Occupational Therapy Intervention in Functional Communication Program with Biomechanical and Rehabilitative Approach for Guillain-Barre Syndrome Patient: A Case Study
Guillain-Barre Syndrome is an immune system-mediated disease that attacks the peripheral nervous system. Biomechanical and Rehabilitative frameworks are used to restore functional ability (remediation) and continue with modifying tasks or environments (adaptation and compensation), which aim to form patient occupational performance to be more optimal. This Final Project discusses patients with problems in functional communication activities. The results of occupational therapy assessments indicate that there are limitations that affect the problem including muscle strength, joint range of motion and endurance. Changes in patient performance satisfaction were evaluated using the Canadian Occupational Performance Measure (COPM) instrument. The results of occupational therapy management show that there is a change in patient performance satisfaction in functional communication activities.
Introduction
Guillain – Barre Syndrome (GBS) is an autoimmune disease which the immune attack is directed against the myelin, causing loss of the myelin sheath and leading to a “short circuit” so that electrical messages cannot travel between the brain and the periphery of the body [1]. Damage to the nerves makes it hard for them to transmit signals. As a result, the muscles have trouble responding to the brain [2]. GBS damages the myelin sheath that wraps around nerve axons and causes a nerve conduction block, leading to muscle weakness and pain or paralysis of the whole body [3]. GBS is a rare disease. There are approximately 2.0 cases of GBS for every 100,000 people each year worldwide [1]. The incidence of GBS increases with age from 1 per 100,000 in those aged below 30 years to about 4 cases per 100,000 in those older than 75 years [4]. Approximately 50% of those diagnosed return to normal health by 1 year, but almost one- third continue to have some muscle weakness even after 3 year [5]. There are two forms of immunotherapy for GBS that have been shown to accelerate recovery: plasma exchange and intravenous immunoglobulin (IVIg). No treatment has been shown to definitely reduce the initial severity of GBS [1]. Treatment for GBS should be started as soon as the diagnosis is made because delay in treatment results in increased nerve damage; thus, recovery is delayed or incomplete. Infections often precede the onset of symptoms, and treatments such as plasma exchanges or intravenous immunoglobulin infusions alleviate the symptoms (American Association of Neuromuscular and Electrodiagnostic Medicine [5], 2016). However, some patients with GBS experience negative effects on the activities of daily living (ADL) and impaired muscular function even at 3–6 years after the onset of GBS. Therefore, it is important for patients with GBS to undergo rehabilitation treatment to increase the likelihood of achieving independence in the activities of daily living and to improve muscular muscle strength, joint range of motion and endurance [6].
Occupational therapy has a role in the case of GBS in the rehabilitation care area. Occupational therapy uses professional expertise and involves patients in activities that aim to restore optimal independence in three areas of Occupational Performance Area (OPA) including, Activity of Daily Living (ADL) in which there are Instrumental Activity of Daily Living (IADL), Productivity and Leisure [7]. Occupational therapy can improve the performance of GBS patients with a frame of reference that is owned such as Biomechanics and Rehabilitation. The Biomechanical frame of reference is used to increase muscle strength, joint range of motion and endurance in carrying out activities. Meanwhile, the Rehabilitative Reference Framework is used to help GBS patients restore their original abilities, physically, mentally, socially, vocationally and economically which are useful for an individual with assets owned [8]. One of the difficulties experienced by GBS patients in the IADL area is in communication activities. Communication is a two- way process in which participants exchange ideas, thoughts, messages in oral and written ways with the aim that the information conveyed can be understood [9]. Mankind has experienced diverse ways of communicating. 50 years ago, people communicated by mail, telegram, radio, television, magazines. However, along with the times, technology has developed a lot. Nowdays, people communicate through communication devices or gadgets such as cell phones, computers, tablets that are supported by the internet, which allows people to use e-mail, chatrooms and videocalls for faster communication [10].
In the IADL area, GBS patients can experience problems in functional communication activities due to weakness of upper extremitys experienced. Functional communication is the activity of sending, receiving, and interpreting information using various systems and equipment including stationery, telephones (cellphones / smart phones), keyboards, audiovisual recorders, computers / tablet, and various other telecommunications devices [11]. At the end of 2011, there were more than 5.9 billion mobile- cellular telephone subscriptions. But this will not mean that everyone has access to mobile telephony [12]. People with physical disabilities often cannot access cellphones because they do not have the necessary accessibility features. 15% of the world’s population, or more than one billion people have physical disabilities that affect their access to modern communication, namely the use of cellphones, computers, laptops or tablet [12]. The use of communication tools can be a medium of resilience for patients. Resilience is the ability of humans to deal with, overcome, strengthen themselves, and even make changes after experiencing unpleasant experiences (adversity) [13]. Communication with family can increase patient motivation to recover [14]. Based on research conducted by Kane in 2016 on 20 participants, the results showed that the use of accessible communication tools for GBS patients could enable patients to be able to communicate independently with friends, family, relatives or caregivers [15]. Therefore, the authors are interested in discussing this case study.
Research Methods
Participants
This research was conducted on a 45 years old was diagnosed with Guillain-Barre Syndrome (GBS) since last July 2018. The GBS condition he experienced caused a decrease in the capacity of his occupational performance. Respondents experienced obstacles in carrying out daily activities, especially when using the telephone to communicate with their families. The respondent complained that he had not been able to carry out functional communication activities, which is the use of gadgets independently because of the muscle weakness he experienced. He underwent occupational therapy to increase the range of joint motion and muscle strength in the upper extremities and to restore functional ability to daily activities.
Instrument
This study uses Canadian Occupational Performance Measurement (COPM) as the examination instrument. This instrument uses the client principle - centered assessment that is used to measure and evaluate scores of interests, performance and patient satisfaction in an activity. Interest scores start on a scale of 1-10, where 1 means not important at all and 10 means very important. This instrument can help patients determine the outcome of the therapy they want and help the therapist in directing the intervention to be given to the patient [16].
Design
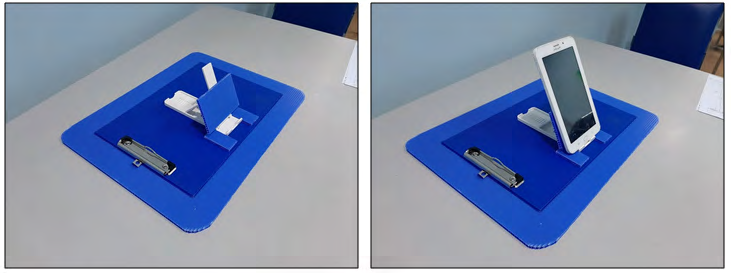
This study intervened in one subject, with the diagnosis of Guillain-Barre Syndrome (GBS) using the Biomechanics and Rehabilitation approach. The Biomechanical approach is used to increase the range of joint motion and the muscle strength of the patient. Meanwhile, the Rehabilitation approach is used to improve the ability of patients to use gadgets (tablet) with the existence of a modification tool in the form of a gadget holder designed by researchers. It aims to improve the patient’s ability in functional communication activities, namely the use of gadgets (tablet) for 26 meetings.

Result
| Upper Extremity | Pre- Active Range of Motion | Post- Active Range of Motion | Change (post-Pre) | |||
|---|---|---|---|---|---|---|
| Dextra | Sinistra | Dextra | Sinistra | Dextra | Sinistra | |
| Shoulder Flexion | 50° | 50 | 130° | 130 | 80° | 80° |
| Extension | 10 | 10 | 40° | 40 | 30° | 30° |
| Adduction | 10 | 10 | 40° | 40 | 30° | 30° |
| Abduction | 50 | 50 | 130° | 130 | 80° | 80° |
| Elbow Flexion | 10 | 10 | 150° | 140 | 140° | 130° |
| Forearm Pronation | 20 | 20 | 80° | 70 | 60° | 50° |
| Supination | 20 | 20 | 80° | 80 | 60° | 60° |
| Wrist Flexion | 10 | 10 | 50° | 40 | 40° | 30° |
| Extension | 10 | 10 | 60° | 50 | 50° | 40° |
| Thumb Flexion | 10 | 0 | 60° | 50 | 50° | 50° |
| Extension | 10 | 0 | 60° | 50 | 50° | 50° |
| Abduction | 10 | 0 | 60° | 50 | 50° | 50° |
| Finger 2 Flexion | 10 | 0 | 50° | 40 | 40° | 40° |
| Extension | 0 | 0 | 30° | 30 | 30° | 30° |
| Abduction | 0 | 0 | 30° | 20 | 30° | 20° |
| Upper Extremity | Pre - Active Range of Motion | Post - Active Range of Motion | Change (Post- Pre) | |||
| Dextra | Sinistra | Dextra | Sinistra | Dextra | Sinistra | |
| Shoulder Flexion | 2+ | 2+ | 4- | 4- | 4 | 4 |
| Extension | 2+ | 2+ | 4- | 4- | 4 | 4 |
| Adduction | 2+ | 2+ | 4- | 4- | 4 | 4 |
| Abduction | 2+ | 2+ | 4- | 4- | 4 | 4 |
| Elbow Flexion | 1 | 1 | 4- | 4- | 8 | 8 |
| Extension | 1 | 1 | 4- | 4- | 8 | 8 |
| Forearm Pronation | 1 | 1 | 4- | 4- | 8 | 8 |
| Supination | 1 | 1 | 4- | 4- | 8 | 8 |
| Wrist Flexion | 1 | 1 | 4- | 4- | 8 | 8 |
| Extension | 1 | 1 | 4- | 4- | 8 | 8 |
| Thumb Flexion | 2- | 2- | 4- | 4- | 6 | 6 |
| Extension | 2- | 2- | 4- | 4- | 6 | 6 |
| Abduction | 2- | 2- | 4- | 4- | 6 | 6 |
| Finger 2 Flexion | 2- | 2- | 4- | 4- | 6 | 6 |
| Extension | 2- | 2- | 4- | 4- | 6 | 6 |
| Abduction | 2- | 2- | 4- | 4- | 6 | 6 |
Table 1: Evaluation of Joint Range of Motion Examination
- Conclusion: Based on the table above, it can be concluded that there was a significant change in the scope of motion of the upper extremity joints after being given an OT intervention with a maximum change of 140°. Likewise,
- Conclusion: Based on the table above, it can be concluded that there is a significant change in the strength of the upper extremity muscle with a change in the maximum score of +8.
- Occupational Performance
- Problem(A)
- Importance (B)
- Performance (C)
- Satisfaction (D)
- Performance (E)
- Satisfaction(F)
- 1. Using a tablet
- 9
- 6
- 6
- 8
- 9
Table 2: Results of the Initial Assessment of COPM.
Likewise there is a significant change in the left side of upper extremity muscle strength with a change in the maximum score of +8.
Pre - Intervention February 8th 2019 Post - Interventio: May 9th 2019
- Conclusion: Based on the table above, it can be concluded that there was a significant change in the scope of motion of the upper extremity joints after being given an OT intervention with a maximum change of 140°. Likewise,
- Conclusion: Based on the table above, it can be concluded that there is a significant change in the strength of the upper extremity muscle with a change in the maximum score of +8.
- Occupational Performance
- Problem(A)
- Importance (B)
- Performance (C)
- Satisfaction (D)
- Performance (E)
- Satisfaction(F)
- 1. Using a tablet
- 9
- 6
- 6
- 8
- 9
Table 2: Results of the Initial Assessment of COPM.
Conclusion: Based on the table above, it can be concluded that patients experienced an increase in the performance score worth 2 points from the pre – intervention and post – intervention after OT intervention. Patients also experienced an increase in the satisfaction score of using the tablet worth 3 points. The increase in points shows a significant change in patient performance and satisfaction in using tablet.
| Problem | Impostance | Pre – Intervention | Post - Intervention | |||
|---|---|---|---|---|---|---|
| (A) | (B) | |||||
| 1 | Using of tablet | 9 | Performance | Satisfaction | Performance | Satisfaction |
| (C) | (D) | (E) | (F) | |||
| 6 | 6 | 8 | 9 | |||
| (G) (H) 54 54 | B x C | B x D | B x E | B x F | ||
| (I) | (J) | |||||
| 72 | 81 | |||||
| Performance Score | ||||||
| Pre – Intervention (K) | = 54 | Pre – Intervention (M) | = 54 | |||
| Post – Intervention (L) | = 72 | Post – Intervention (N) | = 81 | |||
| Performance Score Change | Satisfaction Score Change | |||||
| (L – K) | 18 | (N – M) | 27 |
Table 3: Evaluation of COPM Assessment.
Conclusion: Based on the table above, it can be concluded that there is a relation between the importance of using tablet and patient performance. At the pre - assessment, the results were 54 points. After the OT intervention, there are changes in results to 72 points. Likewise, there is a relation between the importance of using tablet and the level of patient satisfaction. At the pre - assessment, it was found that the satisfaction level was 54 points. After an OT intervention, the patient satisfaction level changed to 81 points. The increase in points shows a significant change in patient performance and satisfaction in using tablet.
Discussion
In this study there is a significant change in the range of joint motion and muscle strength of patients with Acute Inflammatory Deminelinating Polyradiculoneuropathy (AIDP) type after the OT intervention using the Biomechanical frame of reference. The same thing happened in a previous study conducted by Khanzada and Zameer entitled “Effectiveness of Occupational Therapy in Rehabilitation of Guidance - Barre Syndrome: A Case Study” in Pakistan in 2016 with a male respondent, with the Acute Motor type GBS patient -Sensory Axonal Neuropathy (AMSAN) which also experienced the increase of range of joint motion and muscle strength after OT intervention using the Biomechanical frame of reference. However, in the research the author did, the score change of the scope of range of joint motion and muscle strength was greater than the results of the intervention carried out by Khazanda and Zameer. This is because in patients who were intervened by Khazanda and Zameer, he experienced sensory disorders in the area of the upper extremity. Whereas, in patients who was assessed in this study has no sensory disorders. So it can be concluded that sensory function can affect changes in the score of range of joint motion and muscle strength. This will be related to the patient’s ability to carry out activities.
In this study, it was also found that patient was able to carry out functional communication activities, nehich is the use of gadgets (tablet) independently by using a modification tool in the form of a gadget holder after OT intervention using the Rehabilitative frame of reference. The same thing happened in the study conducted by Khanzada and Zameer, with the results that patients were able to perform ADL such as eating and brushing independently using a modified spoon and universal cuff for toothbrush after OT intervention using the Rehabilitative reference frame. So, it can be concluded that the use of tools for modification or adaptation of tools can help GBS patients to be able to carry out daily activities independently.
Based on the feasibility study conducted by Dahlstrand, on the COPM examination, a change in score of 2 points between the pre – assessment and post - assessment was considered a meaningful change clinically [17]. In this study, changes in the score of patient performance changed by 2 points and changes in the score of patient satisfaction changed by 3 points, which means that patient experienced significant changes in performance and satisfaction in functional communication activities, which is the use of gadgets (tablet). Based on this result, it can be concluded that OT intervention using the Biomechanical and Rehabilitative frame of reference is appropriate for GBS patients. The OT intervention can help patients achieve functional abilities to carry out daily activities independently.
Conclusion
Based on the study that has been done, the authors can conclude that the Biomechanical frame of reference is able to help GBS patients to increase the scope of joint motion and muscle strength. There is an increase in ROM at a maximum of 140° in the upper extremity and equal to 130° in the upper extremity. There is also an increase in the score of muscle strength with a maximum score of +8 points in the right side of upper extremity and +8 points in the left side of upper extremity of the limb. During the COPM assessment, we found an increase in patient performance scores of +2 points and an increase in patient satisfaction scores by 3 points. Then, the Rehabilitative frame of reference is able to help GBS patients to carry out their daily activities independently with the existence of modification tools or adaptation tools. So, in this study it can be concluded that there is an increase in the ability of patients with Guillain-Barre Syndrome in functional communication activities with occupational therapy management using the Biomechanical and Rehabilitative terms of reference. An occupational therapist can help individuals with GBS using a biomechanical and rehabilitative approach, but providing comprehensive therapy and involving inter collaboration treatment will be able to make better progress for the client’s independence. Therefore, this can be considered as a follow-up to the current therapy program.
References
-
Parry GJ, Stainberg JS (2007) Guillain-Barre Syndrome. United Kingdom: Demos Health.
-
Singh S (2016) Understanding Autoimmune Disease: An Update Review. Kanpur: Pranveer Singh Institute of Technology.
-
Ang CW, Jacobs BC, Laman JD (2004) The Guillain-Barre syndrome: A True Case of Molecular Mimicry. USA: Trends in Immunology 25(2): 61-66.
-
Kakadia N, Pithadia A (2010) Guillain-Barre Syndrome. Gujarat, India: Pharmacological Reports.
-
(2016) American Association of Neuromuscular and Electrodiagnostic Medicine (AANEM). Guillain-Barre Syndrome. USA: AANEM.
-
Kim KW, Kim SS, Lee JS (2011) Clinical Case Study on Guillain-Barre Syndrome Complaining Both Lower Extremity Weakness with Oriental Medical Treatment. Korea: J Korea CHUNA.
-
Hansen M (2016) Guillain-Barre Syndrome Guidelines for Physical and Occupational Therapy. Narberth: GBS/ CIDP Foundation International.
-
Cole MB, Tufano R (2008) Applied Theories in Occupational Therapy: A Practical Approach. USA: SLACK Incorporated.
-
Amudavalli A (2015) Theories and Models of Communication. Chemai: University of Madras.
-
Drago E (2015) The Effect of Technology on Face to Face Communication. USA: The Elon Journal of Undergraduate Research in Communication.
-
American Occupational Therapy Association (2011) Occupation Therapy in Acute Care. USA: American Occupational Therapy Association Incorporated. (2015). Occupation-Based Activity Analysis. 2nd (Edn.), USA: SLACK Incorporated.
-
Leblois A, Narasimhan N (2012) Making Mobile Phones and Services Accessible for Persons with Disabilities. India: The International Telecommunication Union (ITU).
-
Grotberg Edith H (1999) Tapping Your Inner Strength: How to Find the Resilience to Deal with Anything. Oakland, CA: New Harbinger Publications, Inc.
-
Abascal J, Civit A (2000) Mobile Communication for People with Disabilities and Older People: New Opportunities for Autonomous Life. Workshop on Universal Accessibility of Ubiquitous Computing: Providing for the Elderly.
-
Kane S, Jayant C, Wobbrock J, Ladner R (2016) Freedom to Roam: A Study of Mobile Device Adoption and Accessibility for People with Visual and Motor Disabilities. Seattle: University of Washington.
-
Yang SY, Lin CY, Lee YC, Chang JH (2017) The Canadian Occupational Performance measure for patients with stroke: a systematic review. J Phys Ther Sci 29(3): 548- 555.
-
Khazanda FJ, Zameer S (2016) Effectiveness of Occupational Therapy in Rehabilitation of Guillain-Barre Syndrome: A Case Study. Phys Med Rehabil Int 3(2): 1083.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial