tendon becoming less capable of absorbing and transducing forces [12, 17]. Theories suggest that mechanical and biochemical factors play a role in the pain that is created. Tendon degeneration involving mechanical collagen breakdown and chemical irritants such as lactate, glutamate, and substance P have all been identified as potential causes of pain [18, 19].
Because of multifactorial etiology and lack of quality longitudinal studies on treatment effect, patellar tendinopathy is poorly understood [10] and therefore there is no consensus on the best conservative treatment approach [7, 20]. Current conservative interventions include: eccentric exercise (EE), soft tissue mobilization, manual therapy, range of motion, and modalities. A recent clinical review recommended EE, STM, strengthening of the hip musculature, and stretching throughout the course of PaT [21]. The most popular nonoperative treatment for PaT is EE [22].
Eccentric Exercise for Patellar Tendinopathy
The exact effect of EE on tendinopathies is not completely understood, however, evidence support both increased rate of collagen synthesis and improved tendon microcirculation [23, 24, 25, 26]. Studies however do not propose an optimal duration and frequency of exercise, or whether drop squats verses slow eccentric movement, use of a decline board, or exercising into pain, should be incorporated [22]. A systematic review reported that 5 of 7 EE studies, reported significant improvement and concluded that EE training appears to be the treatment of choice [24, 25]. Some evidence also indicates that the Alfredson model for EE training many be optimal [27, 28, 29, 30, 31, 32, 33].
Extracorporeal Shockwave Therapy for Patellar Tendinopathy
Recently, extracorporeal shockwave therapy (ESWT) is a treatment option for lower limb tendinopathies that is growing in popularity and studies show approximately a 90% success rate in the treatment of shoulder, elbow, and heel tendinopathies, with only a 5-7% recurrence rate [34, 35, 36, 37, 38, 39, 40, 41, 42]. There is also a trend toward success with PaT where EE has failed [43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54]. Shockwaves are rapid, short and distinct single fluctuations of acoustic energy that propagate quickly through a medium [35, 47] and attenuation of the shockwave is highly dependent on the medium type [35].
Several different mechanisms of action on tendinous tissue are described including direct stimulation of healing, neovascularization, direct suppressive effects on nociceptors, and a hyperstimulation effect that blocks the gate-control mechanism [54, 55, 56, 57, 58, 59, 60]. ESWT causes fibrinoid necrosis, paratenon fibrosis, inflammatory cell infiltration [48], and impaired tensile strength in tendons [36] and it can elicit release of growth factors and other active substances [38] which increase the number of neovessels at the normal tendon-bone junction [37]. However, similar to EE there is not a consensus on optimal treatment parameters or use of anesthesia [34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49].
Purpose
The purpose of this meta-analysis and systematic review was to determine the long-term effects of EE on pain and function compared to ESWT in athletes aged 18- 50 with PaT. The systematic review was extended to the additional lower extremity tendinopathy of AT because of its similar prevalence. It is hypothesized that EE will result in a significant difference, in reducing pain and improving function in athletes with PaT, compared to ESWT. The purpose of the systematic review was to define qualitatively, via PICO parameters, which treatment (ESWT or EE) was more supported for LE tendonopathy.
Methods
Search Strategy
The study design and protocol were in accordance with the Systematic Reviews and Meta-Analysis (PRISMA) guidelines [50]. A systematic review was conducted by one reviewer from September 2016 to October 2016 in PubMed, CINAHL, and Cochrane Library databases and reference lists from resulting articles were reviewed. The following search terms included: eccentric exercise OR eccentrics AND patellar tendinopathy OR jumper’s knee; extracorporeal shockwave therapy OR shockwave therapy AND patellar tendinopathy OR jumper’s knee; and tendinopathy (which included AT for the systematic review). The systematic review articles include the same PICO requirements (athletic population with tendinopathy (but specifically AT), EE (I), ESWT (C) and VISA-P and VAS, outcomes.
Eligibility Criteria
Inclusion criteria consisted of the following: subjects over 18 years of age, a history of exercise-related patellar tendon pain for at least 3 months, RCTs, published in the peer-reviewed journals in the year 2003 or later, published in English, use of the Victorian Institute of Sport Australia - Patella (VISA-P) and/or the Visual Analog Scale (VAS) outcome measures, use of the Alfredson protocol, 12-week follow-up data available with both means and standard deviations. Exclusion criteria consist of the following: concurrent corticosteroid or NSAID use during the study period, use of local anesthesia prior to ESWT treatment, pregnancy, subjects with a history of knee surgery, inflammatory or degenerative joint conditions, and symptoms for less than 3 months. For the systematic review search extended to AT
Outcome Measures
The VISA-P scale is a subjective measure used to quantify functional deficits experienced by athletes with PaT [51]. The outcome measure is a self-administered 8- item scale that provides information about pain during functional activities and sports participation [52]. The VISA-P is currently the most widely used outcome measure for athletes with PaT, but the minimum clinically important difference is unknown. The VAS is validated for its accuracy in recording changes in both acute and chronic pain [53, 54].
Operational Definitions
Athletes were defined as those regularly active in a sport or exercise-based activity at either elite or recreational levels. Eccentric exercise was defined by Purdam, et al. [30] adaptation of Alfredson’s [55]. protocol to the patellar tendon. Knee flexion at the bottom of the squat was required to be at least 70°. Extracorporeal shockwave therapy was defined as 3 sessions provided, without local anesthesia as Roope, et al. [59] showed better effect without local anesthesia and intervals were between 48 hours to 1 week because best parameters for PaT are unknown, ESWT treatment was broadened to any protocol The 11-point PEDro served as the primary evaluation measure for studies included in both the meta-analysis and systematic review [56]. Because none of the included studies analyzed both EE and ESWT, it was necessary to combine studies to generate comparisons. Studies were matched based on population size, symptom duration, type of athletes included, and mean baseline VISA-P and VAS scores. Means and standard deviations were used to determine effect size, confidence interval, Q statistic, and p-value for analysis. Cohen’s categorization of ES was used [57] and forest plots were used for visual representation of ES.
Study Selection
See consort Figure 1. for included studies for the Meta-analysis. For the systematic review the effects of both EE and ESWT were reviewed however, articles also included the lower extremity tendinopathy AT along with PaT, the two most common tendinopathies in athletes [58, 59]. For both reviews the PICO, inclusion and exclusion criteria were observed however for the systematic review an extended age, additional research designs and an expansion of outcome were permitted provided the study also used one of the meta-analysis measurements.
![Figure 1: for included studies for the Meta-analysis. For the systematic review the effects of both EE and ESWT were reviewed however, articles also included the lower extremity tendinopathy AT along with PaT, the two most common tendinopathies in athletes [58,59]. For both reviews the PICO, inclusion and exclusion criteria were observed however for the systematic review an extended age, additional research designs and an expansion of outcome were permitted provided the study also used one of the meta-analysis measurements.](/fulltextimages/3914/fig_1.png)
Results
Meta-Analysis Study Characteristics
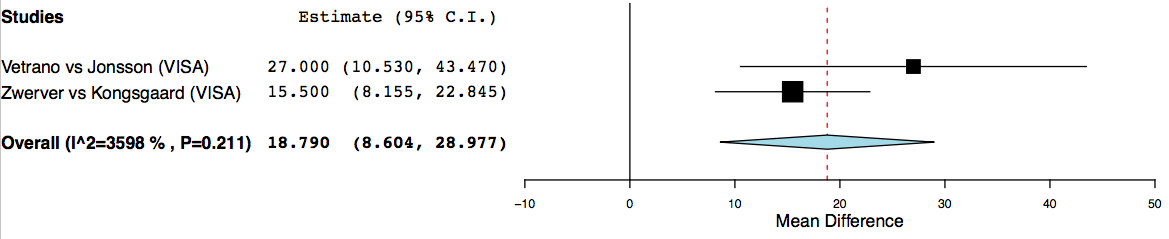
Among the 4 included studies, PEDro scores ranged from a low of 4 to as high as 9 out of 10. All 4 were level 1 RCTs with the most prominent threat being blinding of therapists. All of the studies lasted 12 weeks, except for Vetrano, et al. which ran for 8 weeks Both Jonsson, et al. and Kongsgaard, et al. [60, 61, 62, 63]. used the same EE protocol [30] however, ESWT differed by device and treatment parameters. There were a broad range of symptom durations the meta-analysis studies (range from 3 months to 3 years with mean average of 18.8±13 months) [64]. The majority of studies included were all level 1 RCT’s with the exception of one level four observational study [65].
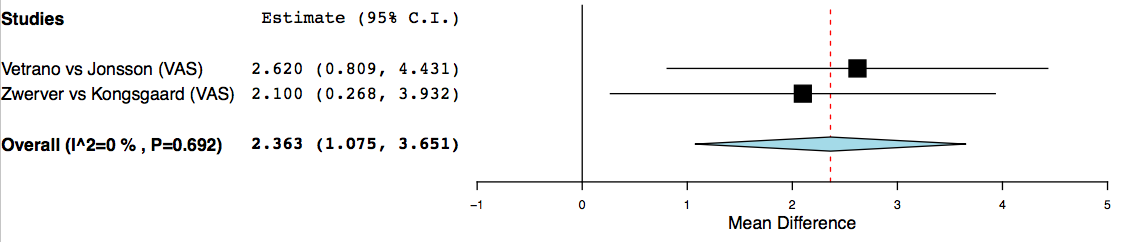
Meta-analysis-Synthesis of Results
The alternative hypothesis of this meta-analysis that EE would result in a greater treatment effect in reducing pain and improving function than ESWT was accepted for both the VISA-P and VAS measures. The grand effect size for the VISA-P analysis was 18.790 (8.604, 28.977) (Figure 2) and for the VAS the grand effect was 2.363 (1.075, 3.651) (Figure 3). The VISA-P and VAS measures were homogenous at (Q = 1.56, p = 0.21) and (Q =.15 and p = 0.692), respectively.
Systematic Review-Study Characteristics
A total of 11 studies qualified for inclusion; 5 studies looked at athletes with AT, and 6 looked at athletes with PaT. Because of issues such as missing data or lack of follow-up reassessment the PaT studies could not be used in the meta-analysis [31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82]. The study by Purdam, et al. met all meta-analysis inclusion criteria, but was excluded due to a shortage of ESWT studies for comparison.
Achilles Tendinopathy: Eccentric Exercise
A full description of the data for the systematic review studies is included in Tables 2 and 3. The studies were mostly RCT’s. Age ranges varied with patients between the ages of 29-60 years of age and most subjects fell in the 40-50 range. All 4 of the studies looked at recreational athletes with chronic mid-portion AT, which consisted of symptoms 2-7 cm proximal to the Achilles tendon insertion point on the calcaneus and an EE only group using the Alfredson protocol for AT with a 12-week intervention periods [32, 67, 68, 69]. The Victorian Institute of Sport Australia – Achilles (VISA-A) Scale [32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68], was the most common functional outcome measure. See Table 1 for details by studies compiled.
| Treatment Parameters/ Study Length | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Outcome Measures | ||||||||||||||
| Study | Sample size (n) and characteristics | Intervention | |||||||||||||
| design | |||||||||||||||
| N=10 soccer, running, and floorball athletes | |||||||||||||||
| Jonsson | Average age=25.7±9.9 years | EE: Single limb squat on 25° | 3x15; 2x/day for 12 weeks | ||||||||||||
| RCT | VISA, VAS | ||||||||||||||
| (2005) | Duration of symptoms=15.4±6.0 months | decline board | |||||||||||||
| (range:10-24) | |||||||||||||||
| N=12 recreational male athletes | |||||||||||||||
| K | ongsgaar | d | Average age= 31.3±8.3 years | EE: Single limb squat on 25° | 3x15; 2x/day for 12 weeks | ||||||||||
| RCT | VISA, VAS | ||||||||||||||
| (2009) | Duration of symptoms=18.8±13.0 months | decline board | |||||||||||||
| (range:3-36) | |||||||||||||||
| N=31 volleyball, basketball, and handball | |||||||||||||||
| i | ESWT: using a Piezoelectric | z; | |||||||||||||
| athletes | 3 sessions at 1 week intervals; outcomes assessed at 12 weeks | ||||||||||||||
| Zwerver | device Parameters: 2000 | ||||||||||||||
| RCT | Average age= 24.2±5.2 years | VISA, VAS | |||||||||||||
| (2011) | mpulses at a frequency of 4H | ||||||||||||||
| Duration of symptoms=7.3±3.6 months (no | |||||||||||||||
| Intensity of 0.58 mJ/mm2 | |||||||||||||||
| range provided) | |||||||||||||||
| N=23 elite and non-elite basketball, volleyball | , | P | ESWT: using an | o | |||||||||||
| and soccer athletes | electromagnetic device | 3 sessions at 48-72 ho intervals; outcomes assessed at 8 weeks | ur | ||||||||||||
| Vetrano | |||||||||||||||
| RCT | Average age= 26.8±8.5 years | arameters: 2400 impulses; n | VISA, VAS | ||||||||||||
| (2013) | |||||||||||||||
| Duration of symptoms=17.6±20.2 months (no | frequency listed; Intensity of | ||||||||||||||
| range provided) | 0.17-0.25 mJ/mm2 |
Table 1: Systematic Review Study Characteristics: Achilles Tendinopathy.
- Study
- Study Design Population size (n) and characteristics
- Intervention
- Comparison Outcome
- N=10
- Average age=44.6 years
- EE: Single limb squat on
- Beyer [41]
- RCT
- Duration of symptoms=19±6.0 months
- 25° decline board
- (range:3-120)
- N=34
- Average age= 48±2 years
- EE: Single limb squat on
- DeJonge [51]
- RCT
- Duration of symptoms=30.7 months
- 25° decline board
- N=37
- Average age= 42.1±11
- EE: Single limb squat on
- Petersen [52]
- RCT years Duration of symptoms=7.1±2.6
- 25° decline board months
- N=20
- Average age=48.2±5.1
- EE: Single limb squat on
- Stasinopoulos[18]
- RCT
- 25° decline board
- VISA-A years
- N=127
- Average age=47.8±11
- ESWT: Electromagnetic device; Parameters: 1,500-
- Vulpiani [44]
- Observational years
- Duration of symptoms=7.1±12.8
- Study
- 2,500 impulses; 0.08-0.40 mJ/mm2 months
Table 2: Systematic Review Study Characteristics: Achilles Tendinopathy.
| Treatment | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Population size (n) and | |||||||||||||||||
| Study | Design | Intervention | Outcome measure | parameters/Study | |||||||||||||
| characteristics | |||||||||||||||||
| Length | |||||||||||||||||
| Purdam [19] | RCT | N=8 Athletes (8 male and 3 female) Average age=28 years | EE: Single limb squat on 25° decline board Control group with standard squats | V AS (EE significant over control (74.2 to 28.5) 6 of 8 returned to sport | 3x15; 2x/day for 12 weeks; outcomes assessed @12 weeks & 15 months | ||||||||||||
| Young [20] | RCT | N=17 13 males 4 females; Elite volleyball players Average age=27.3±1.8 years | EE: Single limb squat on 25° decline board vs. EE on a 10-cm step Significant within group difference; no between group difference Both EE decline and step group showed improves up to a year EE: Single limb squat on 25° decline board | VISA-P, VAS | 3x15; 2x/day for 12 weeks; outcomes assessed @ 12 weeks & 1 year | ||||||||||||
| Visnes [24] | RCT | N=13 Elite volleyball players; 19 males and 10 females Average age=26.8±4.6 years Duration of symptoms= 67±44 months | Control performing sports training as usual | VISA-P No significant between group difference Both significant within group difference | 3x15; 2x/day for 12 weeks; outcomes assessed @ 6 weeks & 6 months | ||||||||||||
| Vulpiani [45] | Observa- tional | N=73 54 male and 19 female Duration of symptoms=>3 months | ESWT: Electromagnetic device; Parameters: 1,500-2,500 impulses; 0.08-0.44 mJ/mm2 2-7 day interval period between treatments depending on pain and presence of calcifications | VAS changes with ADL’s Significant change in VAS | 3-5 sessions @ 2-7-day intervals; outcomes assessed at 1, 6-12, 13- 24, and >24 months Attrition of subjects @later follow-ups | ||||||||||||
| Taunton [46] | RCT | N=20; 10 male; 10 female Duration of symptoms=>3 months | ESWT: Electromagnetic device; Parameters: 2,000 impulses; 0.17 mJ/mm2 ; frequency not known | VISA-P, Vertical jump Control Significant VISA-P within group for ESWT; Significant between group vertical jump over control | 3-5 sessions @ 1 week intervals; outcomes assessed at 5 & 12 weeks | ||||||||||||
| Van der Worp [47] | RCT | N=43 with bilateral involvement 57 tendons; 32 male; 11 female Average age=31.1±10.7 years Duration of symptoms=35.2±43.5 | 3 treatments; ESWT- Electromagnetic device; FSWT Parameters: 2,000 impulses; frequency of 4Hz; Intensity of 0.12 mJ/mm2 RSWT 2.4 intensity (comparable to .12 mJ/mm2 at 8 Hz Radial to focused shockwave) | VISA-P, VAS during ADL’s and decline squat Significant changes in VISA-P @ 14 wk for both ESWTs no between group difference | 3 sessions @ 1 week intervals; outcomes assessed at 1, 4, 7, & 14 weeks |
Table 3: Systematic Review Study Characteristics: Patellar Tendinopathy.
Each of the 4 studies demonstrated a statistically significant within-group improvement on the part of the pure EE group for the VISA-A [32, 67, 68, 69]. Of the studies that used pain as an outcome measure, both reported statistically significant within-group improvement for the VAS [67, 68, 69]. Additionally, Petersen demonstrated improvement on the pain subscale of the SF-36 in the EE. However this study showed no significant difference between subjects treated with EE and those receiving an AirHeel brace [69]. Likewise, Beyer’s study failed to show a significant difference between EE and heavy slow resistance training [67].
Achilles Tendinopathy: Extracorporeal Shockwave Therapy
A single study by Vulpiani et al. [70] utilized ESWT as an intervention for AT and met all other inclusion criteria for the systematic review. This level 4 observational study examined a mixed population of 105 professional and recreational athletes (89 males and 16 females) with both
| 47.8 | ±12.8. The majority (60%) of subjects were amateur | ||
|---|---|---|---|
| athletes, 30.5% practiced sports at least once per week, | |||
| and 10.5% competed at the professional level. Symptoms | |||
| were required to be present for longer than 6 months to | |||
| qualify as a subject | [70] | . |
| The mean VAS significantly decreased from 7.49 | ±1.6 | |
|---|---|---|
| to 4.75±2.9 at the 2-month follow-up point. The mean | ||
| score further decreased to 2.88±3.1 and 2.6±3.3 at | ||
| medium and long-term follow-ups respectively. The | ||
| authors concluded that ESWT appears to be a viable | ||
| treatment option for athletes with AT, leading to long- | ||
| lasting improvement in pain without collateral damage | ||
| [70] | . |
Patellar Tendinopathy: Eccentric Exercise
Three studies all used the Alfredson protocol adapted to the Patellar tendon for a 12 week intervention period. Subjects were a mix of males and female, and all were athletes. In the three studies subject ages ranged between 18 to 35 and the VAS and VISA-P were measured [30, 31, 32, 33]. Two studies found not significant difference compared to a control group and although Young, M et al. [31] found significant within group differences for the both groups (Traditional Alfredson protocol and EE performed on a 10 cm step), there was not between group differences for a superior approach of EE. Young, et al.’s significance was found at both 12 weeks and 1 year post [30, 31, 32, 33].
| Patellar Tendinopathy: Exracorporeal | |
|---|---|
| Shockwave Therapy |
Three studies also examined the effect of ESWT on PaT [65, 66, 67, 68, 69, 70]. Subjects ranged from 15 to 69 with an approximate mean age of 31.1±10.7. Mean symptom duration was 35.2±43.5 with all subjects having symptoms for at least 3 months and subject were male and female. Studies included VAS and VISA-P and change in vertical jump [65, 66]. Study protocols ranged from 4Hz to 8Hz, 0.08 to 0.44 mJ/mm2 , and 1,500 to 2,500 impulses. There was not a difference between focal versus radial shockwave but both showed and significant within group improvement. ESWT should significant improvement in VISA-P and vertical jump over controls and ESWT was effective with eccentric drop squat protocol [70].
Discussion
The purpose of this meta-analysis and systematic review was to evaluate the current literature for both EE and ESWT in the treatment of PaT. Most studies have demonstrated improvement using both interventions, however the results of this meta-analysis show that EE is more effective than ESWT at both reducing pain and improving function in athletes with PaT.
Eccentric Exercise and Pain Reduction
The efficacy of EE in reducing PaT pain is shown in several studies [30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71] possibly due to a stimulatory effect of EE on collagen synthesis with an increase in peritendinous type I collagen, which is primary seen in non-pathological tendons. There is also an inverse correlational between increased type I collagen and decreased pain levels [24]. In AT, EE also causes a temporary decrease in blood flow of peritendinous vessels and it is believed this disruption of flow cause changes in nerve signaling which may influence pain perception [72].
Eccentric exercise may have appeared more effect because more jumping athletes were included in the ESWT studies and PaT is more aggravated by jumping sports5,73, and thus would negatively affected the VAS score. Another threat affecting ESWTs success on pain, such as the case with Zwerver et al. [12] was not placing activity restrictions on subjects during the 12-week treatment period [62]. Other studies such as Jonsson and Kongsgaard placed some activity restrictions on athletes. Continued training could have led to the accumulation of microtrauma over time due to overloading pathological tendons. Continuous microtrauma, in turn, may lead to a failed healing response associated with collagen fibril degeneration, tendon disrepair, and mechanical failure of the tendon [11, 13]. It stands to reason that this difference may explains the 2.1-point difference in effect size.
Finally, EE may have been superior for pain reduction because some of the EE groups such as subjects in Zwerver’s study, had the lowest mean baseline VAS score, meaning they were less symptomatic than the others [62].
Eccentric Exercise and Improved Function
This study is not the first to demonstrate improved functional performance following EE treatment. Several others studies have also found that EE improved VISA-P scores in both athletic and non-athletic subjects with PaT [31, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93] and these studies suggests that treatment effect may be due to a mechanical load-induced reversal of the degenerative process where tensile loading can have an effect on tenocyte production of growth factor release and protein synthesis [24, 78, 79]. These anabolic components may help repair the extracellular matrix, leading to a normalization of both tendon structure and vascularity [72, 73, 74, 75, 76, 77, 78, 79, 80].
The positive effects of EE may be accentuated by placing limitations on sports participation during the treatment period. Several studies that instituted activity restrictions reported favorable results [60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85]. Additionally, Liu et al noted that avoidance of painful sports activity plays a crucial role in the healing process of PaT [76]. Visnes, et al. [33] allowed athletes to resume normal training and competition, and found no functional improvement following a 12-week EE training program. Like those by Zwerver and Vetrano, this study also included elite volleyball athletes. This variable alone could have contributed to the poor outcome, due to the high impact nature of the sport.
| Systematic Review on Common Lower | |
|---|---|
| Extremity Tendinopathies |
Four studies examined the effects of EE on subjects with AT [32, 67, 68, 69]. All 4 reported significant increase in functional ability. Both Beyer, et al. and Petersen et al. [67, 69] demonstrated significant improvement in pain. A single study by Vulpiani, et al. 2009 examined the effects of ESWT on AT at 2, 6-12, and 13-24 months. The results demonstrated a significant decrease in VAS score at 2 months with further improvements at the subsequent follow-ups [70].
Three studies, Visnes, et al. [33], Young, et al. [31], and Purdam, et al. [30], studied the effects of EE on athletes with PaT. Each conducted a 12-week EE intervention with differing follow-up periods. Young demonstrated significant improvement in both VISA-P and VAS scores [31], Purdam found a significant decrease in VAS scores [30], and Visnes reported no treatment effect [33]. The final 3 studies, Taunton, et al. [65], Van der Worp, et al. [82], and Vulpiani, et al. [64] examined the effects of ESWT on athletes with PaT. Both Taunton and Van der Worp demonstrated significant improvement in VISA-P score measured at 12 and 14 weeks respectively. Taunton also showed significant improvement in vertical jump [65]. Van der Worp and Vulpiani demonstrated significant improvement in VAS score as measured at varying follow- up times ranging from 1 month to 2 year [64, 65, 66].
| Clinical Implications of Meta-Analysis | |
|---|---|
| Combined with Systematic Review | : Achilles |
Given the fact that the systematic review on AT included only 1 ESWT study, no definitive conclusions can be drawn in regards to effectiveness of ESWT for this condition. However, the study by Vulpiani, et al. did produce a statistically significant change in VAS score in favor of the experimental group. These findings suggest that ESWT is effective in reducing pain for athletes with AT. This theory has been validated at both 4 months [44] and 1 year in the general population. However, more RCTs are necessary to confirm this finding in athletic populations.
Each of the 4 studies that examined the effect of EE on AT, compared the intervention to another treatment strategy. None included a pure control group that took part in traditional conservative treatments alone including soft tissue mobilization, manual therapy, range of motion, and modalities. Each of these 4 studies found significant improvement in favor of the EE group. However, in the absence of a pure control group, it is impossible to conclude from this review alone that EE alone is more effective than conservative management for athletes with AT. It is necessary to interpret the results in the context of the broader scope of literature.
| [25,28,86,87]. |
|---|
Clinically, these findings indicate that EE is a highly effective treatment for athletes with AT, and should be a key component of the rehabilitation program. Athletes should be dosed according to the Alfredson protocol for the Achilles tendon. Overall, there is a limited evidence to support the use of ESWT in this population and more research is necessary before this intervention can be recommended as an evidence-based treatment option for athletes with AT.
Patellar Tendinopathy
No studies currently exist that compare EE to ESWT in a population of athletes with PaT. The findings of the present study help to fill this gap in the current literature. This meta-analysis and systematic review found that both EE and ESWT effectively improve pain and functional status relative to baseline in athletes with PaT. In the present study, eccentric exercise was effective compared to a control group in 3 studies [31, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77]. However, as with AT, there was a lack of quality studies examining ESWT in athletes with PaT. Therefore, the results support that EE is currently the most effective physical therapy treatment option to address an athlete’s PaT [30, 31, 60, 61] and it also significantly improves function associated with this condition [31, 60, 61]. For these reasons, EE should be the first-option treatment for PaT and this is supported by a recent systematic review by Larsson, et al. [81]. It is also superior because it is cost-effective, non-invasive, time- efficient, and appropriate for a home exercise program [61].
Results of this meta-analysis show that EE is more effective than ESWT at reducing pain and improving function in athletic individuals with PaT. The within group sub-analyses for ESWT however, revealed that while it is effective at improving function in this population, it may not be as effective at reducing pain. Clinically, the results indicate that EE should be introduced first, and if ineffective, ESWT can then be tried. This recommendation agrees with the conclusion of Muffulli, et al. [90].
This systematic review was inconclusive regarding ESWTs effect at improving pain and function. Taunton, et al. [62] and Zwerver, et al. [65] were the only studies that compared an ESWT group to a pure control group, but produced conflicting results [62, 65]. Multiple studies on subjects with AT, that directly compared EE and ESWT for change in pain and function, have demonstrated equal or better results in the ESWT group [44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91]. However, these findings have not yet been replicated in populations with PaT.
In a long-term RCT by Wang, et al. subject with PaT were treated with a single-application of ESWT, while the control group received standard conservative treatment. At 2-3 year follow up the ESWT group achieve significantly better functional outcomes which is also supported by Van der Worp, et al.’s study that supports ESWT for improved functional performance.
Clinically, ESWT should be incorporated into a more comprehensive treatment program for tendinopathies [28, 92]. There is some evidence to suggest that the concurrent use of ESWT and EE may have a synergistic effect, but research on this topic is scarce. Existing studies have shown promising results [66, 83, 93, 94] and each of these studies found significant improvement in groups treated with both interventions. The efficacy of this combined treatment may be due to the healing effects of EE and ESWT at the cellular level that increases circulation to tendinous tissue which increased rate of collagen synthesis, and release of growth factor can combine to promote increased rates of tendon repair, decreased pain, and improved functional outcomes. Furthermore, the clear majority of studies have shown ESWT to be effective for both PaT and AT [34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96]. These studies however, included subjects from the general population rather than athletes.
Rationale for use of ESWT
Currently, the mechanism of ESWT is not fully understood [95]. It is suggested that ESWT may lead to long-term improvement in tendon function through biochemical signaling where shockwaves activate a biochemical signaling cascade. This results in the release of growth factors TGF-b1 and IGF-1. These growth factors cause an anabolic effect within the damaged tendon tissue by promoting extracellular matrix biosynthesis by tenocytes [97, 98]. There is also the release of TGF-b1, proliferating cell nuclear antigen, and nitric oxide which lead to tenocyte proliferation and collagen synthesis [99]. This stimulating effect may accelerate healing within injured tendon. Fibroblast cells treated by ESWT may also increase proliferation [100] which may lead to an increase in collagen synthesis, and therefore rebuilding of damaged tendon. The protein TGF-b1 may also be an inhibitor of macrophage-induced extracellular matrix degradation as well as play a key role in mRNA expression for both collagen types 1 and 3, which make up tenocytes [100]. Collectively, these findings seem to confirm that the activation of primary connective tissue repair processes occur following the administration of ESWT.
Limitations
There were several limitations in this study, the most prominent being the lack of research on athletes with either PaT or AT. Some studies also had lower PEDro scores and a there was a shortage of studies that directly compare EE to ESWT which necessitated the pairing of studies. Both of the EE Studies in the meta-analysis had small samples sizes skewed in favor of EE. Lack of parameter consistency of ESWT is another concern and finally, the treatment windows and follow-up times differed greatly for both interventions.
According to Wang, et al. the most important parameters when using an ESWT application for treatment of musculoskeletal disorders are pressure distribution, energy flux density, and total acoustic energy [95]. Different variations of each of these factors should be further investigated as well as delineating the optimal number of treatments, length of rest period between treatments, and most effective type of application for tendinopathies. Additionally, future studies should differentiate between subjects that are in different stages of PaT.
Conclusion
This meta-analysis demonstrated a greater decrease in pain and improvement in function using EE in athletic populations with PaT. Given the differences in study characteristics and protocols, these results should be interpreted with caution. However, it does seem safe to conclude that both EE and ESWT can safely and effectively be incorporated into a patient’s plan of care. The systematic review further revealed that both interventions were effective for PaT and AT. Collectively, this means that EE should be the first choice for treatment of PaT, while ESWT is a viable option for individuals that do not respond to EE alone. In these cases, a combination of EE and ESWT seems promising, but further research is necessary to confirm the efficacy of this approach.
References
-
Maffulli N, Longo UG, Gougoulias N, Caine D, Denaro V, et al. (2011)Sport injuries: a review of outcomes. Bri medl bull 97(1): 47-80.
-
Loppini M, Maffulli N (2011) Conservative management of tendinopathy: an evidence-based approach. MLTJ Muscles, Ligaments and Tendons Journal 1(4): 134-137.
-
Blazina M, Kerlan R, Jobe F, Carter V, Carlson G, et al. (1973) Jumper's knee. The Orthopedic clinics of North America 4(3): 665-678.
-
Peers KH, Lysens RJ (2005) Patellar tendinopathy in athletes. Sports Med 35(1): 71-87.
-
Lian OB, Engebretsen L, Bahr R (2005) Prevalence of jumper’s knee among elite athletes from different sports a cross-sectional study. The Am J of sports Med 33(4): 561-567.
-
Ferretti A (1986) Epidemiology of jumper’s knee. Sports Med 3(4): 289-295.
-
Rudavsky A, Cook J (2014) Physiotherapy management of patellar tendinopathy (jumper's knee). J Physiother 60(3): 122-129.
-
Kettunen JA, Kvist M, Alanen E, Kujala UM (2002) Long-term prognosis for jumper’s knee in male athletes a prospective follow-up study. Am J of Sports Med 30(5): 689-692.
-
Stanish WD, Curwin S, Mandell S (2000) Tendinitis: its etiology and treatment. Oxford University Press 35(2): 138-140.
-
van der Worp H, van Ark M, Roerink S, Pepping GJ, van den Akker-Scheek I, et al. (2011) Risk factors for patellar tendinopathy: a systematic review of the literature. Br J Sports Med 45(5): 446-452.
-
Cook JL, Purdam CR (2009) Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J of sports Med 43(6): 409-416.
-
Zwerver J (2008) Patellar tendinopathy ('jumper's knee'); a common and difficult-to-treat sports injury. Ned Tijdschr Geneeskd 152(33): 1831-1837.
-
Khan KM, Cook JL, Bonar F, Harcourt P, Astrom M, et al. (1999) Histopathology of common tendinopathies. Sports Medicine 27(6): 393-408.
-
Colosimo AJ, Bassett FH (1990) Jumper's knee. Diagnosis and treatment. Orthopaedic review. 19(2): 139-149.
-
Roels J, Martens M, Mulier J, Burssens A(1977) Patellar tendinitis (jumper's knee). The American journal of sports medicine 6(6): 362-368.
-
Clancy W (1990T) endon trauma and overuse injuries. Sports induced inflammation: clinical and basic science concepts Park Ridge. American Academy of Orthopaedic Surgeons.
-
Rosenbaum AJ, Wicker JF, Dines JS (2010) Histologic stages of healing correlate with restoration of tensile strength in a model of experimental tendon repair. HSS journal 6(2): 164-170.
-
Murtaugh B, Ihm JM (2013) Eccentric training for the treatment of tendinopathies. Current sports medicine reports 12(3): 175-182.
-
Sharma P, Maffulli N (2005) Tendon injury and tendinopathy: healing and repair. The Journal of Bone & Joint Surgery 87(1): 187-202.
-
Larsson ME, Kall I, Nilsson-Helander K (2012) Treatment of patellar tendinopathy--a systematic review of randomized controlled trials. Knee Surg Sports Traumatol Arthrosc 20(8): 1632-1646.
-
Rutland M, O'Connell D, Brismee JM, Sizer P, Apte G, et al. (2010) Evidence–Supported Rehabilitation Of Patellar Tendinopathy. North American Journal of Sports Physical Therapy : NAJSPT 5(3): 166-178.
-
Schwartz A, Watson JN, Hutchinson MR (2015) Patellar Tendinopathy. Sports Health 7(5): 415-420.
-
Rees JD, Wolman RL, Wilson A (2009) Eccentric exercises; why do they work, what are the problems and how can we improve them? Br J Sports Med 43(4): 242-246.
-
Langberg H, Ellingsgaard H, Madsen T (2007) Eccentric rehabilitation exercise increases peritendinous type I collagen synthesis in humans with Achilles tendinosis. Scandinavian journal of medicine & science in sports17(1): 61-66.
-
Knobloch K (2007) Eccentric training in Achilles tendinopathy: is it harmful to tendon microcirculation? British journal of sports medicine 41(6): 1-5.
-
Moore DR, Phillips SM, Babraj JA, Smith K, Rennie MJ, et al. (2005) Myofibrillar and collagen protein synthesis in human skeletal muscle in young men after maximal shortening and lengthening contractions. American Journal of Physiology- Endocrinology and Metabolism 288(6): 1153-1159.
-
Visnes H, Bahr R (2007) The evolution of eccentric training as treatment for patellar tendinopathy (jumper's knee): a critical review of exercise programmes. Br J Sports Med 41(4): 217-223.
-
Alfredson H, Pietilä T, Jonsson P, Lorentzon R (1998) Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. The American journal of sports medicine 26(3): 360-366.
-
Cannell L, Taunton J, Clement D, Smith C, Khan K, et al. (2001) A randomised clinical trial of the efficacy of drop squats or leg extension/leg curl exercises to treat clinically diagnosed jumper's knee in athletes: pilot study. British Journal of Sports Medicine 35(1): 60-64.
-
Purdam CR, Jonsson P, Alfredson H, Lorentzon R, Cook JL, et al. (2004) A pilot study of the eccentric decline squat in the management of painful chronic patellar tendinopathy. Br J Sports Med 38(4): 395- 397.
-
Young M, Cook J, Purdam C, Kiss ZS, Alfredson H,et al. (2005) Eccentric decline squat protocol offers superior results at 12 months compared with traditional eccentric protocol for patellar tendinopathy in volleyball players. British journal of sports medicine 39(2): 102-105.
-
Stasinopoulos D, Manias P (2013) Comparing two eccentric exercise programmes for the management of Achilles tendinopathy. A pilot trial. Journal of bodywork and movement therapies 17(3): 309-315.
-
Visnes H, Hoksrud A, Cook J, Bahr R (2005) No effect of eccentric training on jumper's knee in volleyball players during the competitive season: a randomized clinical trial. Clinical journal of sport medicine 15(4): 227-234.
-
Mani-Babu S, Morrissey D, Waugh C, Screen H, Barton C, et al. (2015) The effectiveness of extracorporeal shock wave therapy in lower limb tendinopathy: a systematic review. Am J Sports Med 43(3): 752-761.
-
Chung B, Wiley JP (2002) Extracorporeal shockwave therapy. Sports medicine 32(13): 851-865.
-
Maier M, Saisu T, Beckmann J (2001) Impaired tensile strength after shock-wave application in an animal model of tendon calcification. Ultrasound in medicine & biology 27(5): 665-671.
-
Wang F, Yang K, Chen R, Wang C, Sheen-Chen SM, et al. (2002) Extracorporeal shock wave promotes growth and differentiation of bone-marrow stromal cells towards osteoprogenitors associated with induction of TGF-β1. Bone & Joint Journal 84(3): 457- 461.
-
Wang CJ (2003) An overview of shock wave therapy in musculoskeletal disorders. Chang Gung medical journal 26(4): 220-232.
-
Rompe JD, Zoellner J, Nafe B (2001) Shock wave therapy versus conventional surgery in the treatment of calcifying tendinitis of the shoulder. Clinical orthopaedics and related research 387: 72-82.
-
Chen HS, Chen LM, Huang TW (2001) Treatment of painful heel syndrome with shock waves. Clinical orthopaedics and related research 387: 41-46.
-
Ko JY, Chen HS, Chen LM (2001) Treatment of lateral epicondylitis of the elbow with shock waves. Clinical orthopaedics and related research 387: 60-67.
-
Wang C-, Yang KD, Wang FS, Chen HH, Wang JW, et al. (2003) Shock Wave Therapy for Calcific Tendinitis of the Shoulder A Prospective Clinical Study with Two- Year Follow-up. The American journal of sports medicine 31(3): 425-430.
-
Rodriguez-Merchan EC (2013) The treatment of patellar tendinopathy. J Orthop Traumatol 14(2): 77- 81.
-
Rompe JD, Furia J, Maffulli N (2008) Eccentric loading compared with shock wave treatment for chronic insertional Achilles tendinopathy. The Journal of Bone & Joint Surgery 90(1): 52-61.
-
Van Leeuwen MT, Zwerver J, van den Akker-Scheek I (2009) Extracorporeal shockwave therapy for patellar tendinopathy: a review of the literature. Br J Sports Med 43(3): 163-168.
-
Verhagen AP, De Vet HC, De Bie RA (1998) The Delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. Journal of clinical epidemiology 51(12): 1235-1241.
-
Romeo P, Lavanga V, Pagani D, Sansone V (2013) Extracorporeal shock wave therapy in musculoskeletal disorders: a review. Medical Principles and Practice 23(1): 7-13.
-
Orhan Z, Cam K, Alper M, Ozturan K (2004) The effects of extracorporeal shock waves on the rat Achilles tendon: is there a critical dose for tissue injury? Archives of orthopaedic and trauma surgery 124(9): 631-635.
-
Sems A, Dimeff R, Iannotti JP (2006) Extracorporeal shock wave therapy in the treatment of chronic tendinopathies. Journal of the American Academy of Orthopaedic Surgeons 14(4): 195-204.
-
Liberati A, Altman DG, Tetzlaff J (2009) The PRISMA statement for reporting systematic reviews and meta- analyses of studies that evaluate health care interventions: explanation and elaboration. Annals of internal medicine 151(4): 65-94.
-
Visentini PJ, Khan KM, Cook JL (1998) The VISA score: an index of severity of symptoms in patients with jumper's knee (patellar tendinosis). Journal of Science and Medicine in Sport 1(1): 22-28.
-
Hernandez-Sanchez S, Hidalgo MD, Gomez A(2012) Responsiveness of the VISA-P scale for patellar tendinopathy in athletes. British journal of sports medicine 48(6): 453-457.
-
Price DD, McGrath PA, Rafii A, Buckingham B (1983) The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 17(1): 45-56.
-
Melzack R (2009) Pain measurement and assessment. Raven Press14(3): 717.
-
Rompe JD, Meurer A, Nafe B, Hofmann A, Gerdesmeyer L, et al. (2005) Repetitive low‐energy shock wave application without local anesthesia is more efficient than repetitive low‐energy shock wave application with local anesthesia in the treatment of chronic plantar fasciitis. Journal of orthopaedic research 23(4): 931-941.
-
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M, et al. (2003) Reliability of the PEDro scale for rating quality of randomized controlled trials. Physical therapy 83(8): 713-721.
-
Cohen J (1988) Statistical power analysis for the behavioural sciences. Hillside NJ: Lawrence Earlbaum Associates.
-
Rees J, Wilson A, Wolman R (2006) Current concepts in the management of tendon disorders. Rheumatology 45(5): 508-521.
-
Scott A, Ashe MC (2006) Common tendinopathies in the upper and lower extremities. Current sports medicine reports 5(5): 233-241.
-
Jonsson P, Alfredson H (2005) Superior results with eccentric compared to concentric quadriceps training in patients with jumper's knee: a prospective randomised study. Br J Sports Med 39(11): 847-850.
-
Kongsgaard M, Kovanen V, Aagaard P (2009) Corticosteroid injections, eccentric decline squat training and heavy slow resistance training in patellar tendinopathy. Scand J Med Sci Sports 19(6): 790-802.
-
Zwerver J, Hartgens F, Verhagen E, van der Worp H, van den Akker-Scheek I, et al. (2011) No effect of extracorporeal shockwave therapy on patellar tendinopathy in jumping athletes during the competitive season: a randomized clinical trial. Am J Sports Med 39(6): 1191-1199.
-
Vetrano M, Castorina A, Vulpiani MC, Baldini R, Pavan A, et al. (2013) Platelet-rich plasma versus focused shock waves in the treatment of jumper's knee in athletes. Am J Sports Med 41(4): 795-803.
-
Vulpiani M, Vetrano M, Savoia V, Di Pangrazio E, Trischitta D, et al. (2007) Jumper's knee treatment with extracorporeal shock wave therapy: a long-term follow-up observational study. Journal of Sports Medicine and Physical Fitness 47(3): 323-328.
-
Taunton K, Taunton J, Khan K (2003) Treatment of patellar tendinopathy with extracorporeal shock wave therapy. British Columbia Medical Journal 45(10): 500-507.
-
Van der Worp H, Zwerver J, Hamstra M, van den Akker-Scheek I, Diercks RL, et al. (2014) No difference in effectiveness between focused and radial shockwave therapy for treating patellar tendinopathy: a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc 22(9): 2026-2032.
-
Beyer R, Kongsgaard M, Hougs Kjær B, ohlenschlæger T, Kjær M, et al. (2015) Heavy slow resistance versus eccentric training as treatment for Achilles tendinopathy: a randomized controlled trial. The American journal of sports medicine 43(7): 1704- 1711.
-
De Jonge S, De Vos RJ, Van Schie HT, Verhaar JA, Weir A, et al. (2008) One-year follow-up of a randomised controlled trial on added splinting to eccentric exercises in chronic midportion Achilles tendinopathy. British journal of sports medicine 46(3): 214-218.
-
Petersen W, Welp R, Rosenbaum D (2007) Chronic Achilles tendinopathy a prospective randomized study comparing the therapeutic effect of eccentric training, the AirHeel brace, and a combination of both. The American journal of sports medicine 35(10): 1659-1667.
-
Vulpiani M, Trischitta D, Trovato P, Vetrano M, Ferretti A, et al. ( 2009) Extracorporeal shockwave therapy (ESWT) in Achilles tendinopathy. A long-term follow-up observational study. Journal of Sports Medicine and Physical Fitness 49(2): 171-176.
-
Stasinopoulos D, Stasinopoulos I (2004) Comparison of effects of exercise programme, pulsed ultrasound and transverse friction in the treatment of chronic patellar tendinopathy. Clinical rehabilitation 18(4): 347-352.
-
ohberg L, Lorentzon R, Alfredson H (2004) Eccentric training in patients with chronic Achilles tendinosis: normalised tendon structure and decreased thickness at follow up. British journal of sports medicine 38(1): 8-11.
-
Ferretti A, Puddu G, Mariani PP, Neri M (1984) Jumper's knee: an epidemiological study of volleyball players. The Physician and Sportsmedicine 2(10): 97- 106.
-
Cook JL, Khan KM, Kiss ZS, Purdam CR, Griffiths L. (2000) Prospective imaging study of asymptomatic patellar tendinopathy in elite junior basketball players. Journal of Ultrasound in Medicine 19(7): 473-479.
-
Frohm A, Saartok T, Halvorsen K, Renstrom P (2007) Eccentric treatment for patellar tendinopathy: a prospective randomised short-term pilot study of two rehabilitation protocols. Br J Sports Med 41(7): 7.
-
Liu XG, Cheng L, Song JM (2014) Effects of low-level laser therapy and eccentric exercises in the treatment of patellar tendinopathy. International Journal of Photoenergy.
-
Lavagnino M, Arnoczky SP, Tian T, Vaupel Z (2003) Effect of amplitude and frequency of cyclic tensile strain on the inhibition of MMP-1 mRNA expression in tendon cells: an in vitro study. Connective tissue research 44(3-4): 181-187.
-
Wang JHC, Thampatty BP, Lin JS, Im HJ (2007) Mechanoregulation of gene expression in fibroblasts. Gene 391(1-2): 1-15.
-
Koenig M, Torp‐pedersen S, Qvistgaard E, Terslev L, Bliddal H (2004) Preliminary results of colour Doppler‐guided intratendinous glucocorticoid injection for Achilles tendonitis in five patients. Scandinavian journal of medicine & science in sports 14(2): 100-106.
-
Furia JP, Rompe JD, Cacchio A, Del Buono A, Maffulli N, et al. (2013) A single application of low-energy radial extracorporeal shock wave therapy is effective for the management of chronic patellar tendinopathy. Knee Surg Sports Traumatol Arthrosc 21(2): 346-350.
-
Wang CJ, Ko JY, Chan YS, Weng LH, Hsu SL, et al. (2007) Extracorporeal shockwave for chronic patellar tendinopathy. Am J Sports Med 35(6): 972-978.
-
Peers KHE, Lysens RJJ, Brys P, Bellemans J (2003) Cross-sectional Outcome Analysis of Athletes With Chronic Patellar Tendinopathy Treated Surgically and by Extracorporeal Shock Wave Therapy. Clinical Journal of Sport Medicine 13(2): 79-83.
-
Bahr R, Fossan B, Loken S, Engebretsen L (2006) Surgical treatment compared with eccentric training for patellar tendinopathy (jumper's knee). J Bone Joint Surg Am 88(8): 1689-1698.
-
Furia J (2005) Extracorporeal shockwave therapy in the treatment of chronic insertional Achilles tendinopathy. Der Orthopade 34(6): 571-578.
-
Kingma JJ, De Knikker R, Wittink H, Takken T (2007) Eccentric overload training in patients with chronic Achilles tendinopathy: a systematic review. British journal of sports medicine 41(6): 1-5.
-
Mafi N, Lorentzon R, Alfredson H (2001) Superior short-term results with eccentric calf muscle training compared to concentric training in a randomized prospective multicenter study on patients with chronic Achilles tendinosis. Knee Surgery, Sports Traumatology, Arthroscopy 9(1): 42-47.
-
Sayana MK, Maffulli N (2007) Eccentric calf muscle training in non-athletic patients with Achilles tendinopathy. Journal of Science and Medicine in Sport 10(1): 52-58.
-
Larsson ME, Käll I, Nilsson-Helander K (2012) Treatment of patellar tendinopathy—a systematic review of randomized controlled trials. Knee surgery, sports traumatology, arthroscopy 20(8): 1632-1646.
-
Maffulli N, Longo UG, Denaro V (2010) Novel approaches for the management of tendinopathy. J Bone Joint Surg Am 92(15): 2604-2613.
-
Rompe JD, Nafe B, Furia JP, Maffulli N (2007) Eccentric Loading, Shock-Wave Treatment, or a Wait- and-See Policy for Tendinopathy of the Main Body of Tendo Achillis A Randomized Controlled Trial. The American journal of sports medicine 35(3): 374-383.
-
Alfredson H, Cook J (2007) A treatment algorithm for managing Achilles tendinopathy: new treatment options. Br J Sports Med 41(4): 211-216.
-
Rompe JD, Furia J, Maffulli N (2009) Eccentric Loading Versus Eccentric Loading Plus Shock-Wave Treatment for Midportion Achilles Tendinopathy A Randomized Controlled Trial. The American journal of sports medicine 37(3): 463-470.
-
Rasmussen S, Christensen M, Mathiesen I, Simonson O (2008) Shockwave therapy for chronic Achilles tendinopathy: a double-blind, randomized clinical trial of efficacy. Acta Orthopaedica 79(2): 249-256.
-
Wang CJ (2012) Extracorporeal shockwave therapy in musculoskeletal disorders. Journal of Orthopaedic Surgery and Research 7(1): 11.
-
Carulli C, Tonelli F, Innocenti M, Gambardella B, Muncibì F, et al. (2016) Effectiveness of extracorporeal shockwave therapy in three major tendon diseases. Journal of Orthopaedics and Traumatology 17(1): 15-20.
-
Abrahamsson SO (1997) Similar effects of recombinant human insulin‐like growth factor‐I and II on cellular activities in flexor tendons of young rabbits: Experimental studies in vitro. Journal of Orthopaedic Research 15(2): 256-262.
-
Banes AJ, Horesovsky G, Larson C (1999) Mechanical load stimulates expression of novel genesin vivoandin vitroin avian flexor tendon cells. Osteoarthritis and Cartilage 7(1): 141-153.
-
Chao YH, Tsuang YH, Sun JS (2008) Effects of shock waves on tenocyte proliferation and extracellular matrix metabolism. Ultrasound in medicine & biology 34(5): 841-852.
-
Berta L, Fazzari A, Ficco AM, Enrica PM, Catalano MG, et al. (2009) Extracorporeal shock waves enhance normal fibroblast proliferation in vitro and activate mRNA expression for TGF-β1 and for collagen types I and III. Acta orthopaedica 80(5): 612-617.
-
Frairia R, Berta L (2011) Biological effects of extracorporeal shock waves on fibroblasts. A review. MLTJ Muscles, Ligaments and Tendons Journal 1(4): 138-147.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial