Effect of a Sensorimotor Training on Pain, Proprioception, and Functional Activities in Participants with Chronic Knee Osteoarthritis: A Randomized Controlled Clinical Trial
Background: Knee osteoarthritis (OA) is a chronic, debilitating condition that significantly impairs functional health status among affected individuals. Key challenges associated with chronic knee OA include persistent pain, diminished functional capabilities, and compromised balance. These factors highlight the critical need for effective intervention strategies. Recent research suggests that sensorimotor training may play a pivotal role in addressing these issues. However, there remains a gap in the literature regarding the specific effects of sensorimotor training on pain perception, proprioception, and overall functional levels in this population. Therefore, the aim of this study was to systematically investigate the impact of sensorimotor training on pain, proprioceptive abilities, and functional performance in individuals with chronic knee OA. Methods: Total 66 patients with chronic knee OA were divided into two equal groups. The control group received a traditional exercise programme and the experimental group received sensorimotor training in addition to traditional exercises. Blind assessment was conducted at the beginning of the study and after 4 weeks of training to measure pain by NPRS, proprioception acuity by passive – active joint position reproduction method, and functional disability by TUG & KOOS scale. Statistical analysis was performed using SPSS 23. Data were presented as mean, standard deviation (SD) and mean difference. Within groups compare we used Paired t test and between groups compare we used Independent t test with post data comparison in SPSS. The significance level was set at (p<0.05). Result: For experimental group and control group statistical significant (p<0.05) improvements were recorded in all measured parameters. Mean difference of KOOS in control group is 5.97% and experimental group is 17.63% and in mean difference of pain in control group is 2.33 and experimental group is 3.88 which shows that SMT is very effective than traditional exercise only. According to MCID of all outcomes, pain, KOSS and TUG test is clinically significant. The sensorimotor group produced significantly better improvement than the traditional group. Conclusion: Sensorimotor training along with traditional exercises is more effective then only traditional exercises for patients with chronic knee OA. The addition of sensorimotor training to traditional strengthening and stretching exercises could provide more motor control and help neuromuscular restoration of balance and subsequently improve the functional level of chronic knee OA subjects.
Abbreviations
JPS: Joint Position Sense; SMT: Sensori Motor Training; SD: Standard Deviation; OA: Osteoarthritis; NPRS: Numerating Pain Rating Scale.
Introduction
Osteoarthritis is one of the most prevalent musculoskeletal condition worldwide, which affects mainly the weight bearing joints like hip joint, knee joint & ankle joint [1]. Prevalence of knee OA is about 28.7% in India, which affects both elderly males and females [2, 3, 4]. It is a major reason of impairment and disability, which poses a significant burden in elderly dependent population in Asian countries [1].
Chronic knee OA also well-known as degenerative arthritis, degenerative joint disease or osteoarthritis. It is a group of mechanical abnormalities linking degradation of joints, subchondral bone and including articular cartilage [4]. Typical clinical symptoms includes knee pain and stiffness particularly after prolong activity and weight bearing, stiffness after inactivity, locking and sometimes effusion, all of which leads to decrease of functions of lower limb [2, 5, 6].
When chronic OA affects weight-bearing joints mainly the knee, it not only affects articular cartilage but moreover all joint structures which results in reduction of joint proprioception, muscle weakness and joint ROM [7]. Its leads to noticeable weakening of muscle function and especially impair the patient’s balance and functions such as the ability to perform sit-to-stand tasks, to gait alterations, functional limitation, and loss of independence [6]. Participants with chronic knee OA reported pain, stiffness, reduce ROM and difficulty with functional activities such as prolonged sitting, ascending and descending stairs, walking, squatting, kneeling, rising from a chair and using local transportation [7]. Therefore, Chronic knee OA is considered an inherent risk factor for the incidence of impaired balance and fall [6].
Joint Proprioception, of which joint position sense (JPS) is a component, contributes to static and dynamic knee joint stability by coordinating the actions of the quadriceps, hamstrings, and associated muscles around knee joint [8, 9]. Elderly with symptomatic chronic knee OA have been reported to have impaired balance, muscles strength, endurance, joint proprioception, balance and gait, as well as some mechanoreceptors in ligaments, and a higher rate of falls compared with those asymptomatic knee OA. As per literature, its show that joint proprioception reduced with injury, degeneration of joint and ageing. Decreased proprioception is associated with chronic knee OA, suggest that decreased joint proprioception may contribute to the onset or progression of chronic knee OA [8, 10, 11].
Sensori motor training (SMT) was developed by Dr. Janda as part of a treatment approach for chronic musculoskeletal pain syndromes. It emphasizes postural control and progressive functional tasks to the sensorimotor system to restore usual muscular system in participants with chronic musculoskeletal pain [12]. The proprio-sensory system supports the muscular system to maintain equilibrium on a reflex, automatic basis [13]. In response to an unexpected load, “the muscles will respond rapidly to stabilize the body, i.e., they will try to maintain balance and posture” [13].
This Programs mainly focused on restoration of sensorimotor function, therefore, would be of value in the treatment of chronic knee OA. It is based on the concept that instead of emphasizing the isolated strength of a group of muscles around a joint, we should understand the importance of the central nervous system in regulating functional movement in order to reach proper firing patterns for sustaining joint stability [6, 12].
The main objective of SMT is to restoring musculoskeletal control through improving sensory input from different parts of the body to improve balance and overall function level of the Participants [6]. Participants progress through three stages of SMT: static, dynamic, and functional. Within each stage, participants progress through exercises in different balance, postures, BOS and challenges to their center of gravity. Each exercise should provoke automatic and reflexive muscular stabilization, stimulating the participants to maintain postural control under a variety of circumstances [7, 12, 14].
As per theory, it could be estimated that sensorimotor training alter proprioception over traditional exercise training. SMT increases sensory input to the central nervous system thus improving sensorimotor function of the knee joint [15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27]. Kinesthaesia and balance training were reported to improve proprioception and functional performance of chronic knee OA participants [16, 17]. SMT is often overlooked throughout rehabilitation of chronic lower limb injury. It has been recommended that enhancing sensorimotor function can lead to improvement of functional performance in participants with knee injury as well as reducing its progression, especially in the older population [17, 27, 28].
Thus, the purposes of the current research were to examine the effects of sensorimotor training in addition to traditional exercises on pain, proprioception and functional activities in participants with chronic knee OA.
Materials and Methods
Total 289 participants of chronic knee OA in Charotar region, Gujarat were screened. Participants included in this study were diagnosed by an orthopedics as having grade I, II & III knee OA with the presence of knee pain, osteophytes and definite joint space narrowing based on the American College of Rheumatology criteria. Out of 289 participants, 66 participants met the inclusion criteria. The study was then performed on 66 participants.
The inclusion criteria were all the participants diagnosed by orthopedics with male and female with age between 45 to 65 years old, unilateral knee osteoarthritis, tibio-femoral and pattelo-fermoral osteoarthritis, kellegren-lawrance radiographically classification grade I, II & III with low to moderate risk of fall, willingness to participate in this study as a volunteer. Exclusion criteria included cardio respiratory disease (Ischemia, arrhythmia, chest pain and exercise induced bronchospasm), any knee surgery (Ligaments injury, TKR, meniscus injury), intra-articular steroid injection, RA, any neurological condition affecting lower limb or use any assistive device for walking Figures 1-6.






All the participants who were ready to participate for the research were informed about the process and written inform consent was taken from each participants prior to the research. Participants were randomized into two equal groups by lottery method. Allocating participants according to their arrival at the OPD alternatively to the Experimental group and the control group.
The pre-treatment baseline assessments were done on 1st day by the investigator other than primary investigator. Post treatment blinded assessments were then taken after 4th weeks. Assessment included Pain (0-10 NPRS), Proprioception acuity (Passive-active joint position reproduction method) and Functional scale KOOS- (Knee Injury and Osteoarthritis Outcome Scale) & Time Up and Go Test were also measured. Group allotter and Investigator both were blinded during study.
Measurement of Pain
Numerating Pain Rating Scale (NPRS) was used to measure the degree of perceived pain. The participants were asked to select a number between 0 and 10 on a 1 cm diagram with 0 representing no pain and 10 representing unbearable pain. The participants marked the number according to the pain intensity.
Measurement of Proprioception
Proprioception accuracy was measured using the passive – active joint position reproduction method, which has been described to be a valid method in the evaluation of proprioception. Goniometry was used to test the ability of the participants to actively repeat the passively position the knee angle. The target angle was 45-60 degrees and the test was repeated 3 times and the changes between the target angle position and the patient perceived end range position was calculated and calculated average of that.
Functional Level Measurements
The functional disabilities of the participants were measured by the KOOS scale. This scale has demonstrated reliability in participants with chronic knee OA. It measures level of disability on five subscales including Symptoms, Stiffness, Pain, Function, daily living, sport, recreational activities and quality of life. Participants were asked to rate their symptoms. The score is a percentage score from 0 to 100, with 0 indicate extreme problems and 100 indicate no problems. TUG test also used to measure the functional performance of sit to stand and walk.
Exercise Programme
Table 1 shows control group exercises protocol, they received only the traditional exercise Programme. Table 2 shows Experimental group exercises protocol, they received a sensorimotor training Programme in addition to a traditional Programme of strengthening and stretching exercises. The exercises were done for five sessions a week for four weeks in succession.
| Exercises | Repetitions | Sets | Weeks |
|---|---|---|---|
| ROM of knee joint (Knee Flexion & Extension) | 10 Rep | 3 Sets | 1st& 2nd weeks |
| Stretching exercises applied to hamstring and calf muscles | 30 Sec Hold | 3 Sets | |
| Quadriceps and hamstring isometric strengthening exercise. | 10 Sec Hold | 8-10 Rep | |
| Straight leg raising exercises (30-40 Degrees) | 10 Sec Hold | 8-10 Rep | 3rd weeks (in addition) |
| Short-arc terminal extension exercise for the knee joint | 10 Sec Hold | 8-10 Rep | |
| Isometric exercises for the abductor and adductor muscles of the hip | 10 Sec Hold | 8-10 Rep | |
| In 4th week all 3rd week exercises with the resistance. | 10 Rep | 3 Sets | 4th weeks (in addition) |
Table 1: Control Group: (Traditional exercise program).
*The maximum weight that could be lifted up to 10 times was determined; the exercises were then concluded as 10 repetitions with half of the weight, then three quarters of this weight, and finally the whole weight. Table 1: Control Group: (Traditional exercise program).
| Exercises | Repetitions | Sets | Weeks |
|---|---|---|---|
| First Phase (Static) | 3 times | 1st Week | |
| 1. Standing upright position (30 s) on a firm surface, then on a soft surface (a mat of 36 to 40--density softness use for the uneven surface). | 30-60 Sec | ||
| 2. Single leg standing with eyes closed (first the affected limb, then the non-affected limb) for10 s on a firm surface, the on a soft surface (a mat). | 10 Sec | ||
| 3. Half-step position for 10 s. | 10 Sec | ||
| 4. One-leg standing for 10 s. | 10 Sec | ||
| Second Phase (Dynamic), in addition: | 10 Rep | 3 Sets | 2nd Week (in addition) |
| 1. Forward stepping lunge. | |||
| 2. T-bank kicks exercise. | |||
| 3. Single leg balance | |||
| Third Phase (Functional), in addition: | 3 times | 3rd & 4th Week (in addition) | |
| 1. Walking exercise on a firm surface, then on a foam surface: | |||
| a) Toe skipping with toes straight ahead for 20 m, toes pointing outward for 20 m and toes pointing inward for 20 m. | |||
| b) Heel skipping with toes straight ahead for 20 m, toes pointing outward for 20 m and toes pointing inward for 20 m. | 3 times | ||
| 2. Squatting exercise: | |||
| a) Against a wall and away from a wall. | 10 Sec Hold | ||
| b) One leg squats on the affected and non-affected limb. | 3-5 times | ||
| 3. Balance exercise: | |||
| a) Walk front, back, side with eyes open and close.20m | |||
| b) Walk front, back and sides on slop.20m, 3 reps. | |||
| c) Stair up and down, front and sides.10 stairs, 3 reps. | |||
| d) Round walk with small circle on slow and fast speed. | 3 times | ||
| e) Round walk with large circle on slow and fast speed. | |||
| f) Long step walk front, back and side. 20 m, 3 reps. |
Table 2: Experimental group: (Sensorimotor training program).
Data Analysis
Statistical analysis was performed using “SPSS” version 23. Data were presented as mean and standard deviation (SD) and mean difference. For within group comparison we used Paired t-test and between group comparisons, we used Independent t-test with post data comparison in SPSS software. The significance level was set at (p < 0.05).
Result
Total 66 participants were enrolled in this study. There were 33 participants in Control Group and Experimental Group. There were no significant differences between the groups with respect to age, body weight, height and BMI (P > 0.05), as shown in Table 3.
| Variable | Group | Mean | SD | P |
|---|---|---|---|---|
| Age (years) | Control | 58.97 | ±3.75 | 0.1 |
| Experimental | 58.24 | ±3.97 | ||
| Weight (kg) | Control | 69.36 | ±11.20 | 0.088 |
| Experimental | 69.86 | ±11.34 | ||
| Height (cm) | Control | 162.58 | ±9.33 | 0.932 |
| Experimental | 162.72 | ±9.08 | ||
| BMI | Control | 26.5 | ±4.46 | 0.193 |
| Experimental | 26.61 | ±4.31 |
Table 3: Demographic Data.
There were no significant differences between the groups with respect to all baseline data (p>0.05), as shown in Table 4. As shown in Table 5, regarding changes in pain, proprioception and functional activities measures when comparing pre- and post-exercise scores, statistically significant improvements were obtained in all measures in the control group and experimental group. There were major statistically significant improvements in functional activities and proprioception on experimental group than control group. In both groups, statistically significant improvements were obtained in all measurement, at post-exercise compared with pre-exercise (P < 0.05). Experimental group shows a clinical significant in all outcome based on MCID. As shown in Table 6, between group post-treatment comparison regarding changes in pain, proprioception and functional activities measures when comparing post-exercise scores, statistically significant improvements were obtained in all measures between two groups (P < 0.05). Experimental group showed much higher improvement in all outcomes than control group.
| Outcomes | Groups (N=33) | Mean ±SD | Mean difference | Paired difference | P- value | |
|---|---|---|---|---|---|---|
| 95% CI | ||||||
| Lower | Upper | |||||
| NPRS | Control | 6.70±0.98 | 0.11 | 0.06 | 0.16 | 0.8 |
| Experimental | 6.81±0.62 | |||||
| #KOOS | Control | 50.70±6.23 | 1.97 | 1.23 | 2.71 | |
| Experimental | 25.67±4.51 | |||||
| $TUG TEST | Control | 12.65±1.24 | 0 | 0 | 0 | |
| Experimental | 12.62±1.12 | |||||
| ^JPS | Control | 14.30±1.93 | 0.54 | 0.43 | 0.65 | |
| Experimental | 14.84±1.80 |
Table 4: Between group pre-treatment comparison.
# = Percentage, $= Seconds, ^= Centimeter *significant difference (p<0.05) Table 4: Between group pre-treatment comparison.
| Outcomes | Groups (N=33) | PRE- mean ±SD | POST Mean ±SD | Mean difference ±SD | Paired difference 95% CI | P- value | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| NPRS | Control | 6.70±0.98 | 4.36±1.12 | 2.33±0.64 | 2.1 | 2.56 | 0.000* |
| Experimental | 6.52±0.62 | 2.64±0.90 | 3.88±0.74 | 3.62 | 4.14 | ||
| #KOOS | Control | 50.70±6.26 | 56.67±7.47 | -5.97±1.72 | -6.58 | -5.35 | |
| Experimental | 52.61±4.56 | 70.24±5.57 | -17.64±2.59 | -18.56 | -16.72 | ||
| $TUG | Control | 12.73±1.28 | 11.48±1.50 | 1.24±0.50 | 1.06 | 1.42 | |
| TEST | Experimental | 12.73±1.18 | 9.91±0.72 | 2.82±0.73 | 2.56 | 3.08 | |
| ^JPS | Control | 14.30±1.93 | 12.09±1.84 | 2.12±0.60 | 1.99 | 2.42 | |
| Experimental | 14.85±1.81 | 10.30±1.57 | 4.55±0.75 | 4.28 | 4.81 |
Table 5: Within group comparison.
# = Percentage, $= Seconds, ^= Centimeter *significant difference (p<0.05) Table 5: Within group comparison.
| Outcomes | Groups (N=33) | Mean ±SD | Mean difference | Paired difference | P- value | |
|---|---|---|---|---|---|---|
| 95% CI | ||||||
| Lower | Upper | |||||
| NPRS | Control | 4.36±1.11 | 1.72 | 2.23 | 1.22 | 0.000* |
| Experimental | 2.64±0.93 | |||||
| #KOOS | Control | 56.67±7.47 | 13.57 | 10.33 | 16.82 | |
| Experimental | 70.24±5.57 | |||||
| $TUG TEST | Control | 11.48±1.50 | 1.58 | 2.16 | 1.99 | |
| Experimental | 9.91±0.72 | |||||
| ^JPS | Control | 12.09±1.84 | 1.79 | 2.63 | 0.95 | |
| Experimental | 10.30±1.57 |
Table 6: Between group post-treatment comparison.
# = Percentage, $= Seconds, ^= Centimeter *significant difference (p<0.05) Table 6: Between group post-treatment comparison.
Discussion
In this study, we have investigated the effect of SMT on pain, joint proprioception and functional activities in subject with chronic knee osteoarthritis. SMT is a superior program aimed at restoring muscular control through increasing sensory input from different parts of the body to improve posture, balance and overall functional level of the participants [7, 10]. For this objective, we measured proprioceptive sense accuracy, pain level and functional level Graph 1 & Flow chart.
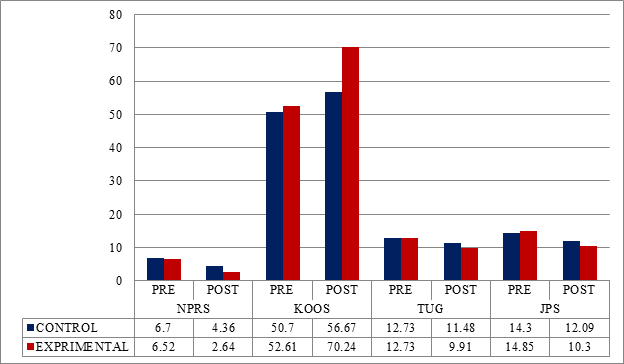
Graph 1: Group comparison.
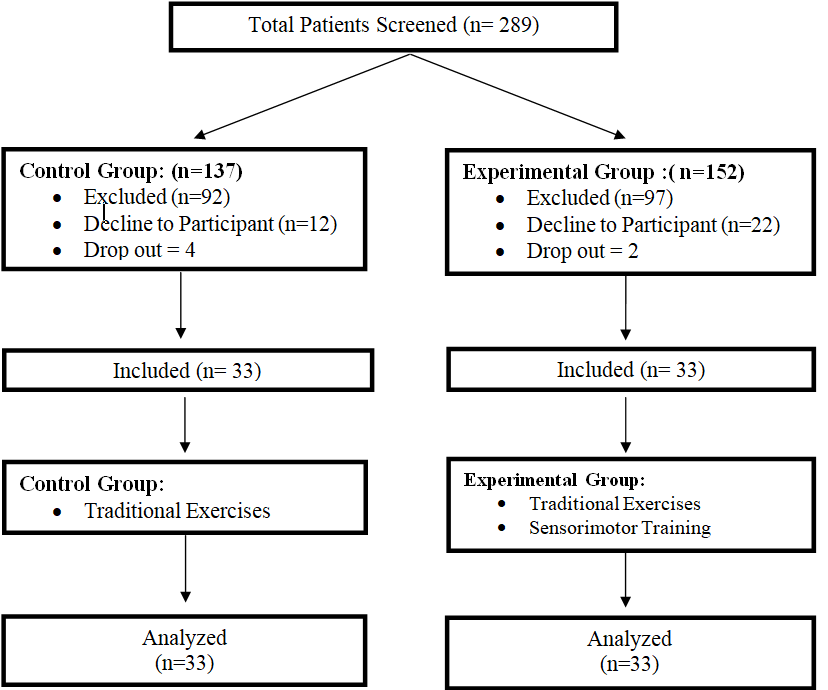
Flow chart: CONSORT flow chart.
The main findings of this study were that SMT produced significant improvement of all measurements, while a traditional exercise programme produced low significant improvement in all measures. It was recommended that the SMT increased coordination between muscle groups and improved the response to sensory-motor information. In SMT, the participants progresses through exercises in different postures, balance, BOS, and challenges to their center of gravity. Therefore, each exercise provokes automatic and reflexive muscular stabilization demanding the participants to maintain postural control under a variety of circumstances [15, 18, 27, 28] .
Several protocols are available for management of chronic knee OA with the aim of improving both patient complaints and overall functional activities. These protocols include traditional exercises programmes with a variety of ROM exercises, strength training and flexibility exercises [19, 20]. Nevertheless, patient complaints often persist and function activities levels cannot be returned [6].
Proprioception is one of the key parameters for maintaining good posture, balance, joint position sense and fall. It was shown that disruption of the afferent component of protective neuromuscular reflexes may lead to increased, repetitive, poorly distributed load across the articular surface, resulting in OA [21, 22]. Alternatively, knee joint position sense impairment might result from the osteoarthritis pathologic process, destroying or disturbing the function of capsule, ligament and/or muscle and tendon mechanoreceptors [21, 22]. The possibility that proprioceptive impairment is a pathogenetic factor in knee OA is a clinically important issue, because if this hypothesis is true, treatment of proprioceptive impairment will have a disease-modifying effect. It seems that further studies are required to detect the importance of impaired proprioception in the progression of knee OA [23].
On average, a reduction of one point or a reduction of 15.0% in the NRS represented a MCID for the patient [29, 30]. A change of 8-10 points may represent a minimal perceptible clinical improvement for the KOOS scale [31]. The average TUG Test MCID was 3.4 s using all 3 methods and all anchors [32].
The association between OA and loss of proprioception, muscle weakness and pain has been reported [8, 11, 24, 29]. These declines in sensory output from the knee joint affects sensorimotor function and may result in impairment functional activities [12, 14, 23]. Even Association between age, severity, grades of OA, pain and proprioception has been reported. In our study, we found significant result for improving proprioception activity by given sensorimotor training. This study shows positive statistically significant changes were detected in the sensorimotor group compared with the traditional exercises group. There are many studies that have investigated the effect of standard traditional exercises in the management of knee OA and reported decreased pain and increased muscle power with consequent improvement in proprioception and functional level. However, according to the results of the current study, it is thought that this type of exercise programme is not enough and cannot achieve optimal functional capacity levels. Exercises should increase neuromuscular control and meet the needs of daily activities.
Shrikant Bhimrao Darade, et al. [23] was concluded that, Effect of sensory motor training program shown improvement in balance, reduction in fear of fall, improves quality of life and also helps to prevent fall in community dwelling elderly individuals with history of fall. This sensory motor training program has shown long lasting effect, up to 6 months of follow up in community dwelling elderly individuals [23, 26].
In our study sensorimotor training program shown improvement in pain, proprioception and functional activities, although both groups produced statistically significant improvements at post-exercise compared with pre-exercise, statistically significant and clinically positive changes were detected in the sensorimotor group compared with the traditional exercises group [26]. There were many studies that have examined the effect of standard traditional exercises in the management of knee OA and reported decreased pain and increased muscle power with consequent improvement in proprioception and functional level [12, 25]. It was concluded that close-chain kinematics is more effective in improving proprioception functional performances in individuals with knee osteoarthritis [10]. Many studies show that improvement in the balance and co-ordination of muscles was better for proprioception improvement.
Conclusion
Over all sensorimotor training was better in improving functional activities and proprioception then traditional exercises in participants with Chronic knee OA. Only traditional exercise likes strengthening exercise, range of motion exercise and stretching will give improvement in knee OA but mainly balance and functional activities are often neglected and are not included in treatment protocol. So traditional exercises along with sensorimotor training which gives better improvement in participants with chronic knee OA and should be included in management protocol.
• Limitations Limitation of this study is small sample size and Language problem in scale measurement. Difficult to understand exercise program for participants.
- Ethical Approval & Clinical Trail Registration This study was approved by Ethical Committee of the Ashok & Rita Patel Institute of Physiotherapy, CHARUSAT, Changa. (AIRP/IRB/14/25) This study was approved by Clinical Trial Registry – India. REF/2015/009850 CTRI Number: CTRI/2017/04/008409, CTRI website URL-http:// ctri.nic.in
- Acknowledgements The author is grateful to the Santram Physiotherapy center Nadiad, for their help with assessment.
References
-
Shaheen AM, Ayad K (2008) Impact of Chronic Osteoarthritis of Knee Joint on Postural Stability and Functional Mobility in Women. Bull Fac Ph Th Cairo Univ 13(1): 317-331.
-
Shadab M, Zulkifle M, Ansari AH, Itrat M (2014) Prevalence of knee osteoarthritis in participants visiting NIUM hospital Bangalore. International Journal of Herbal Medicine 2(2): 61-64.
-
Ajit NE, Nandish B, Fernandes RJ, Roga G, Kasthuri A, et al. (2014) Prevalence of knee osteoarthritis in rural areas of Bangalore urban district. Internet Journal of Rheumatology and Clinical Immunology 1(S1): SO3.
-
Pal CP, Singh P, Chaturvedi S, Pruthi KK, Vij A (2016) Epidemiology of knee osteoarthritis in India and related factors. Indian J Orthop 50(5): 518-522.
-
Felson DT (2009) Developments in the clinical understanding of osteoarthritis. Arthritis Research & Therapy 11(1): 203.
-
Ahmed AF (2011) Effect of sensorimotor training on balance in elderly participants with knee osteoarthritis. Journal of Advanced Research 2: 305-311.
-
Cammarata ML, Schnitzer TJ, Dhaher YY (2011) Does Knee Osteoarthritis Differentially Modulate Proprioceptive Acuity in the Frontal and Sagittal Planes of the Knee?. Arthritis Rheum 63(9): 2681-2689.
-
Hassan BS, Mockett S, Doherty M (2001) Static postural sway, proprioception, and maximal voluntary quadriceps contraction in participants with knee osteoarthritis and normal control participants. Ann Rheum Dis 60(6): 612- 618.
-
Wegener L, Kisner C, Nichols D (1997) Static and Dynamic Balance Responses in Persons with Bilateral Knee Osteoarthritis. J Orthop Sports Phys Ther 25(1): 13-18.
-
Gbiri CA, Okafor UAC, Alade MT (2013) Comparative Efficacy of Open-chain and Close-chain Kinematics on Proprioception, Muscles’ Strength and Functional Performances in Individual with Knee Osteoarthritis. Occup Med Health Aff 1: 104.
-
Knoop J, Steultjens MPM, Leeden M, Esch M, Thorstensson CA (2011) Proprioception in knee osteoarthritis: Narrative review. Osteoarthritis and Cartilage 19(4): 381-388.
-
Page P (2006) Sensorimotor training: A ‘‘global’’ approach for balance training. Journal of Bodywork and Movement Therapies 10(1): 77-84.
-
Elshazly FAA, Nambi GS, Elnegamy TE (2016) Comparative study on Virtual Reality Training (VRT) over Sensory Motor Training (SMT) in Unilateral Chronic Osteoarthritis-A Randomized Control Trial. Int J Med Res Health Sci 8: 7-16.
-
Hurley MV, Scott DL, Rees J (1997) Sensorimotor changes and functional performance in participants with knee osteoarthritis. Ann Rheum Dis 56(11): 641-648.
-
Kapreli E, Athanasopoulos S, Papathanasiou M, Van Hecke P, Kelekis D, et al. (2007) Lower limb sensorimotor network: issues of somatotopy and overlap. Cortex 43(2): 219-232.
-
Diracoglu D, Aydin R, Baskent A, Celik A (2005) Effects of kinesthesia and balance exercises in knee osteoarthritis. J Clin Rheumatol 11(6): 303-310.
-
Tsauo JY, Cheng PF, Yang RS (2008) The effects of sensorimotor training on knee proprioception and function for participants with knee osteoarthritis: a preliminary report. Clin Rehabil 22(5): 448-457.
-
Solomonow M, Krogsgaard M (2001) Sensorimotor control of knee stability: A review. Scand J Med Sci Sports 11(2): 64-80.
-
Huang MH, Lin YS, Yang RC, Lee CL (2003) A comparison of various therapeutic exercises on the functional status of participants with knee osteoarthritis. Semin Arthritis Rheum 32(6): 398-406.
-
Eyigor S, Hepguler S, Capaci K (2004) A comparison of muscle training methods in participants with knee osteoarthritis. Clin Rheumatol 23(2): 109-115.
-
Burton E, Cavalheri V, Adams R, Browne CO, Spencer PB, et al. (2015) Effectiveness of exercise programs to reduce falls in older people with dementia living in the community: A systematic review and meta-analysis. Clin Interven Aging 10: 421-434.
-
Petridou ET, Manti EG, Ntinapogias AG, Negri E, Szczerbinska K (2009) What works better for community-dwelling older people at risk to fall? a meta- analysis of multifactorial versus physical exercise-alone interventions. J Aging Health 21: 713-729.
-
Darade SB, Ganvir SD (2017) Effectiveness of Sensory Motor Training Program in Community Dwelling Elderly Individuals with History of Fall. Physiother Rehabil 2: 2.
-
Koralewicz LM, Engh GA (2000) Comparison of proprioception in arthritic and age-matched normal knees. J Bone Joint Surg Am 82(11): 1582-1588.
-
Taghizadeh S (2008) Proprioception, dynamic balance and maximal quadriceps strength in females with knee osteoarthritis and normal control participants. Int J Rheum Dis 11(1): 39-44.
-
Segal NA, Glass NA (2010) The Effect of Quadriceps Strength and Proprioception on Risk for Knee Osteoarthritis. Med Sci Sports Exerc 42(11): 2081-2088.
-
Riemann BL, Lephart SM (2002) The Sensorimotor System, Part I: The Physiologic Basis of Functional Joint Stability. J Athl Train 37(1): 71-79.
-
Riemann BL, Lephart SM (2002) The Sensorimotor System, Part II: The Role of Proprioception in Motor Control and Functional Joint Stability. J Athl Train 37(1): 80-84.
-
Shakoor N, Furmanov S, Nelson DE (2008) Pain and its relationship with muscle strength and proprioception in knee OA: Results of an 8-week home exercise pilot study. J Musculoskelet Neuronal Interact 8(1): 35-42.
-
Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W (2004) Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur J Pain 8(4): 283-291.
-
Salavati M, Akhbari B, Mohammadi F, Mazaheri M, Khorrami M (2011) Knee injury and Osteoarthritis Outcome Score (KOOS); reliability and validity in competitive athletes after anterior cruciate ligament reconstruction. Osteoarthritis Cartilage 19(4): 406-410.
-
Gautschi OP, Stienen MN, Corniola MV, Joswig H, Schaller K (2017) Assessment of the Minimum Clinically Important Difference in the Timed Up and Go Test after Surgery for Lumbar Degenerative Disc Disease. Neurosurgery 80(3): 380-385.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial