Effect of Yoga on Gait, Balance, Trunk Control and Lower Limb Functions after Stroke: An Experimental Study
Introduction: Stroke is a leading cause of long-term disability, with lower limb dysfunction being the most common symptom. Impairments in balance, trunk control, and gait significantly impact mobility and quality of life. While conventional rehabilitation methods target these deficits, therapies like yoga may provide added benefits. This study aims to evaluate the effect of integrating yoga with conventional therapy on gait, balance, trunk control, and lower limb function in stroke patients. Methods: 32 subjects were randomly assigned to two groups. Group 1 received conventional therapy, while Group 2 underwent conventional therapy with yoga, 4-5 days per week for 4 weeks. Outcome measures included Brunnstrom Recovery Stage of Lower Extremity (BRS-LE), Fugl-Meyer Assessment Lower Extremity (FMA-LE), Barthel Index (BI), Berg Balance Scale (BBS), Dynamic Gait Index (DGI), and Trunk Impairment Scale (TIS). Intra-group comparisons were analyzed using the Wilcoxon Signed Ranks Test, and inter-group differences were assessed using Mann-Whitney U test. Results: Both groups showed significant improvements in gait, balance, trunk control, and lower limb function. However, the experimental group demonstrated significantly greater improvements in BRS-LE, FMA-LE, BBS, and DGI scores compared to control group. Conclusion: Adding yoga to conventional therapy significantly enhances recovery of gait, balance, trunk control, and lower limb function in stroke patients
Rathod H¹*, Pathan S¹, Matolia R¹ and Lad M²
¹Shrimad Rajchandra College of Physiotherapy, Uka Tarsadia University, India ²SSCP, India
Abbreviations
WHO: World Health Organization; TIS: Trunk Impairment Scale; DGI: Dynamic Gait Index; BBS: Berg Balance Scale; BI: Barthel Index; FMALE: Fugl-Meyer Assessment Lower Extremity Scale; BRSLE: Brunnstrom Recovery Stages of Lower Extremity.
Introduction
Stroke remains a major global health concern, ranking as one of the leading causes of disability and death worldwide. According to the World Health Organization (WHO), nearly 15 million people suffer from strokes each year, of which 5 million are left permanently disabled [1]. A stroke typically results from the disruption of blood flow to the brain, causing neuronal damage and impairments in various functional domains, particularly motor control. Survivors of stroke frequently experience deficits in gait, balance, trunk control, and lower limb function, significantly affecting their independence and quality of life [2].
Motor dysfunctions post-stroke often manifest in difficulty walking, maintaining postural stability, and coordinating movement, particularly of the lower limbs. Impaired gait and balance increase the risk of falls, which are a common and severe consequence in stroke survivors. These individuals often develop compensatory movement patterns, which can further exacerbate mobility issues and hinder full recovery [3]. In this context, rehabilitation strategies aimed at improving motor function, particularly those targeting gait and balance, are vital for promoting independence and reducing secondary complications such as falls and muscle atrophy.
Traditional rehabilitation approaches for stroke, including physical and occupational therapy, have shown efficacy in improving motor functions. These therapies often focus on strength training, mobility exercises, and balance tasks [4]. However, in recent years, there has been a growing interest in exploring alternative and complementary interventions, such as yoga, that may offer additional benefits in motor recovery post-stroke.
Yoga is an ancient practice that originated in India and combines physical postures (asanas), breath control (pranayama), and meditation techniques to promote physical, mental, and emotional well-being [5]. In the context of neurological rehabilitation, yoga is gaining attention for its potential to improve flexibility, balance, coordination, and overall physical functioning [6]. Yoga’s focus on mindful movement, breathing, and postural control makes it particularly suitable for stroke survivors, who often struggle with proprioception, coordination, and maintaining postural stability.
Several studies have investigated the therapeutic effects of yoga on motor functions in various populations. For instance, a study by Schmid A, et al. [7] reported that yoga improved balance and mobility in chronic stroke survivors, while other research has highlighted yoga’s role in reducing muscle spasticity and improving trunk control in individuals with neurological conditions [8]. The holistic nature of yoga, which integrates both mental and physical aspects of recovery, may also offer psychological benefits, such as reducing anxiety, depression, and improving mood, which are common in stroke survivors [9].
Despite the growing body of evidence supporting yoga’s potential benefits in stroke rehabilitation, there remains a gap in understanding its specific impact on gait, balance, trunk control, and lower limb function. Given the multifaceted nature of stroke recovery, it is essential to evaluate whether yoga can complement traditional rehabilitation strategies to enhance these critical domains of motor function. This experimental study aims to examine the effect of yoga on gait, balance, trunk control, and lower limb functions in individuals recovering from stroke. The study will utilize a structured yoga intervention tailored to the needs of stroke survivors and assess its efficacy compared to traditional rehabilitation approaches. By focusing on these key functional domains, this research seeks to provide a comprehensive understanding of yoga’s role in enhancing motor recovery after stroke.
Materials and Methods
Study Design
An experimental study was conducted across multiple healthcare facilities, including the Physiotherapy departments of Sardar Smarak Hospital, Shrimad Rajchandra College of Physiotherapy, and Shishudeep Multispecialty Hospital in Bardoli, as well as the Ayurvedic Hospital in Surat. A convenient sampling method was employed to recruit participants. The sample size was determined using the G Power 3.1.9.2 software, with an effect size of 0.9, an alpha level of 0.05, and a statistical power of 0.65. Based on these parameters, the required sample size was calculated to be 30 participants. The study took place over a period of one year, from March 2023 to March 2024.
Participants
Participants were eligible for inclusion if they had been diagnosed with stroke, confirmed by a CT scan, MRI, or other medical reports by a neurophysician, and were between the ages of 30 and 70. Additionally, participants were required to have had a stroke between 3 weeks and 6 months prior to the study, have a score of 24 or higher on the Mini-Mental State Examination (MMSE), and demonstrate the ability to follow instructions. Furthermore, patients needed to be in Brunnstrom recovery stage 3 or higher to be included in the study. Exclusion criteria included individuals who were unable to comprehend simple commands, patients with chronic stroke, and those with other neurological disorders. Participants with musculoskeletal conditions such as fractures or dislocations in the hip or deformities in the lower limb were also excluded, as were individuals with visual or auditory impairments or severe sensory and perceptual deficits that could impact study outcomes.
Procedure
After receiving clearance from the Institutional Ethics Committee, the present study was initiated with the aim of examining the effect of yoga on gait, balance, trunk control, and lower limb functions in post-stroke patients. Although dropouts were anticipated, none of the participants withdrew from the study. A total of 32 subjects, all of whom had experienced a stroke lasting from 3 weeks to 6 months, were recruited based on the study’s inclusion criteria. These subjects, both male and female, aged between 30 and 70 years, voluntarily agreed to participate. After a thorough screening process, each subject was provided with detailed information about the study, and a written consent form was signed to confirm their willingness to participate.
The participants were divided into two groups: Group 1 (Control group) and Group 2 (Experimental group). Group 1 received conventional physiotherapy, while Group 2 received both yoga and conventional physiotherapy. The subjects in both groups participated in training sessions that lasted approximately 45-50 minutes per day, 4 to 5 days a week, over a period of 4 weeks, for a total of 16-20 sessions.
Exercise Protocol
Group 1: Conventional Physiotherapy The conventional physiotherapy protocol involved stretching exercises for tight muscles in both the upper and lower extremities, along with strengthening exercises for the same muscle groups.
Supine Lying Position
Stretching exercises were performed for the tight muscles of the upper and lower limbs, with each stretch held for 30 seconds and repeated 3 times.
Active or active-assisted movements were administered to immobile joints, including shoulder, elbow, wrist flexion and extension, forearm supination and pronation, and finger movements, all repeated 10 times.
Lower limb exercises included hip flexion, extension, abduction, internal and external rotation, knee flexion and extension, ankle dorsiflexion and plantar flexion, and inversion and eversion, all performed 10 times (Figure 1).

Bridging and Trunk Rotation exercises were also incorporated, each repeated 10 times.
Sitting Position
Subjects performed knee flexion and extension exercises on a plinth, repeated 10 times.
Upper limb weight-bearing exercises in the sitting position were also included.
Standing Position
Subjects practiced standing with and without support, reaching out to both sides, repeated 5 times. Group 2: Yoga and Conventional Physiotherapy In addition to the conventional physiotherapy protocol outlined for Group 1, participants in Group 2 practiced specific yoga postures designed to improve balance, strength, and flexibility.
Yoga Postures
Malasana: Subjects performed this posture by squatting with feet slightly wider than hip-width apart, hands in the ‘Namaskar’ position, and a straight spine. This posture was held for 30 seconds and repeated 3 times (Figure 2).

Bhujangasana: Subjects lay on their stomachs, placing their palms on the ground under their shoulders. They lifted their head, chest, and abdomen while keeping the navel on the floor, holding the position for 4-5 breaths and repeating 3 times (Figure 3).

Adho Mukha Svanasana: After performing Bhujangasana, subjects transitioned into this pose by lifting their hips and keeping their feet parallel. They held the posture for 5-10 breaths and repeated 3 times (Figure 4).

Ashwa Sanchalanasana: In this posture, subjects stepped one foot forward between the hands, lifting their trunk while stretching the opposite leg back. This was held for 5-10 seconds and repeated 3 times on each side (Figure 5).

The conventional physiotherapy treatment for Group 2 was the same as that administered to Group 1.
Outcome Measures
Upon obtaining consent, patients completed a demographics questionnaire, ensuring that no personally identifiable information was captured or shared with the research team, aside from the treating physical therapist. Assessments were conducted both prior to and immediately following the intervention. Brunnstrom Recovery Stages of Lower Extremity (BRSLE): The BRS was designed to describe a sequence of extremity motor recovery after stroke based on the synergy pattern on movement that develops during recovery from a flaccid limb to near-normal and normal movement and coordination. The BRS contains 3 items: for the arm (BRS-A), the hand (BRS-H) and the leg (BRS-L), which are scored on a 6-level Likert-type scale (level I to VI). Higher level represents better motor function. It takes less than 10 minutes to complete the evaluation. The Rasch reliabilities of the upper extremity motor function and overall motor function were high 0.91-0.92. Therefore, the BRS may be useful in both clinical and research settings [10]. Fugl-Meyer Assessment Lower Extremity Scale (FMALE): The FMA-LE assess lower extremity motor function including reflex activity, movement within and outside synergy patterns. It comprises 17 items in two subscales: Lower extremity (E) and speed/coordination (F), which scored on a 3-level ordinal scale (0 points: none; 1 point: partial; 2 points: full). The maximum score for the lower extremity subscale is 28 points and for speed/coordination 6 points. In this study for only assessing lower limb motor function so used lower extremity subscale component from the Fugl- Meyer Assessment scale. There are mainly 5 items which are
further divided into total 14 components and the items are scored and then summed up maximum score for the lower extremity subscale is 28 points. This scale has high reliability ICC was high as 0.95- 0.99 [11]. Barthel Index (BI): Barthel index is an ordinal scale which is routinely used standard tool for assessing functional independence. The index analyzes 10 self-care aspects: bowels, bladder, grooming, toilet use, feeding, transfer, mobility, dressing, stairs and bathing. The total score ranges from 0 to 100 points. The higher score, the greater functional independence. It has a good to excellent reliability for all scores and subscales ICC 0.82-0.99 and good sensitivity to changes in ADL [12, 13]. Berg Balance Scale (BBS): Berg balance scale is high reliable tool with absolute reliability ICC is 0.97. It is used to measure assessed static as well as dynamic balance among older people with impairment in balance function by assessing the performance of functional tasks. Furthermore, this tool includes 14 items with 5-point scale, a range of 0 to 4 with the score of 0 means in lowest level of function and 4 means highest level of function. A global score or total possible score is 56. Score between 0 to 20 high fall risk, 21 to 40 represent medium fall risk and 41 to 56 low fall risk [14]. Dynamic Gait Index (DGI): Dynamic gait index is used to evaluate functional stability during gait activities in older people and to evaluate their risk of falling. The DGI tests 8 facets of gait and can be used with an assistive device such as walking with normal speed, walking while changing speed, turning the head horizontal, turning the head vertical, gait with pivot turn, walking over and around obstacles and stair climbing. Scores are based on 4-point scale: 0 represent severe impairment, 1 represent moderate impairment, 2 represent minimal impairment and 3 represent no gait dysfunction. It has good interrater reliability ICC 0.96 and validity r=0.83 [15].
Trunk Impairment Scale (TIS): The TIS measures the motor impairment of the trunk after a stroke through the evaluation of static and dynamic sitting balance as well as coordination of trunk movement. The TIS consists of the three subscales: sitting balance, dynamic balance and coordination. Each subscale contains between three and ten items. The TIS score ranges from a minimum of 0 to a maximum 23. In this study to assess trunk control by using two subscales of the TIS are static balance and dynamic balance. So, for assessing static balance total score is summed up from maximum score 7 and for dynamic balance total score is summed up from maximum score 10. It has a good test-retest reliability and interobserver reliability for the TIS total score ICC was 0.96 and 0.99, respectively and concurrent validity r= 0.83 [16, 17].
Statistical Analysis
Descriptive statistics including mean, standard deviation were analyzed. Mann-Whitney U test was used for comparing means between all the two groups. Wilcoxon Singed Ranks Test was used to compare the difference within the groups at two time periods- baseline and after 4 weeks. Results were considered to be significant at p<0.05 and confidence interval was set at 95%. All statistical analysis was performed using SPSS version 21.0.0.
Results
Thirty-two patients participated in this study, with a mean age of 52.25 years (standard deviation [SD] = 12.71) for group 1 and 53.06 years (standard deviation [SD] = 9.63) for group 2.
Table 1 shows the descriptive statistics of age, duration of stroke and Mini Mental State Examination (MMSE) among 16 subjects per group for all 32 subjects in both the groups.
| Group 1 (mean ± SD) | Group 2 (mean ± SD) | |
|---|---|---|
| Age | 52.25 ± 12.71 | 53.06 ± 9.63 |
| Duration of Stroke | 120 ± 69.02 | 99.19 ± 61.17 |
| Mini Mental State Examination | 28.13 ± 1.67 | 28.75 ± 1.53 |
Table 2: Demographic Characteristics of Participants.
Table 2 shows the descriptive statistics of gender, occupation, dominance side and affected side distribution among 16 subjects per group for all 32 subjects in both the groups.
| Characteristics | Group 1(Frequency) | Group 2(Frequency) | |
|---|---|---|---|
| Gender | |||
| Male (n) | 62.5% (10) | 50% (8) | |
| Female (n) | 37.5% (6) | 50% (8) | |
| Occupation | |||
| Worker (n) | 56.25% (9) | 37.5% (6) | |
| Housewife (n) | 37.5% (6) | 50% (8) | |
| Retired (n) | 6.25% (1) | 12.5% (2) | |
| Dominance side | |||
| Right (n) | 93.75% (15) | 81.25% (13) | |
| Left (n) | 6.25% (1) | 18.75% (3) | |
| Affected side | |||
| Right (n) | 43.75% (7) | 68.75% (11) | |
| Left (n) | 56.25% (9) | 31.25% (5) | |
Table 1: Demographic Characteristics of Participants in Frequency.
Table 3 shows result of within group analysis for Group-I using Wilcoxon Singed Ranks test to determine the difference between pre and post treatment.
The pre- and post-treatment outcomes for various clinical measures were analyzed, and significant improvements were observed across all parameters. The mean Brunnstrom Recovery Stage (BRS) score increased from 4.38 ± 0.89 pre- treatment to 5.00 ± 0.82 post-treatment, with a p-value of 0.002, indicating statistical significance. Similarly, the mean Fugl-Meyer Assessment for Lower Extremity (FMA-LE) score improved from 22.56 ± 3.86 to 24.44 ± 2.58, with a p-value of 0.003, also considered significant.
For the Barthel Index (BI), the mean score rose from 70.63 ± 23.66 pre-treatment to 77.50 ± 19.83 post-treatment, yielding a p-value of 0.001, indicating a statistically significant improvement. The Berg Balance Scale (BBS) score increased from a mean of 37.94 ± 14.73 to 41.19 ± 13.03, with a p-value of 0.001, signifying a significant enhancement in balance. Additionally, the Dynamic Gait Index (DGI) score showed a mean increase from 12.13 ± 8.10 to 14.38 ± 7.22, with a p-value of 0.001, highlighting a significant improvement in gait. Lastly, the Trunk Impairment Scale (TIS) score improved from 14.25 ± 2.35 pre-treatment to 15.25 ± 1.57 post-treatment, with a p-value of 0.004, confirming statistical significance.
| Outcome measures | Mean | SD | Mean difference | Z value | P value (<0.05 sig) |
|---|---|---|---|---|---|
| BRS Pre | 4.38 | 0.89 | 0.62 | -3.162 | 0.002 |
| BRS Post | 5 | 0.82 | |||
| FMA LE Pre | 22.56 | 3.86 | 1.88 | -2.953 | 0.003 |
| FMA LE Post | 24.44 | 2.58 | |||
| BI Pre | 70.63 | 23.66 | 6.87 | -3.256 | 0.001 |
| BI Post | 77.5 | 19.83 | |||
| BBS Pre | 37.94 | 14.73 | 3.25 | -3.305 | 0.001 |
| BBS Post | 41.19 | 13.03 | |||
| DGI Pre | 12.13 | 8.1 | 2.25 | -3.322 | 0.001 |
| DGI Post | 14.38 | 7.22 | |||
| TIS Pre | 14.25 | 2.35 | 1 | -2.913 | 0.004 |
| TIS Post | 15.25 | 1.57 |
Table 3: Within Group Comparison for Group 1.
Graph 1 shows the pre- post comparison for BRS, FMA LE, BI, BBS, DGI and TIS for group 1.
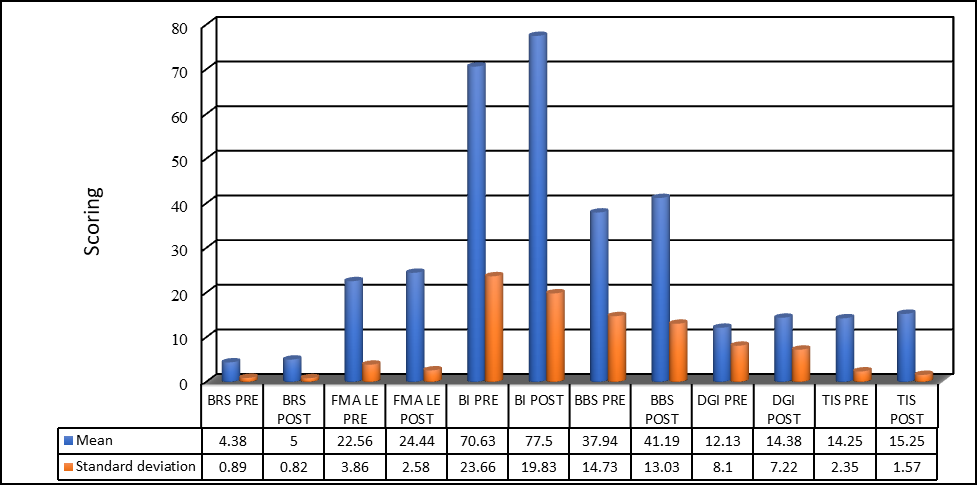
Graph 1: Mean difference within group comparison for Group 1.
Table 4 shows results of within group analysis for Group 2 using Wilcoxon Singed Ranks test to determine the difference between pre and post treatment. The analysis of pre- and post-treatment scores revealed significant improvements across all clinical measures. The mean Brunnstrom Recovery Stage (BRS) score increased from 5.00 ± 0.63 pre-treatment to 5.69 ± 0.70 post-treatment, with a p-value of 0.001, indicating statistical significance. Similarly, the mean Fugl- Meyer Assessment for Lower Extremity (FMA-LE) score improved from 24.25 ± 2.84 to 26.63 ± 2.13, with a p-value of 0.001, also considered statistically significant. For the Barthel Index (BI), the mean score rose from 85.94 ± 14.86 pre-treatment to 93.13 ± 9.81 post-treatment, with a p-value of 0.003, signifying a significant improvement in functional independence. The Berg Balance Scale (BBS) score showed a substantial increase from 48.88 ± 5.37 to 53.44 ± 2.63, with a p-value of 0.000, indicating highly significant progress in balance. The Dynamic Gait Index (DGI) also demonstrated a notable improvement, with the mean score increasing from 18.75 ± 2.18 to 22.19 ± 1.42, and a highly significant p-value of 0.000. Additionally, the Trunk Impairment Scale (TIS) score improved from 15.19 ± 1.42 to 16.44 ± 0.81 post- treatment, with a p-value of 0.003, considered statistically significant.
| Mean | SD | Mean difference | Z value | P value (<0.05 sig) | |
|---|---|---|---|---|---|
| BRS Pre | 5 | 0.63 | 0.69 | -3.317 | 0.001 |
| BRS Post | 5.69 | 0.7 | 0.69 | -3.317 | 0.001 |
| FMA LE Pre | 24.25 | 2.84 | 2.38 | -3.319 | 0.001 |
| FMA LE Post | 26.63 | 2.13 | 2.38 | -3.319 | 0.001 |
| BI Pre | 85.94 | 14.86 | 7.19 | -2.971 | 0.003 |
| BI Post | 93.13 | 9.81 | 7.19 | -2.971 | 0.003 |
| BBS Pre | 48.88 | 5.37 | 4.56 | -3.524 | 0 |
| BBS Post | 53.44 | 2.63 | 4.56 | -3.524 | 0 |
| DGI Pre | 18.75 | 2.18 | 3.44 | -3.528 | 0 |
| DGI Post | 22.19 | 1.42 | 3.44 | -3.528 | 0 |
| TIS Pre | 15.19 | 1.42 | 1.25 | -2.979 | 0.003 |
| TIS Post | 16.44 | 0.81 | 1.25 | -2.979 | 0.003 |
Table 4: Within Group Comparison for Group 2.
Graph 2 shows the pre- post comparison for BRS, FMA LE, BI, BBS, DGI and TIS for group 2
Graph 2: Mean difference within group comparison for Group 2.
Table 5 shows between group analysis for Group 1 and Group 2 using Mann-Whitney U Test with its z value and p<0.05 significance level.
| Outcome measures | Mean ± SD | MD | Z-value | P-value (<0.05 sig) | |
|---|---|---|---|---|---|
| Group 1 | BRS POST | 5±.82 | 0.69 | -2.546 | 0.011 |
| Group 2 | BRS POST | 5.69 ±.70 | 0.69 | -2.546 | 0.011 |
| Group 1 | FMA LE POST | 24.44 ± 2.58 | 2.19 | -2.201 | 0.028 |
| Group 2 | FMA LE POST | 26.63 ± 2.13 | 2.19 | -2.201 | 0.028 |
| Group 1 | BI POST | 77.5 ± 19.83 | 15.63 | -2.228 | 0.026 |
| Group 2 | BI POST | 93.13 ± 9.81 | 15.63 | -2.228 | 0.026 |
| Group 1 | BBS POST | 41.19 ± 13.03 | 12.25 | -2.479 | 0.013 |
| Group 2 | BBS POST | 53.44 ± 2.63 | 12.25 | -2.479 | 0.013 |
| Group 1 | DGI POST | 14.38 ± 7.22 | 7.81 | -2.623 | 0.009 |
| Group 2 | DGI POST | 22.19 ± 1.42 | 7.81 | -2.623 | 0.009 |
| Group 1 | TIS POST | 15.25 ± 1.57 | 1.19 | -2.551 | 0.011 |
| Group 2 | TIS POST | 16.44 ± .81 | 1.19 | -2.551 | 0.011 |
Table 5: Between Group Comparison for Group 1 and Group 2.
The comparison of post-treatment outcomes between Group 1 and Group 2 revealed statistically significant differences across all clinical measures. The mean difference in Brunnstrom Recovery Stage (BRS) between the two groups was 0.69, with a p-value of 0.011, indicating statistical significance. Similarly, the mean difference in the Fugl-Meyer Assessment for Lower Extremity (FMA-LE) was 2.19, with a p-value of 0.028, also considered significant. For the Barthel Index (BI), the mean difference between Group I and Group II was 15.63, with a p-value of 0.026, showing a significant improvement in functional independence. The mean difference in Berg Balance Scale (BBS) scores was 12.25, with a p-value of 0.013, indicating a significant improvement in balance.
The Dynamic Gait Index (DGI) showed a highly significant mean difference of 7.81 between the two groups, with a p-value of 0.009. Additionally, the mean difference in the Trunk Impairment Scale (TIS) was 1.19, with a z-value of -2.551 and a p-value of 0.011, considered statistically significant.
Graph 3 shows post comparisons for BRS, FMA LE, BI, BBS, DGI and TIS for both group 1 and group 2. The mean differences between Group 1 and Group 2 were plotted to assess the improvement between the two groups. In the between-group comparison of post-treatment scores for BRS, FMA-LE, BI, BBS, DGI, and TIS, Group II demonstrated significantly greater improvement than Group 1, with all results showing statistical significance. These findings indicate that Group 2, which received yoga and conventional physiotherapy, experienced superior improvements in gait, balance, static and dynamic trunk control, and lower limb function compared to Group I, which received only conventional physiotherapy.
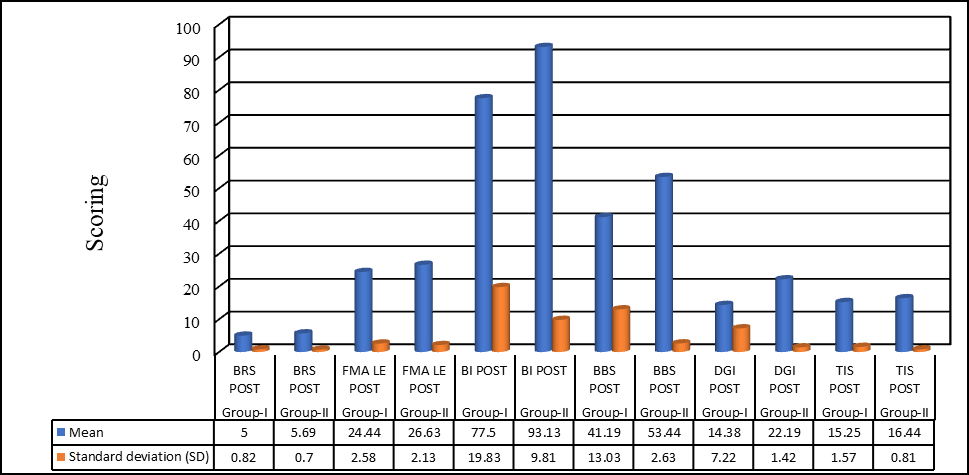
Graph 3: Mean difference between group comparison for Group-I and Group-II
Discussion
The primary finding of this study is that a 4-week regimen of yoga combined with conventional physiotherapy significantly improved lower limb function, gait, balance, and trunk control compared to conventional therapy alone. The slow, controlled movements and deliberate breathing in yoga, alongside a focus on lower limb weight-bearing and minimal upper extremity involvement, made the asanas accessible to patients and easy to learn, allowing them to perform the exercises independently.
Research by George J Salem, et al. [18] highlighted that older adults with weak ankle dorsiflexor strength have a higher risk of falling. Additionally, the hip abductors are crucial for pelvic stability, and their function correlates with fall risk. Hip flexors, which play a vital role in advancing the limb during the swing phase of gait, also contribute to walking speed and fall recovery. These muscle groups are essential for maintaining balance and gait, and in this study, the yoga asanas targeted these muscles effectively, stretching and strengthening them. The isometric muscular endurance of participants likely increased due to the extended holds in yoga postures, performed with controlled breathing. This practice engages the stabilizing muscles, recruiting different motor units to maintain the poses. Yoga postures that involve resistance and repetitive stretching improve proprioception by stimulating muscle, ligament, and joint receptors, including intrafusal fibers and Golgi tendon organs. Improved blood circulation to muscles and connective tissues further supports muscle flexibility. The static stretching nature of yoga asanas promotes elongation of muscle fibers through the addition of sarcomeres and plastic elongation of connective tissue [19]. Mark D Tran, et al. demonstrated that stretching enhances the efficiency of agonist muscles while decreasing neuromuscular activity in antagonist muscles, a process linked to increased oxidative enzyme activity and capillarization [20].
The yoga poses used in this study Bhujangasana, Adho Mukha Svanasana and Ashwa Sanchalanasana are integral to Suryanamaskara (Sun Salutation). These poses expand the chest and engage the abdominal muscles, helping to regulate breathing. Consistent breathing promotes mental clarity and self-awareness. Regular practice of these postures builds muscle strength and joint flexibility within a short period, benefiting spinal health and improving immunity. The alternating forward and backward bends in Suryanamaskara are particularly beneficial for the back, as they stretch and compress the spinal column, improving circulation and regulating nerve flow [21].
Previous studies on yoga in stroke rehabilitation indicate that these asanas activate core muscles, particularly the quadriceps, gluteus medius, minimus, and maximus. Yoga is a comprehensive workout for the body, mind, and spirit, strengthening the body, enhancing mental alertness, and promoting spiritual development by activating various energy centers. When performed slowly, yoga is calming; when performed quickly, it becomes energizing [22]. The improvements in balance, gait, trunk control, and lower limb function observed in the experimental group may be attributed to increased strength and endurance in the abdominal muscles, back extensors, hip abductors, hip flexors, quadriceps, and ankle plantar flexors. Additionally, enhanced lower limb range of motion, spine flexibility, and heightened concentration and self-awareness likely contributed to these functional gains [23].
Yoga has shown promising effects on functional recovery post-stroke, particularly in improving gait, balance, trunk control, and lower limb function. The combination of yoga postures and controlled breathing enhances strength, flexibility, and balance critical for gait and trunk control. Furthermore, yoga’s focus on mindfulness and body awareness improves proprioception, which is often impaired after stroke. Practicing yoga may also reduce spasticity and muscle stiffness, common post-stroke symptoms, thereby facilitating improvements in gait and trunk control [24].
Based on the findings of this study, it is suggested that yoga may be more beneficial when initiated during the acute and subacute phases of rehabilitation, rather than in the chronic phase. Early introduction of yoga may stimulate the formation of new neural pathways, aiding patients in learning new movements more easily, promoting earlier brain recovery, and facilitating neural plasticity [25].
This study has few limitations. We did not include a follow-up after the 4-week intervention period, limiting the understanding of the long-term effects of the treatment. Some participants faced challenges performing certain yoga asanas independently at home due to the need for assistance, which may have influenced the overall outcomes of the study. Future studies should incorporate follow-up assessments to evaluate whether the improvements observed are maintained over time and for how long. While this study focused on acute and subacute stroke patients, future research could explore the effects of yoga on chronic stroke populations to expand the applicability of the findings. Future research could also explore additional effects of yoga on stroke patients, such as its impact on coordination, mental health outcomes like depression and anxiety, stress reduction, and improvements in mood disorders.
Conclusion
After 4 weeks of treatment, significant improvements were observed in both groups across all outcome measures. While both groups, those receiving conventional therapy alone and those receiving conventional therapy combined with yoga showed improvements, the group receiving conventional therapy along with yoga demonstrated markedly greater improvements. The enhanced outcomes in the combined therapy group can be attributed to key components of yoga, such as synchronized breathing, weight-bearing postures, and stretching and strengthening exercises, which complemented conventional physiotherapy. These elements likely contributed to more substantial gains in gait, balance, trunk control, and lower limb functions. Thus, it can be concluded that combining conventional physiotherapy with yoga is more effective than conventional therapy alone in improving gait, balance, trunk control, and lower limb function in stroke patients.
Acknowledgement
Special thanks to all the subjects who willingly who were took part in this study.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent Statement
All the subjects who were took part in the study provided informed consent.
Data Availability Statement
The data that support the presented result can be received directly from the corresponding author who is in charge of deals with data storage.
References
-
Feigin VL, Forouzanfar MH, Krishnamurthi R, Mensah GA, Connor M, et al. (2014) Global and regional burden of stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. The Lancet 383(9913): 245-254.
-
Langhorne P, Bernhardt J, Kwakkel G (2011) Stroke rehabilitation. The Lancet 377(9778): 1693-1702.
-
Tyson SF, Rogerson L (2009) Assistive walking devices in nonambulant patients undergoing rehabilitation after stroke: the effects on functional mobility and walking impairments, and patients’ opinion. Archives of Physical Medicine and Rehabilitation 90(3): 473-478.
-
Pollock A, Baer G, Campbell P, Choo PL, Forster A, et al. (2014) Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochrane Database of Systematic Reviews (4): CD001920.
-
Sengupta P (2012) Health impacts of yoga and pranayama: A state-of-the-art review. International journal of preventive medicine 3(7): 444-458.
-
Scherer SA, Bauer AJ, Brixius K, Bloch W (2019) Effects of an eight-week yoga intervention on balance, mobility, and physical fitness in older adults. Journal of Sports Medicine.
-
Schmid AA, Van Puymbroeck M, Koceja DM, Page SJ (2012) Effects of a 12-week yoga intervention on fear of falling and balance in people with chronic stroke. Topics in Stroke Rehabilitation 19(3): 224-230.
-
Patel NK, Newstead AH, Ferrer RL (2012) The effects of yoga on physical functioning and health-related quality of life in older adults: a systematic review and meta- analysis. Journal of Alternative and Complementary Medicine 18(10): 902-917.
-
Lawrence ES, Coshall C, Dundas R, Stewart J, Rudd AG, et al. (2001) Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke 32(6): 1279-1284.
-
Huang CY, Lin GH, Huang YJ, Song CY, Lee YC, et al. (2016) Improving the utility of the Brunnstrom recovery stages in patients with stroke: validation and quantification. Medicine 95(31): e4508.
-
Hernández ED, Forero SM, Galeano CP, Barbosa NE, Sunnerhagen KS, et al. (2021) Intra-and inter-rater reliability of Fugl-Meyer Assessment of Lower Extremity early after stroke. Brazilian Journal of Physical Therapy 25(6): 709-718.
-
Della Pietra GL, Savio K, Oddone E, Reggiani M, Monaco F, et al. (2011) Validity and reliability of the Barthel index administered by telephone. Stroke 42(7): 2077-2079.
-
Dos Santos Barros V, Bassi-Dibai D, Guedes CL, Morais DN, Coutinho SM, et al. (2022) Barthel Index is a valid and reliable tool to measure the functional independence of cancer patients in palliative care. BMC Palliative Care 21(1): 124.
-
Conradsson M, Lundin-Olsson L, Lindelöf N, Littbrand H, Malmqvist L, et al. (2007) Berg balance scale: intrarater test-retest reliability among older people dependent in activities of daily living and living in residential care facilities. Physical therapy 87(9): 1155-1163.
-
Jonsdottir J, Cattaneo D (2007) Reliability and validity of the dynamic gait index in persons with chronic stroke. Archives of physical medicine and rehabilitation 88(11): 1410-1415.
-
Fujiwara T, Liu M, Tsuji T, Sonoda S, Mizuno K, et al. (2004) Development of a new measure to assess trunk impairment after stroke (trunk impairment scale): its psychometric properties. American journal of physical medicine & rehabilitation 83(9): 681-688.
-
Verheyden G, Nieuwboer A, Mertin J, Preger R, Kiekens C, et al. (2004) The Trunk Impairment Scale: a new tool to measure motor impairment of the trunk after stroke. Clinical rehabilitation 18(3): 326-334.
-
Salem GJ (2013) Weak ankle dorsiflexor strength and fall risk in older adults. Journal of Geriatric Physical Therapy.
-
Tran MD (2016) Stretching and muscle efficiency: A neuromuscular perspective. Journal of Sports Science.
-
Tran MD (2016) The effects of stretching on neuromuscular efficiency and oxidative capacity. Journal of Sports Medicine.
-
Iyengar BKS (2015) Light on Yoga. HarperCollins.
-
Field T (2016) Yoga research review. Complement Ther Clin Pract 24: 145-161.
-
Taylor MJ (2014) Core muscle activation during yoga asanas. Journal of Bodywork and Movement Therapies.
-
Saraswati SS (2017) Yoga and Neurological Rehabilitation. Satyananda Yoga Publications.
-
Cheung C (2018) Neural plasticity and stroke recovery: The role of early intervention. Journal of Stroke and Cerebrovascular Diseases.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial