Phenotypes Identification and Physiotherapy Decision-Making Algorithm for the Conservative Non-Pharmacological Treatment of Knee Osteoarthritis: A Scoping Review
Purpose: Knee osteoarthritis phenotype research is an emerging area of study that has not yet matured or led to any major discoveries with significant implications in the clinical setting. We aimed to systematically summaries knee osteoarthritis phenotypes and recommended non-pharmacologic interventions, and to develop a clinically applicable algorithm that categorizes patients with knee osteoarthritis based on phenotypes, thereby making management easier and more effective. Methods: We conducted a main systematic literature search in publication databases (PubMed and Cochrane). Subsequently, a secondary search in PubMed for recommendations, guidelines, or consensus regarding the non-pharmacologic treatment of knee osteoarthritis was conducted. Our findings were then used to develop an algorithm for the effective, conservative, nonpharmacological treatment of knee osteoarthritis. Results: Five phenotype categories, including neuropathic, local, psychological, high body mass index, and comorbidities were identified. Secondly, we summarized the most recommended interventions, including strengthening, aerobics, education, mind-body, neuromuscular training, flexibility, aquatic exercise, psychological, and walking aids. We subsequently created an algorithm with sixteen phenotypes. Conclusions: We systematically reviewed all eligible studies that aimed to identify knee osteoarthritis phenotypes, and summarized all non-pharmacological interventions mentioned in the relevant literature. Further, we opine that each rehabilitation programme should be tailored to each patient’s particularities or phenotype at the least. Further, we provide a unique algorithm based on critical reasoning to assist decision-making in conservative non-pharmacological treatment of knee osteoarthritis pain. In the detailed and well-structured treatment for knee osteoarthritis patients, phenotype identification is essential. We suggest the adoption of this algorithm into daily clinical practice.
Introduction
Knee osteoarthritis (KOA) is a leading burden on the elderly population. The disease is characterized by pain and a reduction in an individual’s function. As a consequence, quality of life is decreased and psychological disorders such as depression, anxiety, and helplessness might occur.
The determination of the pathology by only the amount of damage shown on an X-ray is not a valid option because of the discordance between pain and imaging [1, 2, 3, 4, 5]. Furthermore, the correlation between pain associated with pathology and the central nervous system has been suggested [6]. Additionally, psychological factors might contribute to pain and would therefore need to be addressed, if present, through an individualized and multidimensional rehabilitation programme [7, 8]. The fact that pain might persist even after a total replacement of the joint [9] confirms the contribution of non-local factors to pathological pain.
The multifactorial nature of KOA suggests the need to divide sufferers into various phenotypes [10, 11, 12]. The initial phenotypes vary between studies; however, all studies identify local-biological, psychological, and neuropathic indicators. International guidelines [13, 14] recommend exercise as the most effective non-pharmacological intervention. Psychosocial interventions, individually or combined with exercise, are recommended by guidelines [13, 14] further confirming the need for individualized and multidirectional interventions.
The word phenotype is often used loosely and incorrectly in the literature. Thus, in this text, the phenotype will refer to the observable and measurable characteristics that can be present in a KOA patient. The need to identify KOA phenotypes has previously been reported. The literature suggests a variety of phenotypes [10, 15, 16, 17]. While KOA phenotypes have been identified previously, none of those studies provided further information in an effort to bridge the gap between phenotypes identification and clinical implementation. Therefore, to the best of our knowledge, this is the first study that provides a logical evaluation procedure that sorts the patients into phenotypes and simultaneously suggests the most appropriate treatment.
The first aim of this umbrella review was to summarize KOA phenotypes and suggest a classification. Second, we aimed to systematically summarize all the suggested treatments provided by the relevant literature. Finally, based on our results and the authors’ critical opinion, we intended to suggest a logically structured algorithm that allows the clinicians to identify each patient’s phenotype and the most suitable intervention.
Methods
To identify any eligible studies, two searches were conducted, with the first regarding KOA phenotypes and the second aiming to collect evidence of the most suggested interventions concerning KOA.
Search strategy
We conducted a systematic search of the literature from database inception to 1 July 2020. To identify studies that divide KOA into clinical phenotypes, two authors systematically reviewed PubMed and The Cochrane Library. Our research was restricted to English language publications, but no date restriction was applied. The search was performed using the Boolean operators AND, OR, parentheses, and quotation marks, and adjustments were made as needed to match database particularities. A table with keywords and their possible synonyms was created and divided using the word ‘OR.’ Then, the subgroups of keywords were combined using the word ‘AND.’ The keywords used concerning phenotype identification was as follows: knee osteoarthritis OR knee degeneration OR knee pain OR knee degenerative disease AND phenotype OR classification OR sub group OR clinical AND Systematic review OR Review. To achieve the aims of the study, a supplementary second search was conducted in PubMed with the following keywords: knee osteoarthritis OR knee degeneration OR knee pain OR knee degenerative disease AND intervention OR exercise OR training OR treatment OR rehabilitation AND consensus OR guideline OR recommendation. Both searches were applied in the title field of the database. References of each eligible study were screened to identify any further sources. We did not search through grey literature.
Eligibility criteria
All identified publications went through a three-step parallel review of the title, abstract, and full text, performed independently by two authors, based on predefined inclusion and exclusion criteria. To identify the included studies for the umbrella review, the PICOS criteria were used. Thus, to match the inclusion criteria, the study needed to: include subjects with a diagnosis of KOA (P); search the literature for KOA phenotypes (I); not require a comparator (C); consider phenotype classification as an outcome measure (O); and be a systematic review or meta-analysis (S). For the needs of the intervention effectiveness search, the included studies needed to follow the PICOS criteria as follows: concern KOA (P); evaluate the effectiveness of any intervention (I); no comparator was required (C); suggestions regarding interventions were considered as the outcome (O); and be a consensus, guideline, or recommendation study type.
Data Extraction and Methodological Quality Assessment
Data extraction was performed independently by two investigators, and in case of discrepancies, the final decision was reached after discussion with a third investigator. To minimize the risk of bias in the review process, a standardized data extraction tool was employed [18]. For the phenotype review, the following data were extracted from the included studies: citation details; objectives of the included review; type of review; details of the participants, setting, and context; the number of databases sourced and searched; the date range of database searching; the publication date range of studies included in the review that inform each outcome of interest, number of studies, types of studies and country of origin of studies included in each review; instrument used to appraise the primary studies and the rating of their quality; outcomes reported that are relevant to the review question; method of synthesis/analysis employed to synthesize the evidence; and comments or notes the review authors may have regarding any included study.
To summarize the effectiveness of each intervention through our secondary search, a table was created and independently completed by each investigator. The citation details and interventions were extracted for this table.
To assess the methodological value of each study, we used the ROBIS tool [19]. ROBIS is a rigorously developed tool designed specifically to assess the risk of bias in systematic reviews. The tool is completed in three phases: assess relevance (optional); identify concerns with the review process; and judge the risk of bias in the review. Signaling questions are included to help assess specific concerns about potential biases within the review. The ratings from these signaling questions help assessors to judge the overall risk of bias.
Intervention Effectiveness-Grading System
To define the value of each intervention, we agreed to give each intervention recommended or strongly recommended one point (+1). An intervention conditionally recommended was valued for half a point (+0.5) per time found. The total value of intervention was reduced by one point (-1) for every recommendation against, and by half a point (-0.5) if the effectiveness was reported as inconclusive. After the total of each intervention was found, an overall recommendation was given by the authors of this paper. An intervention was recommended if the total score ranged from nine to twelve, conditionally recommended if its total was within five and eight, and a recommendation against was given if the score was equal or lower than 4.
Results
Literature Search
Concerning the main search of our study, phenotypes identification, our literature search identified a total of 179 articles, of which 39 were from PubMed and 140 from Cochrane Library. Concerning the summarization of the most recommended non-pharmacological interventions, our literature search identified 372 articles in PubMed. After removing duplicates and excluding articles based on the title and abstract, we identified two articles concerning phenotypes [10, 20] and fourteen concerning interventions [13, 14, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32] eligible for inclusion. Further details regarding the studies’ identification process are illustrated in the appendix (Appendix 1-6).
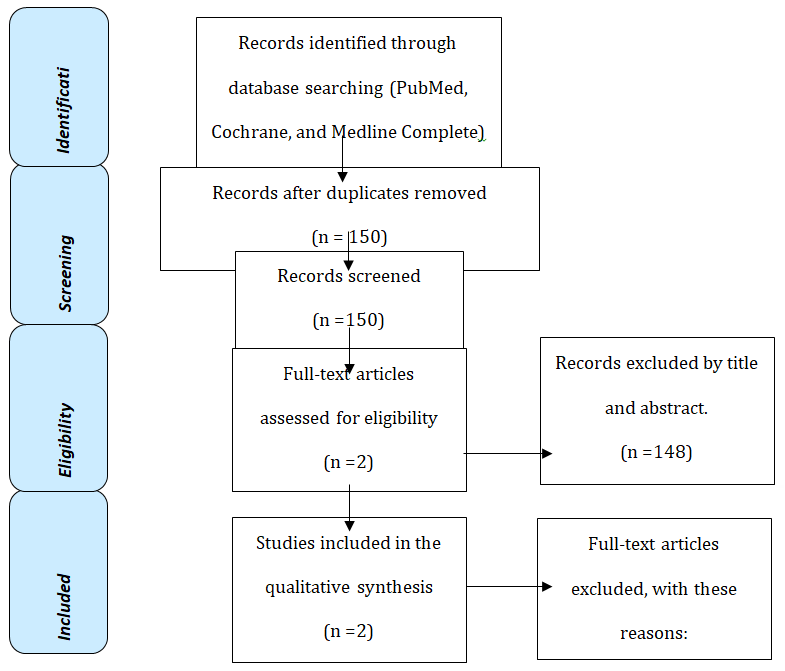
Appendix 1: Study flow chart (PRISMA)
| Signalling question | Reference | [10] | Judgement | [16] | Judgement |
|---|---|---|---|---|---|
| Phase 2 | Low concerns | Low concerns | |||
| 1.1 | Y | Y | |||
| 1.2 | Y | Y | |||
| 1.3 | Y | Y | |||
| 1.4 | Y | Y | |||
| 1.5 | Y | Y | |||
| 2.1 | Y | Low concerns | Y | Low concerns | |
| 2.2 | Y | Y | |||
| 2.3 | Y | Y | |||
| 2.4 | Y | Y | |||
| 2.5 | Y | Y | |||
| 3.1 | Y | Low concerns | Y | Low concerns | |
| 3.2 | Y | Y | |||
| 3.3 | Y | Y | |||
| 3.4 | Y | Y | |||
| 3.5 | Y | Y | |||
| 4.1 | Y | Low concerns | Y | Low concerns | |
| 4.2 | Y | Y | |||
| 4.3 | Y | Y | |||
| 4.4 | Y | Y | |||
| 4.5 | Y | Y | |||
| 4.6 | Y | Y | |||
| Phase 3 | Low risk of bias | Low risk of bias | |||
| A | Y | Y | |||
| B | Y | Y | |||
| C | Y | Y |
Appendix 2: methodological quality assessment.
| Keyword | PubMed | Cochrane |
|---|---|---|
| Knee osteoarthritis | Knee pain, knee degenerative. | |
| Phenotype | Classification, sub group, clinical. | |
| Systematic review | Review. | |
| #1 AND #2 AND #3 | ((((knee osteoarthritis[Title/Abstract])) OR (knee pain[Title/Abstract])) OR (knee degenerative[Title/Abstract]) AND (systematicreview[Filter])) AND (((((phenotype[Title/Abstract]) OR (subgroup[Title/Abstract])) OR (sub- group[Title/Abstract])) OR (subtype[Title/ Abstract])) OR (sub-type[Title/Abstract]) AND (systematicreview[Filter])) | knee osteoarthritis in Title Abstract Keyword OR knee pain in Title Abstract Keyword OR knee de- generative in Title Abstract Keyword AND phe- notype in Title Abstract Keyword AND subgroup OR sub-group OR subtype OR sub-type in Title Abstract Keyword – (Word variations have been searched) |
| Total reviews | 39 | 140 |
| Keyword | PubMed | |
| Knee osteoarthritis | Knee degeneration, knee degenerative disease. | |
| Intervention | Exercise, training, rehabilitation, treatment | |
| Study type | Consensus, guideline, recommendation. | |
| #1 AND #2 AND #3 | ((((knee osteoarthritis[Title/Abstract]) OR (knee pain[Title/Abstract])) OR (knee degenerative[Title/Abstract])) AND (((((intervention) OR (exercise)) OR (training)) OR (treatment)) OR (rehabilitation))) AND (((consensus[Title/Abstract]) OR (guideline[Title/Abstract])) OR (recommendation[Title/Abstract])) | |
| Total | 372 | |
Appendix 3: Phenotypes search.
Appendix 4: Interventions effectiveness search.
| Citation Details | [10] | [16] |
|---|---|---|
| Objectives Of The Included Review | Koa Phenotypes Identification | Koa Phenotypes Identification |
| Type Of Review | Systematic Review | Systematic Review |
| Participant Details | Koa Population | Koa Patients |
| Setting And Context | Community-Based Setting | |
| Number Of Databases Sourced And Searched | 1 | 4 |
| Date Range Of Database Searching | 01/01/1984 To 29/04/ 2016 | Inception To September 2016 |
| Publication Date Range Of Studies Included In The Review That Inform Each Outcome Of Interest | 2000-2015 | 2007-2016 |
| Number Of Studies, Types Of Studies And Country Of Origin Of Studies Included In Each Review | Patients Aged 18 Years Or Older With Koa | 8 Retrospective, 20 Cross-Sectional Design And 6 Cohort |
| Instrument Used To Appraise The Primary Studies And The Rating Of Their Quality | Adaption Of The Standardized Hayden Score | Downs And Black Instrument |
| Outcomes Reported That Are Relevant To The Umbrella Review Question | 6 Phenotypes | 7 Phenotypes |
| Method Of Synthesis/Analysis Employed To Synthesize The Evidence | Qualitative Synthesis | Descriptive Synthesis |
| Comments Or Notes The Umbrella Review Authors May Have Regarding Any Included Study | 6 Clinical Phenotypes | Significant Heterogeneity Across The Studies In The Selection Of Participants And Characteristics And Methods Used To Investigate Knee a Phenotypes |
Appendix 5: standardized data extraction tool.
| Reference | Interventions (namely) | |||
|---|---|---|---|---|
| Recommended | Conditionally | Against | Inconclusive | |
| [32] | Aerobic, strengthening, patient education, flexibility, Tai chi, aquatic exercise. | Therapeutic modalities (heat, cold, sound, and electricity) | ||
| [31] | Aerobic, strengthening, flexibility, functional exercises, gait training, patient education | Proprioception, balance, behavioral, manual therapy, taping (patello- femoral OA), aquatic exercise, balneotherapy, TENS, heat, cold. | Massage, ultrasound, electrotherapy, electromagnetic field, laser therapy, | |
| [21] | Self-management programs, strengthening, low-impact aerobic exercises, neuromuscular education, engage in physical activity consistent with national guidelines. | Acupuncture, lateral wedge insoles, | Physical modalities, manual therapy, valgus directing force brace (medial compartment unloader) | |
| [30] | Education, self-management, strengthening, aerobic | thermotherapy (heat or cold), manual therapy (manipulation and stretching), TENS, footwear, bracing (instability), assistive devices (walking sticks) | acupuncture | |
| [29] | Education (goals and lifestyle changes), thermotherapy (heat or cold), flexibility- stretching-strengthening program, daily walk, aerobic, strengthening (concentric), insoles, knee brace, assistive device (walking stick) | hydrotherapy (without swelling or stiffness) | Mechanotherapy (flexibility- mobilization- stretching) | |
| [26–28] | Aerobic, strengthening, ROM, stretching, manual therapy, home exercise program, patient education, heat, cold after, taping (patella-femoral OA), coordination exercises, balance, motor control, gait training. MDT, mind-body (Hatha Yoga, Tai Chi Qigong, Sun style Tai Chi) | |||
| [25] | cardiorespiratory fitness, muscle strength, flexibility and neuromotor performance (balance, agility, coordination and gait, proprioceptive exercise, Tai Chi, Yoga) |
| [23] | Education, strengthening, aerobic, proprioceptive exercises, electrotherapeutic agents with analgesic properties (TENS), Physical agents with superficial heating (hot-packs, infrared, etc.) and deep heating (ultrasound, short- wave diathermy) property (patients without active synovitis). Superficial cold (active synovitis), Balneotherapy, Assistive and adaptive devices, neuropathic treatment. | Aquatic exercise, Tai Chi | ||
|---|---|---|---|---|
| [22] | Psychological and Social Support, Ultrashort Wave Therapy, Medium- and Low-Frequency Electric Therapies (TENS), Ultrasound Therapy, Shockwave Therapy, Infrared Treatment and Magnetic Therapy, Millimeter Wave Therapy, Patient education, muscle strengthening, aerobic, Spa, Application of Walking Aids. | |||
| [24] | Land-based exercise, muscle strengthening, stretching/range of motion, aerobic conditioning, neuromuscular/balance, cycling, Tai Chi and yoga | Cognitive behavioral therapy, Stationary cycling and Hatha yoga, aquatic exercise, massage, manual therapy, heat therapy, assistive walking device, TENS, | Cold therapy, Valgus unloading braces, footwear, kinesiotaping, electrotherapy, therapeutic ultrasound, acupuncture, | Self- management, Varus unloading knee braces, shoe orthotics, patella taping, Pulsed electromagnetic/ shortwave therapy, |
| [14]Hip, and Polyarticular osteoarthritis (OA | Arthritis Education, Structured Land-Based Exercise Programs (Type 1- strengthening and/or cardio and/or balance training/ neuromuscular exercise, Type 2- Mind- body Exercise including Tai Chi or Yoga) | Aquatic exercise, gait aids, self-management, Cognitive behavioral therapy | ||
| [13] | Exercise (walking, strengthening, neuromuscular training, and aquatic exercise), self-efficacy/management programs, Tai chi, cane, brace (tibiofemoral) | Heat, therapeutic cooling, cognitive behavioral therapy, acupuncture, kinesiotaping, balance training, brace (patellofemoral), Yoga, radiofrequency ablation | TENS, manual therapy, massage, modified shoes, wedged insoles, pulsed vibration therapy |
Appendix 6: interventions through guidelines/recommendations or consensus search.
Studies’ Characteristics
As presented in Appendix 2, both included articles concerning KOA phenotypes were systematic reviews and included KOA patients. The authors of the first study [10] searched one database from inception to 2016 and identified six clinical phenotypes. In the second study [20] the authors searched four databases from inception to 2016 and identified seven phenotypes.
Methodological quality
Two authors independently assessed the methodological quality of each study, and a consensus was reached through discussion. Both assessed systematic reviews were evaluated as low risk of bias. The study evaluation is presented in Appendix 2. We did not perform a quality assessment of the secondary search identifying studies due to type.
Phenotypes
In the first included systematic review [10] six phenotypes were identified, including chronic pain, inflammatory, metabolic syndrome, bone and cartilage metabolism, mechanical overload, and minimal joint disease. In the second eligible review [16] seven phenotypes were identified, including pain sensitization, psychological distress, radiographic severity, body mass index (BMI), muscle strength, inflammation, and comorbidities.
Interventions
After summarizing all mentioned non-pharmacologic interventions through relevant guidelines/recommendations or consensus, we created a table that illustrates the number of times that each intervention is reported as recommended, conditionally recommended, recommended against, or had inconclusive effectiveness. After similar interventions were grouped, nineteen remained. We subsequently used our grading system to identify the total score of each intervention group. The intervention groups and their total score are illustrated in Table 1.
| Intervention | Recommended (+1) | Conditionally recommended (+0.5) | Against (-1) | Inconclusive (-0.5) | Total score | Result |
|---|---|---|---|---|---|---|
| #NAME? | 12 | 0 | 0 | 0 | 12 | Recommended |
| Aerobic | 12 | 0 | 0 | 0 | 12 | Recommended |
| Education | 10 | 0 | 0 | 0 | 10 | Recommended |
| Mind-body | 6 | 3 | 0 | 0 | 7.5 | Conditionally recommended |
| Neuromuscular training | 7 | 1 | 0 | 0 | 7.5 | Conditionally recommended |
| Flexibility | 6 | 1 | 1 | 0 | 5.5 | Conditionally recommended |
| Aquatic exercise | 2 | 5 | 0 | 0 | 5.5 | Conditionally recommended |
| Psychological | 4 | 4 | 0 | 1 | 5.5 | Conditionally recommended |
| Walking aids | 4 | 3 | 0 | 0 | 5.5 | Conditionally recommended |
| Thermotherapy | 1 | 4 | 0 | 0 | 3 | Against |
| Gait training | 3 | 0 | 0 | 0 | 3 | Against |
| Physical Modalities | 4 | 4 | 3 | 1 | 2.5 | Against |
| Relaxing techniques | 2 | 3 | 1 | 0 | 2.5 | Against |
| Cryotherapy | 1 | 3 | 1 | 0 | 1.5 | Against |
| Manual therapy | 1 | 3 | 1 | 1 | 1 | Against |
| Brace | 2 | 1 | 1 | 2 | 0.5 | Against |
| Taping | 1 | 2 | 1 | 1 | 0.5 | Against |
| Acupuncture | 0 | 1 | 2 | 0 | -1.5 | Against |
| Insoles/ modified shoe | 1 | 0 | 2 | 1 | -1.5 | Against |
Table 6: Interventions table
Discussion
The study objectives were achieved. We systematically reviewed all eligible studies that aimed to identify KOA phenotypes and summarized all non-pharmacological interventions mentioned in the relevant literature. Only interventions were summarized, as variables were beyond the scope of this review. We opine that each rehabilitation programme should be tailored to each patient’s particularities or phenotype at the least. Further, we provide a unique algorithm based on critical reasoning to assist decision- making in conservative non-pharmacological treatment of KOA pain.
Phenotypes
According to our results, we believe that five KOA phenotype categories can be identified: neuropathic; local; physiological; high BMI; and comorbidities. We opine that these five phenotype categories summarize our results and include all the identified phenotypes reported. Of the five suggested phenotype categories, four (neuropathic, local, physiological, and high BMI) can be addressed through a rehabilitation/exercise programme, while the fifth (comorbidities) should be taken under consideration regarding the exercise variables.
Algorithm
While each phenotype might present individually, or in combination with one or more of the other four phenotypes, we suggest an evaluation algorithm to identify a patient’s specific phenotype. Each phenotype category shall be marked as positive or negative during the initial assessment. After all four categories were examined, one was left with a specific phenotype number (Table 2) that corresponds to the phenotype table where the therapist is advised which intervention to choose from the interventions table (Table 3). To the best of our knowledge, there is no other study that provides an evaluation algorithm of KOA phenotypes, and further suggestions for adequate approaches to each one.
| Phenotype | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Local pathology | Y | Y | Y | Y | Y | Y | Y | Y | N | N | N | N | N | N | N | N |
| Psychological | Y | Y | Y | Y | N | N | N | N | Y | Y | Y | Y | N | N | N | N |
| Neuropathic | Y | Y | N | N | Y | Y | N | N | Y | Y | N | N | Y | Y | N | N |
| High BMI | Y | N | Y | N | Y | N | Y | N | Y | N | Y | N | Y | N | Y | N |
Table 7: Phenotypes.
The initial phenotype can be extracted using Table 3. In this table, all possible answers following the algorithm are given. Sixteen phenotypes have been identified according to the four phenotype categories.
The therapist is instructed to choose interventions from the categories in which the patient phenotype is positive. Y, Yes; N, No; BMI, Body mass index.
| Local pathology interventions | Psychological interventions | Neuropathic interventions | High BMI interventions | |
|---|---|---|---|---|
| Mechanical tension | • Strengthening • Flexibility | • Education • Psychological interventions • Mind-body | • Mind-body • Neuromuscular training | • Weight loss |
| Metabolic stress | • Aerobic • Aquatic exercise | |||
| We categorized all the interventions that were marked as recommended or conditionally recommended according to the found phenotype categories and in correlation with the evaluation algorithm we suggest. |
Table 8: Categories of identified effective interventions.
Symptoms
After excluding the possibility of spine-related pain and relative red flags, one should follow the proposed algorithm. In the local category assessment, a clinician should aim to identify clinical findings that correspond to joint damage. It is extremely important to identify more than one symptom that corresponds to local pathology damage, because similar symptoms may be present in other knee pathologies also. Thus, the possibility of misdiagnosis is limited.
While one could argue that the neuropathic indicators category should be included in the psychology category, our results favour their separation. We accept that some psychological conditions, such as depression, might result in central sensitisation or widespread pain; however, an individual with alterations in the motor cortex due to chronic pain might not present with fear avoidance. Therefore, we support discrimination between brain-affected areas. Alterations to the mesolimbic and pre-frontal structures of the brain are labelled as psychological and motor or sensory cortex alterations, and any changes in the ascending and descending pain mechanisms are labeled as neuropathic.
While a gold standard for measuring pain sensitisation in humans does not exist, various methods are proposed in the literature [33]. In KOA, quantitative sensory testing (QST), temporal summation, conditioned pain modulation, and flexor withdrawal responses have been used [33, 34]. Methods involving pressure, temperature, cold thresholds, and pinpricks are predominantly used in QS [35] and pressure pain threshold measurement can be suitable for daily clinical practice because of its easy application and reliability [33, 34, 35, 36, 37]. Further, questionnaires such as pain DETECT and S-LANSS scales may assist a clinician to identify neuropathic pain [38, 39].
Interventions
According to our results, strengthening, aerobics, education, mind-body, neuromuscular training, flexibility, aquatic exercise, psychological interventions, and walking aids shall be considered potential interventions for KOA patients. The bio psychosocial concept of pain includes the biological, psychological, and social management of a patient with pain arising from any cause. While management of pain as a multifactorial symptom is highlighted in our results, we believe it might unnecessarily increase therapeutic intervention time. Thus, we suggest intervention choices only be made from the categories positively marked in the phenotypes table. While any type of exercise programme that is performed regularly and is closely monitored can improve KOA pain, we suggest the two mechanisms of muscle hypertrophy be considered [40]. It was proposed that mechanical tension results in better muscular adaptations than metabolic stress [40]. Therefore, despite both aerobic and strengthening being equally graded, we suggest strengthening in cases where weight bearing is not a limitation or provokes symptoms.
There is no evidence that favours a specific strengthening programme; however, we opine that general lower body training is the most suitable option because adding hip exercises can improve outcomes [41]. A frequency of two to three sessions per week is suggested [42, 43]. Exercise intensity should be the highest tolerance that does not cause discomfort to the patient. Identifying the initial intensity with a classic one repetition maximum (1RM) measurement might cause pain to the patient and consequently poor effort during measurement. Therefore, as per Tan et al. [44] we suggest the use of the predictive equation of 1RM. In cases where the ideal load cannot be achieved, we suggest muscular adaptations should be reached using a metabolic stress mechanism. In such a scenario, the aerobic exercise of an adequate dosage should be used [45]. We suggest aerobic exercise as the first-line treatment for the obese/overweight minor-phenotypes that require exercise, to better address obesity. For any patient who presents with laxity or balance impairments, we suggest hydrotherapy [46] because of the extra balance support provided by water pressure, and the reduced chance of falling while exercising, due to buoyancy. In phenotypes that do not require exercise, patients should be encouraged to engage in achievable amounts of physical activity of even modest intensity [47].
With respect to interventions under the psychological category, we suggest patient education and those psychological interventions used in studies where the intervention was applied by a physical therapist [48, 49, 50, 51, 52, 53]. While this category is beyond the scope of the physical therapist, the most suitable intervention according to clinical findings and therapist training should be considered.
For interventions under the neuropathic category, our results suggest the use of neuromuscular training and mind-body exercises. An approach that results in lasting neuropathic adaptations should be salient, include adequate repetitions, and sustain the attention of patients [6]. We suggest that therapists seek ways to combine neuropathic training with their general exercise programmes. For example, patients could perform exercises in front of a mirror, with the exercise divided into phases and speed of execution guided by a metronome. In a study of a healthy population, exercise with visual and acoustic cues was reported to result in greater strength measures compared to exercise without, suggesting a mechanism of neural adaptation that leads to greater muscle activation [54].
Concerning the twelfth phenotype, where only psychological indications are present, we suggest therapists encourage the patient to engage in a general exercise of any type and any intensity perceived as adequate, or group exercises such as yoga or Tai chi. Physical presence in a therapy center is not required, and the therapist can promote the patient’s compliance to instructions by weekly distance- delivered sessions. The patient shall also be referred to a psychologist if pain persists and the psychological indications do not improve in a reasonable period.
With respect to phenotype sixteen, where none of the three category indications matches, we suggest revaluating the local pathology indications with a reduced required percentage of acceptances. If the criteria subsequently match, other pathologies of the knee or early stages of KOA should be suspected. The patient should be advised to undergo an MRI of the joint. If the re-evaluation is again negative, the patient should be referred to a physician for a comorbidity check.
Sleep disturbance is common in KOA and is related to pain [55, 56]. We opine it can be addressed adequately without any modifications of the proposed phenotypes. When sleep disturbances are present and do not improve within a reasonable period, referral to a physician for sleep aid medication might be appropriate. We did not include sleep disturbance in any of the indication categories because of its multifactorial aetiology.
Comorbidities should always be considered. Each comorbidity affects the exercise variables whereby the treatment should not be dangerous, but should not be too light either. We suggest therapists adjust the exercise variables of their programme to the patient’s particularities without altering the suggested treatments given by the algorithm.
Other applications of the algorithm
Our algorithm can assist surgeons in identifying patients with a high risk of being non-responders to joint arthroplasty [9, 57]. We suggest that any phenotype without exclusively positive answers under local pathology indications (phenotype 8) is at high risk.
Limitations
This review presents some limitations. First, only articles written in English were considered, indicating that there is a risk of publication bias. Secondly, in conflict with other phenotype identification studies, we followed a different methodological procedure, with two searches. While methodology bias might be present, it allowed us to create a multidimensional text that discusses not only phenotypes but also the assessment and treatment of KOA. We opine that such multidimensional texts are needed for discussing such a complex subject.
Suggestions for Future Research
We suggest that the algorithm’s value could be validated using high-quality trials. Further research is needed to identify the most suitable interventions with respect to psychological deficiencies or neuropathic pain in the KOA population. We further suggest that the algorithm be retrospectively confirmed in surgical studies to evaluate the ability to identify non-responders to joint arthroplasty.
Implications for physiotherapy practice
Our algorithm can enhance daily clinical practice. We believe that it provides an easy way to identify each patient’s phenotype and choose the most appropriate intervention.
Conclusion
Based on the relevant literature, we systematically summarized KOA phenotypes. Through our results, five phenotype categories were identified. Further, we recommend the interventions with relevant guidelines, recommendations, or consensus. Finally, we suggest an algorithm that might be suitable for categorizing KOA patients. We suggest a specific evaluation procedure and tools to improve clinical outcomes and reduce the heterogeneity of literature results attributable to the inclusion of inappropriate phenotypes for applied interventions. The algorithm covers all the identified phenotypes according to our findings. Our algorithm might be a powerful tool in identifying non-responders to knee arthroplasty surgeries.
References
-
Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, et al. (2012) Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859): 2163-2196.
-
Fransen M, McConnell S, Harmer AR, Van Der Esch M, Simic M, et al. (2015) Exercise for osteoarthritis of the knee: A Cochrane systematic review. Br J Sports Med 49(24):1554-1557.
-
Ismail A, Moore C, Alshishani N, Yaseen K, Alshehri MA (2017) Cognitive behavioural therapy and pain coping skills training for osteoarthritis knee pain management : a systematic review. J Phys Ther Sci 2228-2235.
-
Finan PH, Buenaver LF, Bounds SC, Hussain S, Park RJ, et al.(2013) Discordance between pain and radiographic severity in knee osteoarthritis: Findings from quantitative sensory testing of central sensitization. Arthritis Rheum 65(2): 363-372.
-
Culvenor AG, Oiestad BE, Hart HF, Stefanik JJ, Guermazi A, et al (2019) Prevalence of knee osteoarthritis features on magnetic resonance imaging in asymptomatic uninjured adults : a systematic review and meta- analysis. Br J Sports Med 53(20): 1268-1278.
-
Pelletier R, Higgins J, Bourbonnais D (2015) Is neuroplasticity in the central nervous system the missing link to our understanding of chronic musculoskeletal disorders ? BMC Musculoskelet Disord 16: 25.
-
Mills K, Hubscher M, O Leary H, Moloney N (2019) Current concepts in joint pain in knee osteoarthritis. Der Schmerz 33(1): 22-29.
-
Caneiro JP, O Sullivan PB, Roos0 EM, Smith AJ, Choong P, et al. (2020) Three steps to changing the narrative about knee osteoarthritis care: A call to action. Br J Sports Med 54(5): 256-258.
-
Lundblad H, Kreicbergs A, Jansson KA (2008) Prediction of persistent pain after total knee replacement for osteoarthritis. J Bone Jt Surg Ser B 90(2): 166-171.
-
Dell Isola A, Allan R, Smith SL, Marreiros SSP, Steultjens M (2016) Identification of clinical phenotypes in knee osteoarthritis: a systematic review of the literature. BMC Musculoskelet Disord 17(1): 1-12.
-
Knoop J, Van Der Leeden M, Thorstensson CA, Roorda LD, Lems WF, et al. (2011) Identification of phenotypes with different clinical outcomes in knee osteoarthritis: Data from the osteoarthritis initiative. Arthritis Care Res 63(11): 1535-1542.
-
Kittelson AJ, Stevens Lapsley JE, Schmiege SJ (2016) Determination of Pain Phenotypes in Knee Osteoarthritis: A Latent Class Analysis Using Data from the Osteoarthritis Initiative. Arthritis Care Res 68(5): 612-620.
-
Kolasinski SL, Neogi T, Hochberg MC, Oatis C, Guyatt G, et al. (2020) 2019 American College of Rheumatology / Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand , Hip , and Knee. Arthritis Rheumatol 72(2):149-162.
-
Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, et al. (2019) OARSI guidelines for the non- surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr Cartil 27(11): 1578-1589.
-
Van Spil WE, Kubassova O, Boesen M, Bay Jensen AC, Mobasheri A (2019) Osteoarthritis phenotypes and novel therapeutic targets. Biochem Pharmacol 165: 41- 48.
-
Deveza LA, Melo L, Yamato TP, Mills K, Ravi V, et al. (2017) Knee osteoarthritis phenotypes and their relevance for outcomes: a systematic review. Osteoarthr Cartil 25(12): 1926-1941.
-
Nelson FRT (2018) The Value of Phenotypes in Knee Osteoarthritis Research. Open Orthop J 12(1): 105-114.
-
Aromataris E, Fernandez R, Godfrey CM, Holly C, Khalil H (2015) Summarizing systematic reviews : methodological development , conduct and reporting of an umbrella review approach 13(3): 132-140.
-
Whitinga P, Savovi J, Higginsa JPT, Caldwella DM, Reevese BC, et al. (2016) ROBIS : A new tool to assess risk of bias in systematic reviews was developed 69: 225-234.
-
Deveza LA, Melo L, Yamato TP, Mills K, Ravi V, et al. (2017) Knee osteoarthritis phenotypes and their relevance for outcomes : a systematic review. Osteoarthr Cartil 25(12): 1926-1941.
-
American Academy of Orthopaedic Surgeons (2013) Treatment Of Osteoarthritis Of The Knee Evidence- Based Guideline 2ndEdn.
-
Huang D, Liu Y, Liang L, Lin X, Song T, et al. (2018) The Diagnosis and Therapy of Degenerative Knee Joint Disease : Expert Consensus from the Chinese Pain Medicine Panel. 2018.
-
GokceKutsal, Tuncer T, Cay FH, Altan L, Gurer G, et al. (2018) 2017 update of the Turkish League Against Rheumatism (TLAR) evidence-based recommendations for the management of knee osteoarthritis. Rheumatol Int. 38(8): 1315-1331.
-
Royal Australian College of General Practitiones (2018) Guideline for the management of knee and hip osteoarthritis.
-
Osthoff AR, Niedermann K, Braun J, Adams J, Brodin N, et al. 2018 EULAR recommendations for physical activity in people with inflammatory arthritis and osteoarthritis. 77(9):1251-1260.
-
Brosseau L, Taki J, Desjardins B, Thevenot O, Fransen M, et al. (2017) The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis . Part one : Introduction, and mind-body exercise programs 31(5): 582-595.
-
Brosseau L, Taki J, Desjardins B, Thevenot O, Fransen M, et al. (2017) Westby M, Gallardo ICÁ, Gifford W. The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis . Part two : Strengthening exercise programs. 31(5): 596-611.
-
Brosseau L, Taki J, Desjardins B, Thevenot O, Fransen M, et al.(2017) The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis . Part three : Aerobic exercise programs. 31(5): 612-624.
-
Rillo O, Riera H, Acosta C, Liendo V, Bolaños J, et al. (2016) PANLAR Consensus Recommendations for the Management in Osteoarthritis of Hand, Hip, and Knee.22(7): 345-354.
-
(2014) osteoarthritis: the care and management of osteoarthritis in adults. National Institute for Health and Clinical Excellence. NICE Clin Guidel.
-
Peter H, Jansen J, Hurkmans J, Bloo H, Dekker J, et al. (2011) Physiotherapy in hip and knee osteoarthritis: Development of a practice guideline concerning initial assessment, treatment and evaluation. acta Reum port. 36(3): 268-281.
-
American Geriatrics Society (2001) Exercise Prescription for Older Adults With Osteoarthritis Pain : Consensus Practice Recommendations. 808-823.
-
Fingleton C, Smart K, Moloney N, Fullen BM, Doody C (2015) Pain sensitization in people with knee osteoarthritis: A systematic review and meta-analysis. Osteoarthr Cartil 23(7): 1043-1056.
-
Suokas AK, Walsh DA, McWilliams DF, Condon L, Moreton B, et al. (2012) Quantitative sensory testing in painful osteoarthritis: A systematic review and meta-analysis. Osteoarthr Cartil. 20(10): 1075–1085.
-
Arendt-Nielsen L (2017) Pain sensitisation in osteoarthritis. Clin Exp Rheumatol. 35(5): S68-74.
-
Kennedy DL, Kemp HI, Ridout D, Yarnitsky D, Rice ASC (2016) Reliability of conditioned pain modulation: A systematic review. Pain 157(11): 2410-2419.
-
De Oliveira Silva D, Rathleff MS, Petersen K, De Azevedo FM, Barton CJ (2019) Manifestations of pain sensitization across different painful knee disorders: A systematic review including meta-analysis and metaregression. Pain Med (United States) 20(2): 335-358.
-
Moss P, Benson HAE, Will R, Wright A (2018) Patients with Knee Osteoarthritis Who Score Highly on the PainDETECT Questionnaire Present with Multimodality Hyperalgesia, Increased Pain, and Impaired Physical Function. Clin J Pain 34(1): 15-21.
-
Bennett MI, Smith BH, Torrance N, Potter J (2006) The S-LANSS score for identifying pain of predominantly neuropathic origin: Validation for use in clinical and postal research. J Pain 6(3): 149-158.
-
Pearson SJ, Hussain SR (2014) A Review on the Mechanisms of Blood-Flow Restriction Resistance Training-Induced Muscle Hypertrophy. Sport Med 6(3): 149-158.
-
Hislop AC, Collins NJ, Tucker K, Deasy M, Semciw AI (2020) Hospital PC. Does adding hip exercises to quadriceps exercises result in superior outcomes in pain, function and quality of life for people with knee osteoarthritis ? A systematic review and meta-analysis. Br J Sports Med 54(5): 263-271.
-
Juhl C, Christensen R, Roos EM, Zhang W, Lund H (2014) Impact of exercise type and dose on pain and disability in knee osteoarthritis : A systematic review and meta- regression analysis of randomized controlled trials. Arthritis Rheum 66(3): 622-636.
-
Imoto AM, Pardo JP, Brosseau L, Taki J, Desjardins B, et al. (2019) Evidence synthesis of types and intensity of therapeutic land-based exercises to reduce pain in individuals with knee osteoarthritis. Rheumatol Int 39(7): 1159-1179.
-
Tan S, Wang J, Liu S (2015) Establishment of the Prediction Equations of 1RM Skeletal Muscle Strength in 60- to 75-Year-Old Chinese Men and Women. J Aging Phys Act 23(4): 640-646.
-
Schulz JM, Birmingham TB, Atkinson HF, Woehrle E, Khan MCM, et al. (2019) Are we missing the target ? Are we aiming too low ? What are the aerobic exercise prescriptions and their effects on markers of cardiovascular health and systemic inflammation in patients with knee osteoarthritis ? A systematic review and meta-analysis. Br J Sports Med 54(13): 771-775.
-
Dong R, Wu Y, Xu S, Zhang L, Ying J, et al. (2018) Is aquatic exercise more effective than land-based exercise for knee osteoarthritis? Med (United States) 97(52): e13823.
-
Kraus VB, Sprow K, Powell KE, Buchner D, Bloodgood B, et al. (2019) Effects of Physical Activity in Knee and Hip Osteoarthritis: A Systematic Umbrella Review. Med Sci Sports Exerc 51(6): 1324-1339.
-
Bennell KL, Ahamed Y, Jull G, Bryant C, Hunt MA, et al. (2016) Physical Therapist-Delivered Pain Coping Skills Training and Exercise for Knee Osteoarthritis: randomized Controlled Trial. Arthritis Care Res (Hoboken) 68(5): 590‐602.
-
Kao MJ, Wu MP, Tsai MW, Chang WW, Wu SF (2012) The effectiveness of a self-management program on quality of life for knee osteoarthritis (OA) patients. Arch Gerontol Geriatr 54(2): 317-324.
-
Hunt MA, Keefe FJ, Bryant C, Metcalf BR, Ahamed Y, et al. (2013) A physiotherapist-delivered, combined exercise and pain coping skills training intervention for individuals with knee osteoarthritis: a pilot study. Knee 20(2): 106‐112.
-
Hinman RS, Campbell PK, Lawford BJ, Briggs AM, Gale J, et al. (2020) Does telephone-delivered exercise advice and support by physiotherapists improve pain and/or function in people with knee osteoarthritis? Telecare randomised controlled trial. Br J Sports Med 54(13): 790-797.
-
Silva FS da, Melo FES de, Amaral MMG do, Caldas VVA, Pinheiro ILD, et al. (2015) Efficacy of simple integrated group rehabilitation program for patients with knee osteoarthritis: Single-blind randomized controlled trial. J Rehabil Res Dev 52(3): 309-322.
-
Bennell KL, Nelligan R, Dobson F, Rini C, Keefe F, et al. (2017) Effectiveness of an Internet-Delivered Exercise and Pain-Coping Skills Training Intervention for Persons With Chronic Knee Pain: A Randomized Trial. Ann Intern Med 166(7): 453-462.
-
Leung M, Rantalainen T, Teo WP, Kidgell D (2015) Motor cortex excitability is not differentially modulated following skill and strength training. Neuroscience 305: 99-108.
-
Dai Z, Neogi T, Brown C, Nevitt M, Lewis CE, et al. (2019) Sleep quality is related to worsening knee pain in those with widespread pain: The Multicenter Osteoarthritis Study. J Rheumatol 47(7): 1019-1025.
-
Koffel E, Kats AM, Kroenke K, Bair MJ, Gravely A, et al. (2019) Donaldson MT, Goldsmith ES, Noorbaloochi S, Krebs EE. Sleep Disturbance Predicts Less Improvement in Pain Outcomes: Secondary Analysis of the SPACE Randomized Clinical Trial. Pain Med 21(6): 1162-1167.
-
Pan F, Tian J, Munugoda IP, Graves S, Lorimer M, et al. (2020) Do Knee Pain Phenotypes Have Different Risks of Total Knee Replacement? J Clin Med 9(3): 632.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial