Assessment of the Effect of Stretching Quadriceps on Pain and Strength in Patello-Femoral Pain Syndrome
Objective: To assess the effect of eccentric, slow speed, submaximal Quadriceps stretching on the pain and strength of patients suffering from the Patello-femoral pain syndrome (PFPS). Materials and methods: Isokinetic evaluation of the Quadriceps strength before and after stretching the injured knee of the pathological group and the dominant knee of the control group, for 27 patients with PFPS and 12 healthy control subjects. The assessment is carried out with contractions at 60°/s and 120°/s in concentric mode and 30°/s in eccentric mode. A pain assessment by an EVA test is made before and after stretching at each speed of the test on the knee tested for both groups. Results: After the Quadriceps stretching we obtained a decrease in pain of -38% (p<0.017) and an increase in strength of +17% for the pathological group. No significant change in the control group. There is a statistical correlation between the decrease in pain and the gain in strength after stretching (p<0.002). Conclusion: We confirm the effectiveness of performing eccentric, slow speed, submaximal Quadriceps stretching on the PFPS. The beneficial effects suggest that a systematic use of the former is advisable in muscle strengthening. These results confirm the necessity of stretching exercises.
Introduction
The Patello-femoral Pain Syndrome, once diagnosed from amongst the numerous Patello-femoral conditions, is a pathology frequently encountered in sports medicine among young adults. It is characterized by retro patellar pain when in a prolonged sitting position, upon climbing and descending stairs or when in a squatting position [1, 2, 3, 4, 5]. Several non-exhaustive theories have been put forward to try to explain this multifactorial etiology which is generally poorly understood (muscular imbalance, abnormalities in dynamique alignment, overuse of joints, abnormality in cartilage, stiffness of the lateral retinaculum) [6]. This joint must combine biomechanical, static and dynamic requirements due to a lack of bone congruity and the constraints linked to the power generated when carrying out functional tasks.
Passive stability is determined by bone anatomical structure (trochlea - patella) and ligament anatomical structure (medial or lateral), whilst active stability depends on muscle balance (Hamstrings/Quadriceps) as well as passive ligament balance between medial and lateral structures [7, 8].
This is the reason that Numes and Co. [9] in order to diagnose this syndrome, recommend using tests to measure the level of pain (squatting) and also offer guidance on using the tests to find the agonist / antagonist muscle ratio. They also suggest using medical imagery to assist with the diagnosis.
Consequently the medical care and therapy for Patello- femoral pain syndrome, PFPS is still widely debated. There appears to be constant improvement in pain and functionality through physiotherapy treatments, however comparison with a placebo group is rarely carried out [10]. Even though many authors agree in acknowledging the weakness of the Quadriceps/Hamstrings duo and in the need to strengthen it, it is difficult to reach a consensus on the efficiency of any one medical treatment over another [2, 11, 12, 13].
Certain authors recommend medical treatment prioritising muscle strengthening of the Quadriceps in isometric, concentric and eccentric mode, yet proof of its efficiency is still debated [14]. Nevertheless, eccentric muscular work, in isokinetic mode on the Quadriceps for the treatment of PFPS shows a loss of strength in the Quadriceps muscle when the knee is extended (from 30% to 40%, bent between 35° and 60°) [11, 13]. This loss in strength leads to an inappropriate and unbalanced ratio of the agonist/antagonist muscle duo in the knee [1, 3, 8, 9, 15, 16, 17]. According to the authors, this could partly explain the patient’s grievances. Thus, certain studies are oriented towards strategies which more or less associate and combine muscle strengthening exercises, stretching, and/or functional education over periods of 1.5 (6 weeks) to 3 months [2, 12, 18].
The medical treatment for stiffness and the neurophysiological symptoms, which are directly associated with these stiffness phenomena when the syndrome appears, (reduced mobility and joint restriction observed [1, 3, 8].) incite therapists to recommend stretching to recover this physiological range (muscular and in the joints). These stretching techniques enable the loosening and relaxing of the muscles (20), so as to regain maximum joint mobility by analytical postural techniques (19).
Thus the main aim of this study is to measure how stretching the Quadriceps (specifically the Rectus Femoris) affects the pain and the short term recovery of muscular power for patients suffering from PFPS.
Material and Method
Subjects: 2 subject groups have been studied
A Patello-femoral pain syndrome group (PFPS) consisting of 27 patients (16 men and 11 women) aged between 18 and 40 years, suffering from a unilateral Patello-femoral pain syndrome (Table 1). The contralateral knee was exempt from pathology. These patients were taken into the sports medicine department at a hospital and assessed by the PM&R doctor in the department. No imagery was used and assessment was based purely on clinical diagnosis.
Patients included in the study displayed the following symptoms: Pain upon touching the patella. Patella pain when climbing or descending stairs. Pain when in full squatting position. Pain when in a prolonged sitting position.
Exclusion criteria were the following: knee surgery, those suffering from femorotibial or those suffering from bilateral Patello-femoral pain syndrome, since cognitive difficulties prevent tests being carried out successfully in the best conditions.
A group of control subjects (CS) consisting of 12 subjects (5 men and 7 women), of the same age, height, weight, were also selected (Table 1). These subjects, selected according to the characteristics of the PFPS group had neither suffered pathology of nor undergone any prior surgery on either lower limb. The aim was to single out the effects of the stretching and to ensure that the results obtained could not be associated with anything else other than the stretching applied to the knee. Therefore for this control group we proceeded with an assessment of the healthy knee before and after stretching and an assessment of the contralateral knee without stretching.
| Group | Gender | Age | Height | Weight | |
|---|---|---|---|---|---|
| CS | 5M / 7W | 27.58 (5.40) | 170 (0.05) | 62.54 (6.98) | |
| PFPS | 16M / 11W | 30.15 (8.86) | 178 (0.10) | 70.67 (12.44) |
Table 1: Data anthropometric group.
Data regarding age, weight, height and gender for both subject groups (CS= control subjects and PFPS = Patello- femoral pain syndrome) showing the average and the standard deviation.
The stretched knee was considered the knee belonging to the favoured leg. Three tests were carried out: the subject was pushed from behind without prior warning, was then asked to hop on one leg and finally to kick a ball. Each time we made note of the dominant leg and we selected the leg most frequently used first. Each subject or patient, after having been informed of the assessment procedure, signed an informed consent prior to the study. The study was conducted in accordance with the Declaration of Helsinki and approved by the Local Committee for Human Protection (protocol has been realized directly on the sport hospital medical service of hospital La Timone, Marseille).
Material
Pre and post stretching strength assessments as well as the warm up (which is completed before the assessment) are carried out using a Contrex®MJ, isokinetic dynamometer, human kinetics 1.7.4 filter V 1.7.3 in a sports medicine unit.
The factor taken into account during the assessments is the peak torque or point of maximum strength (expressed in Newton-metres, Nm/kg).
In fact, for repeat experiments, the measuring of the peak torque at slow or rapid angular velocity is very reliable with correlation coefficients between 0.93 and 0.99 [21, 22].
Assessment of the Strength Ratio Quadriceps/ Hamstrings
The peak torque in Nm/kg Quadriceps/Hamstrings is recorded at every speed (60°/sec concentric, 120°/sec concentric and 30°/sec eccentric), for both legs in both the pathological and control groups.
These recordings, which have been recognized and approved, are the same as those frequently used in medical documentation [11, 15, 23, 24]. They enable us to assess the deficit in strength of the Quadriceps in the Patello-femoral pain syndrome.
Assessment of Patella Pain
The rating of the patients’ level of pain is carried out in two phases : before stretching and after stretching for each test carried out (isokinetic at 60°/sec concentric, 120°/sec concentric and 30°/sec eccentric).
The assessor asked the patient to rate the patella pain they felt, using a visual analogue pain scale (VAS, 0-100 mm) so as to be able to notice any difference before and after stretching [25]. This assessment is then converted into a score between zero and ten.
Method
Each Subject Observed the Following Protocol
For the pathological group: an assessment of strength and pain on both the injured and contralateral knee before and after stretching on the injured side.
For the control group: an assessment of the strength and pain of both the dominant and contralateral knee before and after stretching the dominant knee.
Experimental Protocol
Position of the subject: the subject sits on a chair raised by 5° horizontally and inclined by 20° vertically (standard position so as to enable a comparable performance between all the subjects) [26]. The patient does not look at the monitor screen so as to avoid an increase from 6.4 to 7.2% in his or her performance due to this factor [27]. The arms are placed straight down the body with the hands gripping the handles. To reduce compensation the subject is held still by two thoracic straps which are crossed to prevent flexing movements from the torso, a pelvic strap to prevent pelvic movements and a femoral strap on the assessed leg to ensure that flexion of each body part occurs independently from the rest. The non-assessed leg is free from all binding and no instructions are given for any particular voluntary movements of the latter. This is so as not to influence the results of the assessed limb [28]. The axis of rotation of the lever arm of the dynamometer coincides with the knee’s axis of rotation (Figure 1).

For the tested leg a support system and one of counter pressure fixed two fingerbreadths above the lateral malleolus holds together the leg area and the lever arm. The range of flexion and extension are defined for all our patients. They will be used for reference during warm-ups and during tests, which have been approved by validated protocols. (GEDRI Group d’Etude pour le Development et la Recherche en Isocinétisme: Study Group for the Development and Research into Isokinetics [29]). The effect of gravity is offset by the dynamometer. Each patient benefits from an isokinetic, bilateral muscle warm-up that always begins on the healthy side.
Representation of rectus femoris and vastus muscle stretching procedure by the physiotherapist (see in the text for more details).
Kues and Co, et al. [24] recommend carrying out one to two sessions of isokinetic contractions prior to the test so as to ensure reliability of the latter. Whilhite and Cohen [30] recommend beginning the test using a slow speed of 60°/sec, carrying out only 5 contractions and then continuing at quick speeds with 6 contractions. Finally according to Croisier [31, 32] the slow speed of 30°/sec for an eccentric test is ideal to enable the patient to familiarise himself with this type of test. Our protocol will therefore be established according to these recommendations. Since the experimental process is more easily carried out on the healthy side, we have followed the same order and the same speeds throughout, as follows: 6 concentric repetitions at 60°/sec Flexor/Extensor 6 concentric repetitions at 120°/sec Flexor/Extensor 3 eccentric repetitions at 30°/sec Extensor The isokinetic test with a visual analogue pain scale (VAS) before stretching The test begins on the healthy side with the following protocol: 4 concentric repetitions at 60°/sec Flexor/Extensor. 5 concentric repetitions at 120°/sec Flexor/Extensor. 2 eccentric repetitions at 30°/sec Extensors only.
Between each series, the patient rests for 30 seconds. Each subject is verbally encouraged yet receives no visual feedback. This protocol is carried out first of all on the healthy side and is then repeated on the injured side. After carrying out the isokinetic tests and assessing the pain, the physiotherapist performs stretching on the Quadriceps of the injured knee whilst following an identical protocol for each patient.
Quadriceps stretching on the injured knee After the test, the patient accompanies the physiotherapist into an adjoining room, which contains a table to carry out the stretching. He explains and demonstrates the protocol by performing the stretching on the healthy leg, that is to say the position and the manipulation method that he will perform on the injured leg.
i. Position of the patient: The patient sits, placing his buttocks on the edge of the table. He then lies down slowly into the supine position, taking hold of his healthy knee with his hands and gripping it. Thus he has his healthy leg bent up against his chest and held by his hands, while his injured leg is hanging off the end of the table from the under crease of the buttock downwards. The specifics of this biarticular muscle require the carrying out of a hip extension stretch first of all, followed by flexion of the knee.
ii. Position of the physiotherapist: The therapist adjusts the height of the electric table so as to bring the patient’s knee to the same height as his anterior superior iliac spine. He then inclines his torso forwards until his thorax presses against the patient’s thigh. The therapist is at this point holding a half spread leg position, his leg flexed forwards, interlocked with the patient’s knee. His outstretched back leg enables him to have a stable stance to resist the patient’s push (Figure 1). However the correct balance can only be reached if the patient’s hemi pelvis is also locked into a stable position. This is essential to avoid the stretch losing efficiency, which could occur if he or she compensates during lateral inflexion with the hemi pelvis on the opposite side to the leg being stretched.
To achieve the correct position, the patient places his or her free healthy foot against the practitioner’s shoulder (the practitioner is in front of the patient). The physiotherapist must then maintain equal pressure by pushing on one side with his torso against the patient’s thigh and on the other side with his shoulder against the patient’s foot. Once the practitioner is locked into a stable position, the actual stretching can begin. The stretching used can be explained in two phases as follows:
iii. 1st phase of stretching: Once the position is reached which produces maximum lengthening of the muscle through extension of the hip and adequate flexion of the knee, the patient is required to perform a static contraction of the Rectus Femoris by raising his knee. The practitioner opposes this movement by inclining his chest forwards to block the upward movement of the knee.
iv. 2nd phase of stretching: Whilst the patient holds the static contraction of the Rectus Femoris, the practitioner bends the patient’s knee very slowly, whilst pushing with his tibia against that of the patient. This is known as eccentric, slow speed, active tension stretching where the patient accepts to have his knee flexed and asserts an opposing force, which is less than that of the practitioner. In fact when the physiotherapist asks the patient to bring his knee up to his chest, the contralateral Rectus Femoris is put under active tension in its role as hip Flexor (proximal insertion of the biarticular head) then, during this active tension, the Quadriceps is stretched in eccentric mode in its role as knee Extensor (distal insertions of the different Quadriceps heads). This stretching is repeated three times for 20 seconds with 20 seconds’ rest between each stretch. This protocol is carried out in the same way on each patient.
Once the stretching is completed, the patient positions himself once again on the isokinetic dynamometer and carries out once more the test of strength, which is identical to the procedure already described and follows the same protocol. There is on average a lapse of three minutes between the 1st and 2nd assessment.
Statistical Analysis
The values are expressed as averages with a standard deviation each time. After having completed tests for normality (Kolmogorov-Smirnov tests), our results are analysed by using a general linear model through repeated observations of multiple analysis of variance (MANOVA). The analysis is based on three factor “groups” (control/ pathological), limb (stretched/ not-stretched), and speed of implementation (60°/s and 120°/s concentric and 30°/s eccentric).
Student’s t-test for non-matched samples was used to check the differences in value between groups or between specific comparisons on the percentages calculated. The statistical significance level is fixed at a value of p <0.05.
Results
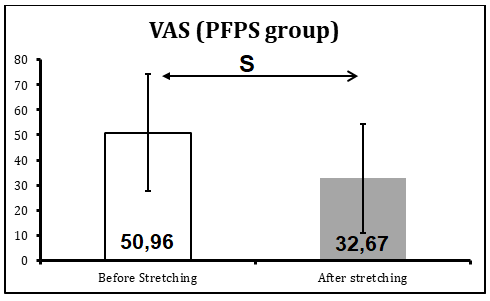
The first factor analysed concerns the pain for our PFPS patients. Our results show a large, statistically significant change with an average decrease of 38% (p<0.005) in pain for the same test at 30°/s eccentric (Figure 2 and Table 2).
| PFPS | |||
|---|---|---|---|
| Stretching | Before | Difference | After |
| 60°Conc | 37.81 | NS | 27.96 |
| 27.33 | 23.03 | ||
| 120°Conc | 30.44 | NS | 23.07 |
| 24.08 | 20.45 | ||
| 30°Ecc | 50.3 | S | 33.67 |
| 27.36 | 25.04 |
Table 2: EVA evaluation.
We notice that before stretching, the pain is always significantly stronger at 30°/s in eccentric mode than at
60°/s and 120°/s in concentric mode (respectively F=3.25, p<0.04 for 60°/s concentric and F= 4.03, p<0.012 for 120°/s concentric versus 30°/s eccentric).
When we compare these same assessments after stretching, we do not find any further significant differences between these concentric or eccentric conditions in terms of the pain factor.
When we compare the results for each situation tested, that is to say that we compare the results before and after stretching, we obtain insignificant results for the comparisons for concentric contractions. The results are significantly different when we compare them before and after stretching for the situation of 30°/s in eccentric mode (F = 3.374, p< 0.017 with a significant decrease in pain of 38% after stretching).
The second factor analysed is the peak strength. In concentric mode at the speeds of 60°/s and 120°/s, we have not found any significant differences for the control group (CS) or for the pathological group (PFPS). This is valid for the values of peak torque and also for the assessments of pain before and after stretching (Tables 2,3).
| PFPS | % | % | CS | % | ||||
|---|---|---|---|---|---|---|---|---|
| PFPS | HK/IK | CS | IK/SIK | HK/SHK | ||||
| 60° Conc. Contr. | HK | IK | SIK | HK | SHK | |||
| Peak Torque Nm/kg | 2.03 | 1.85 | -8.87 | 1.93 | 4.03 | 2 | 2 | 2.56 |
| 0.45 | 0.45 | 0.53 | 0.3 | 0.4 | ||||
| 120° Conc. Contr. | ||||||||
| Peak Torque Nm/kg | 1.56 | 1.47 | -5.76 | 1.53 | 4.08 | 1.5 | 1.5 | 0.6 |
| 0.3 | 0.37 | 0.41 | 0.2 | 0.2 | ||||
| 30° Eccen. Contr. | ||||||||
| Peak Torque Nm/kg | 2.82 | 2.6 | -7.8 | 3.05 | 17.31 | 3 | 3.3 | 8.22 |
| 0.57 | 0.59 | 0.71 | S | 0.6 | 0.6 | S |
Table 3: Isokinetic values before and after stretching.
However, the comparative analysis between the PFPS group and the CS group of the values for strength and pain at 30°/sec in eccentric mode reveal significant differences (Tables 2,3).
Thus for the peak torque, when we compare the values obtained for the healthy limb and the injured limb in the PFPS group, we observe a significant difference 2.84 Nm/KG (+/- 0.48) vs 2.60 Nm/KG (+/-0.52) p<0.002 before stretching. However for the peak torque for the healthy limb in the PFPS group, we do not obtain significantly different values from those of the CS before treatment, even though these values do remain inferior.
The average value of the Quadriceps’ peak torque in the PFPS group increases significantly from 2.6 (+/-0.52) before stretching to 3.05 Nm/Kg after stretching. This is an increase of 0.405 Nm/Kg (p<0.0001), which represents a gain of 17.22%. Our results also show a significant improvement of 8.22% in the CS group in spite of an increase of only +0.246 Nm/Kg (which is equivalent to 3.103 Nm/Kg before stretching the healthy knee and 3.286 Nm/Kg after stretching this same knee). The stretching leads to an increase in the strength developed which is twice as much for the PFPS group than for the CS group.
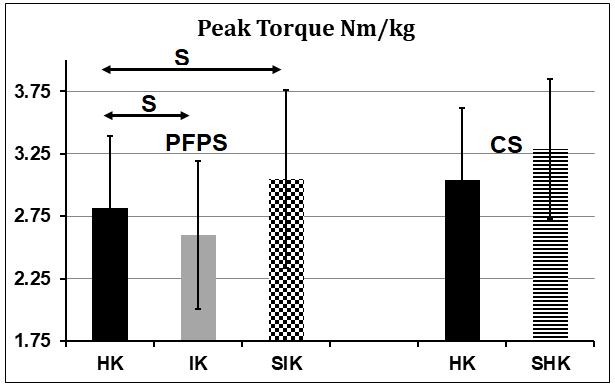
Regarding the peak torque, we observe that the average value obtained for the injured knee for the PFPS group after stretching which is 3.05 Nm/KG (+/- 0.71) is practically identical to the value obtained for the peak torque for the CS group before stretching which is 3.04 Nm/KG (+/- 0.58) (Figure 3). This difference is not significant. Likewise we found no significant difference when we compared the CS group before and after stretching – the stretching exercises do not have a direct effect on peak torque measured when the limb is healthy.
Finally, in the PFPS group when we compare the Quadriceps strength on the injured leg with that of the contralateral leg after stretching, we observe that the values of peak torque are reduced with only a 5% difference (2.90 Nm/KG (+/- 0.83) healthy side vs 3.05 Nm/KG (+/- 0.71) stretched injured side. This difference is no longer significant (p>0.05) and the values tend to be standardised between the two sides, which was not the case before stretching. Moreover we observe that the values are more variable (0.83
vs 0.71) for the healthy leg for the PFPS group.
Graphic representation of improving the sensation of pain by Visual Analogue Scale for PFPS patients (patella- femoral pain syndrome) in position 30 °/s eccentric contraction mode between before and after stretching (S = Significant).
Graphic representation of results obtained in flexion peak torque per body weight kilo (Nm/KG) for the PFPS group (patello-femoral pain syndrome) and the CS group (control subjects). For the Healthy Knee (HK), the Injured Knee (IK), the Stretched Injured Knee (SIK) for the PSFP group or the Healthy Knee (HK) and the Stretched Healthy Knee (SHK) for the CS group, (S= Significant).
Comparison of the difference in pain before/ after stretching (in bold the average, in italics the standard deviation) for the three situations tested in isokinetic mode: 60°/s and 120°/s in concentric contraction mode and 30°/s in eccentric contraction mode (Difference S = significant, NS = non-significant).
This shows a comparison of the isokinetic factors obtained for the peak torque for the Extensors (Ext) or Flexors (Flex) before/after stretching the Rectus Femoris. The values are represented for the PFPS group (Patello-femoral Pain Syndrome) and for the CS group (Control Subject) for concentric mode contractions (Conc. Contr.) at 60°/s and 120°/s and for eccentric mode contractions (Eccen. Contr.) at 30°/s per Kilo of body weight (in bold the average values and in italics the standard deviation). This is for the stretching conditions of the Healthy Knee (HK), the Injured Knee (IK), the Stretched Injured Knee (SIK) for the PSFP group or the Healthy Knee (HK) and the Stretched Healthy Knee (SHK) for the CS group. The variations in the progress obtained after stretching (expressed as percentages), between the knees of the PFPS group and those of the CS group in the different conditions analysed are indicated in bold (S = significant difference).
Discussion
Generally speaking, our results show that performing stretching on the pain has a short-term effect for patients. Thus we observe a significant decrease in pain combined with an increase in strength when eccentric contraction is performed at an exact speed of 30°/s. Our results also show that the stretching has an effect on the control group but that it is significantly lower. The stretching therefore has an influence on the power and strength of the muscle contraction in eccentric mode and also on the initial pain experienced. However our results do not show that there is any effect of stretching on the pain during a concentric contraction.
These results observed which are quantified as short term, can be understood from the neurophysiological point of view, in that they are directly attributable to the stretching itself as well as the muscular ratios Quadriceps/Hamstrings quantified by isokinetics. Usually scientific literature studies the effects of musculotendinous stretching for the prevention or repair of muscle tissue [33, 34, 35, 36] yet the effects of stretching also have an effect on osteo-articular pathologies and can also contribute to the process of rehabilitation. Due to the multifactorial characteristics of the etiology of PFPS, numerous tests have been developed to produce a diagnosis [37]. Neverless, no test is currently recognised as validating the efficiency of the therapeutic treatment. Our view on the effect of stretching can be found in certain works [6, 15, 16, 26, 38].
Thus we recommend active tension stretching of the Rectus Femoris, which does not focus on the contractile tissue (Actin Myosin cross bridges) but on the musculotendinous junction [38]. Active muscular contractions are also altered by short latency loops in segmentary motor reflex: myotatic reflexes, inhibition reflexes 1b or inverse myotatic reflexes, reciprocal inhibition reflexes, the Renshaw cell circuit [34]. Let us remember that inhibition reflex 1b begins in the Golgi receptors, which are found in the junction of the musculotendinous fibers and in the aponeurosis configuration. The purpose of this reflex is to protect the musculoskeletal system against excessively harmful tension [39]. It is therefore beneficial since it stimulates the antagonists, in this case the Hamstrings, which leads to easier flexion of the knee. This is what the practitioner is aiming for [5, 9, 34]. If the practitioner does not require active contraction of the Rectus Femoris, the manoeuvre carried out is simple passive stretching, which is ceased at the patient’s first pain threshold. These biomechanical aspects combined with the articular, capsular and ligamentary characteristics contribute to limiting our patient’s degree of freedom. Thus during the second phase of stretching in our study, the patient performs submaximal opposed resistance exercises with the Vastus Medialis and the Vastus Lateralis. The Rectus Femoris is subjected to active tension stretching whilst the Vastus both undergo submaximal eccentric stretching at slow speed. Controlling when the pain appears is easier in eccentric mode at a slow speed [35, 36] through better synchronisation of the improved motor units as a result of central inhibition on the Renshaw cell circuit [15, 25].
As has been demonstrated by Middleton [29], the effects of submaximal eccentric work at a slow speed are efficient as a technique in gaining articular amplitude.
Furthermore other authors [9, 40] have shown that the level of reflex excitability (the relationship between H/M, H being Hoffman’s reflex response and M being the locomotive response) is lower after passive stretching combined with isokinetic eccentric work is performed on the triceps sural. This decrease by way of a reduction in the response H, which is equivalent to a decrease in muscle tone and in osteo- tendinous reflex, is increased during eccentric work [9, 40]. Eccentric exercises and passive stretching affect the same texture (connective tissue in the muscle) [20]. It therefore seems likely, as the previously mentioned authors believe, that they affect tissue in the same way (notably an effect on the cytoskeleton of muscle fibre).
1) Regarding muscles, eccentric work reduces reflex muscle contractions, which contribute to articular stiffness [31, 23]. In the framework of the PFPS study, we often notice this stiffness in the knee along with a blocked feeling in the patella during acute attacks. In this case, eccentric work would be efficient due to its effect on decreasing articular stiffness [28, 5] and it could also reach 7° for ankle dorsiflexion [36]. The initial level of pain being high, bringing a positive change to the latter would therefore be made easier. Even though this study concerns the ankle, we can consider that these mechanisms are also applicable to the knee.
2) Regarding the spinal cord, the sum of sensitive information linked to voluntary muscle movement and muscular contraction inhibits nociceptive integration [35]. The authors specify that in this case, the inhibition of the myotatic reflex originating from the Golgi tendon organs would be even stronger.
This process is part of the efficient adaptability of the organization of motor synergies. Neuronal systems involved in the organization of motor synergies are complex and this includes the spinal locomotor generators, sensory feedback, presynaptic inhibitions, recurrent inhibitions as well as systems descending from supraspinatus structures [35, 41]. Passive stretching is believed to have the distinct characteristics of reducing maximum strength, which is potentially traumatic [42] and of enabling the patient to recover functional motor function when it comes to physiological muscle components and also the programming of the neurological motor components [36].
The authors have demonstrated this in the gastrocnemius muscle over a period of 4 weeks’ of stretching exercises. Eccentric stretching at slow speed stimulates a progressive increase in the strength developed up to a point close to that of maximum stretch [26, 34]. Even though it is difficult for the subject to reach his or her maximum voluntary strength, it is observed that maximum strength in eccentric mode is superior to that in static or concentric mode [14, 30, 43, 44]. As for concentric work, this essentially uses muscular contractive tissue. The strength produced during eccentric work originates partly from contractile elements, which is essentially due to the resistance of the supporting connecting tissue to the stretching [34, 17]. This stretching is held for 20 seconds and repeated three times consecutively and it logically stimulates the improvement in the eccentric strength of the Quadriceps obtained from our results.
The different adaptable mechanisms that have been put forward to explain this increase in strength after stretching are essentially: better recruitment of the motor units through an increase in their discharge frequency and better synchronisation in their recruitment. These two factors must be developed simultaneously [40]. This is something, which could explain the increase in peak torque after stretching, as is observed after strength training [45]. Thus in pathologies of articular instability, preliminary stretching enables the reinforcing of the muscle strengthening work and the isokinetic eccentric exercise could help the patient to better control the potentially harmful movement [5].
Various studies have shown that there is a link between the decrease in strength and in EMG activity at the start of Quadriceps flexion in eccentric mode for patients with painful knees or those suffering from PFPS. When the Patello-femoral is put under excessive strain, causing an increase in the painful symptomatology this is believed to produce selective inhibition of the Quadriceps. However eccentric work leads to numerous structural adaptations and especially a change in muscle typology. We observe an increase in type II fibres and a decrease in type I fibers [46]. So is the strength gain linked to the decrease in pain or the specifics of the stretching in eccentric mode? The answer can be found in the analysis of the strength gain in the control group who undergo this stretching on a painless knee. The latter acquire a significant gain in strength of 8.22% when we compare their healthy limb before stretching and the same limb after stretching (this knee benefits from the effects of stretching) but the gain is less significant when compared to that of 17.31% for the stretched knee of the pathological group. We believe that it is the specifics of the eccentric mode work, which encourage the increase of the maximum voluntary strength and that it really is this factor, which contributes to the recovery of strength. The decrease in the pain factor observed in our results enables us to make use of this achievement by carrying out eccentric work. Likewise, performing eccentric exercise on the muscle groups, which have an inhibitory effect on the movement, would appear to be an ideal prevention measure [38, 47]. Nevertheless, this improvement only appears to be possible and achievable in accordance with a neurological phenomenon combined with the rise in inhibition of the pain factor (patella pain) [36]. In view of our results, the gain in strength appears to be achieved through the effects of the mechanical properties (increased muscular tension) and the neurological properties (pain inhibition) of eccentric mode stretching.
Consequently, as stated by Konrad and Tilp, et al. [35] tolerance to the stretching, probably due to the adaptation of the nociceptive nerve endings, appears to be the main explanation for the strength gain obtained in our results. We should bear in mind that as far as these authors are concerned, it is impossible to modify short term the structural framework of the muscle/ tendon unit [35, 36].
Moreover, in our study, patients have undergone stretching three times for 20 seconds with a 20-second rest between each series. There is on average a three-minute gap between the stretching and the test of strength; it would be wise to carry out tests every ten minutes taking into account the signs of tiredness. Middleton [29] during his experiment in using eccentric contraction as a technique for range gain in the Rectus Femoris, carries out 50 submaximal isokinetic repetitions at slow speed on a patient suffering from a hip flessum. These satisfying results seem to confirm the importance of a significant number of repetitions. It appears suitable to recommend to the patient-physiotherapist duo to carry out 5 consecutive stretching exercises per physiotherapy session, which would enable them to complete 50 stretches in 10 sessions. Repetition could be an important factor in obtaining lasting wellbeing (neuromechanical) in the PFPS pathology. These differences could be due to the total stretching time, which varies from study to study, or the intensity of the stretching which is difficult to standardise [36]. It is considered that new studies, which alter the duration, the number of stretches, as well as the recovery time, could give us just as much informative information to confirm the relevance of our results. This study is of particular interest to sports doctors, physiotherapists and sports coaches, yet in the absence of other similar studies, it would seem wise to wait for new experiments so as to be able to draw more significant conclusions.
Conclusion
The stretching techniques suggested enable an improvement in motor performance, in terms of power during eccentric work, combined with a decrease in painful phenomena, which is always detrimental to rehabilitation medical care. The gain in strength observed is linked to the choice of eccentric submaximal stretching at slow speed, which enables better control of the pain and minimal consequences of the latter during motor activities. So as to fully benefit from the effects of the stretching, it seems advisable to perform it at the beginning of the rehabilitation session, so as to maximise the effectiveness of the functional treatment. Likewise preparation in eccentric mode of the muscle groups, which have an inhibitory effect on the movement, would appear to be an ideal preventive treatment solution. There is currently a consensus in PFPS rehabilitation, in that it must include strengthening and relaxing of the Quadriceps, especially if the latter displays signs of stiffness. Regarding the medical care for this pathology, our results show the importance of these specific stretching exercises to treat stiffness and to facilitate better quality muscle strengthening.
References
-
Callangh MJ, Odham JA (1996) The Role Of Quadriceps Exercise In The Treatment Of Patello-Femoral Pain Syndrome. Sports Med 21(5): 384-391.
-
Clarck D, Downing N, Mitchell J, Coulson L, Syzpryt E, et al. (2000) Physiotherapy for anterior knee pain: a randomized controlled trial. Ann Rheum Dis 59(9): 700- 704.
-
Kannus P, Niitymaki S (1994) Witch factor predict outcome in the non-operative treatment of patello- femoral pain syndrome. Med Sci Sporst Exerc 26: 289- 96.
-
Rugg S, Gregor R, Mandelbaum B, Chiu L (1990) In vivo momento arm calculations at the ankle unsing magnetic resonance imaging (MRI). J Biomech 23(5): 495-501.
-
Simic L, Sarabon N, Markovic G (2013) Does pre-exercise static stretching inhibit maximal muscular performance ? A meta analytical review. Scand J Med Sci Sports 23(2): 131-148.
-
Cook C, Mabry L, Reiman M, Hegedus E (2012) Best test/clinical findings for screening and diagnosis of patellofemoral pain syndrom : a systematic review. Physiotherapy 98(2): 93-100.
-
Dejour H (2006) Les syndromes femoro-patellaires, diagnostic, facteurs d’instabilite rotulienne et classification. Medecin du Sport 78: 36-42.
-
Thommee R, Augustsson J, Karlsson J (1999) Patello- femoral pain syndrome: a review of current issues. Sports Med 28(4): 245-262.
-
Middleton P, Montero C (2004) Eccentric muscular contraction : implications in treatment of athletes. Ann Readapt Med Phys 47(6): 282-289.
-
Crossley K, Bennell K, Green S, McConnell J (2001) A systematic review of physical interventions for patellofemoral pain Syndrome. Clin J Sport Med 11(2): 103-110.
-
Bennet JG, Stauber WT (1986) Evaluation and treatment of anterior knee pain using eccentric exercise. Med Sci Sports Exerc 18(5): 526-530.
-
De Broucker MJ, Gougeon F (1996) Reeducation isocinetique excentrique des syndromes routines. Masson Ed, Paris 252-255.
-
Edouard P, Degache F, Calmels P (2009) Intérêt du travail musculaire excentrique dans le treatment des syndromes douloureux femoro-patellaires. Exercise musculaire excentrique. Masson (Edn.),Paris pp: 113-119.
-
Heintjes E, Berger MY, Bierma-Zeinstra SM, Bernsen RM, Verhaar JA, et al. (2003) Exercise therapy for patella- femoral pain syndrome. Cochrane Data Base Syst Rev (4): CD003472
-
Dvir Z, HalperinN, Shaklar A, Robinson D (1991) Quadriceps functions and patello-femoral pain syndrome. Part 2: The break phenomen during eccentric activity. Isokinetics and Exercise Science 1: 31-35.
-
Kvist J, Gillquist J (2001) Sagittal plane knee translation and electromyography activity during closed and opened kinetic chain exercises in anterior cruciate ligament- deficient patients and control subjects. Am J Sport Med 29(1): 72-82.
-
Tang SF, Chen CK, Hsu R, Chou SW, Hong WH, et al. (2001) Vastus medial is obliqus and Vastus lateralis activity in open and closed kinetic chain exercises in patients with patellofemoral pain syndrome: Arch Phys Med Rehabil 82(10): 1441-1445.
-
Dupont Y (2003) Pathologie douloureuse femoro- patellaires. Analyse et classification. Knee surgery in sports Traumatologie and Arthroscopy pp: 52-56.
-
Guissard N, Duchateau J (2004) Effect of static stretch training on neural and mechanical properties of human plantar–flexor muscles. Muscle and nerve 29(2): 248- 255.
-
Prévost P (2005) Les étirements interets et limites dans les pratiques sportives. Physio Sport News. 4: 7-15.
-
Calmels P, Abeilon G, Domenach M, Minaire P (1991) Fiabilite et reproductibilité des mesures de la force isocinetique. Isocinetisme et médecine de rééducation, Masson Ed, Paris pp: 26-34.
-
Hill A: First and last experiments in Muscle Mechanics. Cambridge University Press; 1970.
-
Kramer J (1994) Reliability of absolute and ratio in assessment of knee extensor and flexor strength. Isokinetic Exerc Sci 4: 51-57.
-
Kues JM, Rothstein JM, Lamb RL. (1992) Obtening reliable measurement of knee extensors torque produced during maximal voluntary contractions an experimental investigation. Phys Ther 72(7): 492-501.
-
Jensen MP, Karly P, Braver S (1986) The measurement of clinical pain intensity: a comparison of six methods. Pain 27(1): 117-126.
-
Dvir Z (1991) Clinical applicability of isokinetics: a review. Clinical Biomechanics 6(3): 133-144.
-
Kellis E, Baltzopoulos V (1996) Resistive eccentric exercise: effects of visual feedback on maximum moment of knee extensors and flexors. J orthop Sports Phys Ther 23(2): 120-124.
-
Kang SW, Na YM, Moon JH, Chun SI, Yoon YR, et al. (1997) Interlimb interaction and stabilization of controlateral leg in isokinetic knee evaluation. Arch Phys Med Rehabil 78(5): 497-500.
-
Middleton P (1995) Notre experience du travail excentrique comme technique de gain amplitude: indications et résultats. ANMSR 4-9.
-
Wilhite MR, Cohen ER, Wilhite SC (1992) Reliability of concentric and eccentric measurements of quadriceps performance using Dynamometer: the effect of testing order for three different speeds. J Ortho Sports Phys Ther 15(4): 175-182.
-
Croisier JL, Crielaard JM (2000) Hamstring muscle tear with recurrent complaints: an isokinetic profile. Isokin Exerc Sci 8: 175-180.
-
Croisier JL. L’équilibre des forces musculaires agonists/ antagonists. In Preventions des troubles musculo- squelettiques chez le sportive. Saur amps Medical Ed Montpellier 2013. 72-73.
-
Brassine E, Mouraux D (2013) Les étirements. in Prevention des troubles musculo-squelettiques chez le sportive. Saur amps Medical, Ed Montpellier pp: 39-42.
-
Duchateau J, Enoka RM (2008) Neural control of shortening and lengthening contractions: influence of task contraints. J Physiol 586(24): 5853-5864.
-
Konrad A, Tilp M (2014) Increased range of motion after static stretching is not due to changes in muscle and tendon structure. Clin Biomech 29(6): 636-642.
-
Nakamura M, Ikezoe T, Takeno Y, Ichihashi N (2012) Effects of 4 week static stretch training program on passive stiffness of human gastrocnemius muscle tendon unit in vivo. Eur. J Appl Physiol 112(7): 2749-2755.
-
Numes G, Stapait E, Kirsten M, Noronha M, Santos G, et al. (2013) Clinical test for diagnosis of patellofemoral pain syndrome : systematic review with meta-analysis. Physical therapy in sport 14(1): 54-59.
-
Edouard P, Samozino P, Julia M, Gleizes Cervera S, Vanbierviliet W, et al. (2011) Reliability of isokinetic assessment of shoulder rotator strength : a systematic review of the effect of position. J Sport Rehabil 20(3): 367-383.
-
Gabriel D, Kamen G, Frost G (2006) Neural adaptations to resistive exercise : mechanisms and recommendations for training practices. Sports Med 36(2): 133-149.
-
Remaud A, Guevel A, Cornu C (2007) Antagonist muscle captivation and muscle inhibition : effects on external torque regulation and resistance training induced adaptations. Clinical neurophysiology 37(1): 1-14.
-
Windhorst U (2007) Muscle proprioceptive feedback and spinal networks. Brain Research Bulletin 73(4-6): 155-202.
-
McHugh M, Cosgrave C (2010) To stretch or not to stretch: the role of stretching in injury prevention and performance. Scand J. Med Sci Sports 20(2): 169-181.
-
Enoka RM (1996) Eccentric contractions require activation strategies by the nervous system. J Appl Physio 81(6): 2339-2346.
-
Reid DC (1993) The myth, mystic and frustration of anterior knee pain. Clin J Sport Med 3: 139-143.
-
Zehr P (2002) Considerations for use of the Hoffmann reflex in exercice studies. Eur J Appl Physiol 86(6): 455- 468.
-
Guilhem G, Cornu C, Guevel A (2010) Neuromuscular and muscle-tendon system adaptation to isotonic and isokinetic eccentric exercise. Ann Phys Rehabil Med 53(5): 319-341.
-
Piva S, Fitzgerald K, Wisniewski S, Delitto A (2009) Predictors of pain and function outcome after rehabilitation in patients with patellofemoral pain syndrome. J Rehabil. Med 41(8): 604-612.
-
Herbert L, Gravel D, ArsenaultA, Tremblay G (1994) Patellofemoral pain syndrome: the possible role of an inadequate neuromuscular mechanism. Clin Biomech 9(2): 93-97.
-
Pocholle M, Codine P (1991) Rééducation des ligamentoplasties. Choix d’un protocole isocinetique. Ann Kinesither 18(7): 363-368.
-
Wikstrom E, Tillman M, Chmielewski T, Borsa P (2007) Measurement and evaluation of dynamic joint stability of the knee and ankle after injury. Sports Med 36(5): 393-410.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial