The Effects of Aptamin® Mist on Skin Barrier Function, Skin Hydration, Pruritus VAS, and SCORAD Index in Mild Atopic Dermatitis
Moisturizers play a key role in the management of atopic dermatitis. This study aimed to evaluate the efficacy and safety of Aptamin® Mist on skin barrier function and skin hydration of participants with mild atopic dermatitis. Participants used Aptamin® Mist and Cetaphil® moisturizing cream to measure transepidermal water loss (TEWL), skin moisture content, visual analog scale (VAS) for evaluating pruritus, SCORing the Atopic Dermatitis (SCORAD) index, and Subject’s Global Assessment (SGA) were measured for 8 weeks. The moisture content of the test product significantly increased (p < 0.05), and the TEWL decreased (p < 0.05) after product use. The pruritus VAS score significantly improved (p < 0.017) after test product use. The SCORAD index of the test product significantly decreased (p < 0.05) after product use. In SGA, 95.652% participants reported an improvement in itchiness. In the safety assessments, no skin abnormalities were observed upon physical examination by a dermatologist. Using the test product, Aptamin® Mist, participants who had dry skin exhibited improvements in the skin moisture content, pruritus VAS score, and SCORAD index after 8 weeks. Thus, Aptamin® Mist is a potent ingredient for cosmeceutical developments in atopic dermatitis.
Soonhye Hwang1*, Mideum N Kim1, Areum Won1, Ji Hyun Kim1, Nuri Yang2, Jin Hee Shin2, Yoon‐Seong Kim1 and Jeong Hoon Kim1
Introduction
Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disease that is commonly associated with atopy. The disease typically presents in early childhood and is associated with dry, itchy skin [1, 2, 3, 4]. The impaired epidermal barrier associated with AD results in increased transepidermal water loss (TEWL) and reduced water holding capacity of the stratum corneum, which leads to an increased propensity for skin irritation and pruritus [5, 6, 7].
In practice, there are two important facets in the management of AD, namely, preventive and therapeutic measures. Preventive measures refer to proper and frequent skin lubrication by the topical application of moisturizers and bathing [8, 9].
However, when these preventive measures fail to control disease exacerbation, therapeutic measures such as topical/systemic corticosteroids, antibacterials, and various immunomodulating agents may be required to control skin inflammation [10, 11]. In steroid cases, AD causes many side effects, such as blood flow disorders, immune disorders, gastrointestinal disorders, and hormone secretion problems. For this reason, researchers are trying to develop new treatment options for AD that have fewer side effects [12, 13].
Cetaphil® RestoraDerm is the first and only regimen with advanced ceramide and filaggrin technology that helps replenish the skin barrier. Ceramides are composed of long- chain fatty acids that link with other important molecules to promote cellular function. Ceramides create a barrier to prevent permeability. Filaggrin functions in the formation of the corneocyte, and the generation of its intracellular metabolites contributes to the stratum corneum hydration [14, 15, 16, 17].
We conducted this clinical study on 47 participants who had very dry skin with itchiness and compared the effects of Aptamin® Mist with those of Cetaphil® RestoraDerm. We determined the efficacy and safety of Aptamin® Mist on skin barrier function, skin hydration, VAS assessment of pruritus, and SCORing of the Atopic Dermatitis (SCORAD) in participants with mild atopic dermatitis. This novel Aptamin® Mist, which contains Aptamin® C, improves skin barrier function, skin hydration, VAS assessment of pruritus, and SCORAD in this clinical study.
Materials and Methods
Study design and population
In this double-blinded, randomized, and controlled trial, 47 participants with dry skin under 29 (A.U.) by Corneometer® CM825 CM with mild AD were enrolled. Participants applied two products, Aptamin® Mist (Test Product; Nexmos Co. Ltd., Korea) and Cetaphil® RestoraDerm (Control Product; Galderma, Switzerland) (Table 1), to the area of the itching site and then dried regularly twice a day in the mornings and evenings for 8 weeks.
| Product | Ingredients | |
|---|---|---|
| Test | Aptamin® Mist | Water, s-DNA Aptamer-2 (Aptamin® C200), L-ascorbic acid, Hyaluronic acid, 1,2-Hexanediol |
| Control | Cetaphil® RestoraDerm Cream | Water, Glycerin, Caprylic/Capric Triglyceride, Sunflower Seed Oil, Pentyleneglycol, Shea butter, Cyclopentasiloxane, Cetearyl Alcohol, Sorbitol, Behenyl Alcohol, Glyceryl Stearate, Tocopheryl Acetate, Cetyl Alcohol, Arginine, Niacinamide, Disodium Ethylene Dicocamide PEG-15 Disulfate, Glyceryl Stearate Citrate, Sodium Polyacrylate, Caprylyl Glycol, Ceteareth-20, Sodium PCA, Allantoin, Citric Acid, Panthenol, Dimethiconol, Disodium EDTA, Sodium Hyaluronate, Hydroxypalmitoyl Sphinganine |
Table 1: Ingredients of investigated products.
Informed written consent was obtained before recruitment. The study protocol of the clinical study was submitted by the Chung-Ang University Industry Academic Cooperation Foundation, and ethical approval was obtained from the Institutional Review Board of P&K Skin Research Center.
Efficacy Assessments
Primary Efficacy
The skin hydration level was evaluated at the test area using a Corneometer CM825 (Courage-Khazaka electronic GmbH, Germany). The corneometer probe was connected to the skin to make sensor-based measurements, three times, and the averaged value was used as the skin hydration results. A corneometer measures the capacitance where the probe connects to measure the water content and presents excellent results in dry skin with low water content. It is possible to measure the water content uniformly at 30–40 µm under the corneum layer, where the effects of cosmetics or medications are few. The unit is A.U., and the value is proportional to the skin moisturizing amount.
TEWL was measured around the test area using a Vapometer (Delfin). It was measured once for 10 s, and the small TEWL value represented better skin status. It is possible to predict the skin water reserving function and skin water barrier function with the TEWL value, and the unit was g/m2h.
In the VAS score of pruritus, the pruritic participants were directly marked below the 10 cm line to record their level of itchiness on visits 1 to 4. The marks were measured each time and compared before and after using test products to evaluate the degree of itchiness.
Secondary Efficacy The degree of skin itchiness, area size, symptoms, and sleep disorder of the test participants were evaluated by a dermatologist at every visit. The modified SCORAD index (MSI) was calculated as follows.
Modified SCORAD Index (MSI) = ES/5 + 7x(IS/2) + SS
- Extend score (ES): Σ(rkr affected area of the measured area [%] × an area transmutation constant)
- Intensity score (IS): Sum of the scores on erythema, edema or papulation, exudation, crust, abrasion, lichenification, and skin dryness by researcher according to four grades: None (0), Weak (1), Moderate (2), and Severe (3).
- Subjective symptom score (SS): Sum of the scores on skin itchiness and sleep disorder according to 11 grades: 0–10.
After test product use, participants were evaluated according to the Global Assessment of Efficacy survey about the improvement of skin itchiness using the following parameters: very good (4), good (3), moderate (2), bad (1), and very bad (0). The researcher evaluated the efficacy of the test product with each answer’s percentage value.
The skin pH was measured once and was evaluated using the skin pH meter PH905. The skin pH represents the skin health status; the lower the pH, the more the skin acidity increases. As the skin pH increases and outranges the normal level of acidity, there is a greater possibility of skin bacteria or skin irritations. Skin temperature was evaluated using a Skin Thermometer ST500 (Courage-Khazaka electronic GmbH, Germany). It was measured three times, and the value was averaged to use as skin temperature (℃) data. The test area was photographed by DSLR before and after product use. Photographed pictures are attached for evaluating improvement in the skin before and after product use.
Safety Assessments
The safety of the test product was evaluated more than once for all participants who used the test products. Any adverse effects after product use and throughout the study period were considered together to determine the incidence of adverse events and to use as safety evaluation data. Any adverse effects were surveyed on each visit. If any events happened before the next visit, the study participant was directed to contact the researchers immediately. If an adverse effect occurred, the researcher informed the chief researcher. Then, the chief researcher evaluated the degree of symptoms and relationship with test products for further appropriate action and participation options.
Statistical Analysis
The statistical analysis package SPSS 19.0 was used to evaluate the efficacy of the test product for skin changes.
The significance level was set as 5% (i.e., p value < 0.05 was considered statistically significant). Probability was rounded to three decimal places. Continuous variables were summarized as the average with standard deviation, and categorical variables were summarized as the frequency and percentage. For measurements of more than three times, the parametric tests, for messing repeated measures ANOVA (post-hoc: Bonferroni correction), and the non-parametric test, Friedman test (post-hoc: Wilcoxon signed-rank test with Bonferroni correction), were used according to the statistical treatment for analysis. For between comparisons, the change rate compared with that before use was applied as evaluation data. Besides the parametric test, the independent t-test and the non-parametric test, Mann–Whitney U test, were used according to the statistical treatment for analysis.
Results
Study Population
The average age of 47 participants who participated in and finished the study was 30.574 years. Seven people were in their 10s, 21 were in their 20s, six were in their 30s, 11 were in their 40s, and two were in their 50s. All participants comprised 33 females and 14 males. Of them, 34 had dry skin and 13 had dry to normal skin. Selected participants did not show any adverse events nor medical or drug history.
Efficacy Assessments
Primary Efficacy
At the primary efficacy study, there was a significant increase in the skin moisture level of test group participants compared with that before treatment (Figure 1). The moisture content of the test product significantly increased (p < 0.05) at 2, 4, and 8 weeks after product use, compared with that before use. There were no significant differences at 2, 4, and 8 weeks after product use compared with the control product. As a result of the two products, the contents of skin moisture significantly increased (Figure 1, Table 2).
| Test product | Control product | |
|---|---|---|
| Before | 15.818 ± 7.841 | 16.185 ± 7.264 |
| 2 weeks after | 23.339 ± 10.566** | 26.201 ± 12.272** |
| 4 weeks after | 24.987 ± 11.871** | 27.236 ± 11.223** |
| 8 weeks after | 29.552 ± 12.209** | 29.414 ± 11.795** |
| Before | 5.652 ± 2.039 | 4.858 ± 2.059 |
| 2 weeks after | 4.674 ± 1.815## | 3.663 ± 2.533## |
| 4 weeks after | 3.474 ± 1.701## | 3.242 ± 2.448## |
| 8 weeks after | 1.648 ± 1.582## | 2.683 ± 2.566## |
Table 2: Measurement of the result of skin moisture, A.U. (Mean ± SD). **: p < 0.05 by repeated measures ANOVA, post-hoc Bonferro
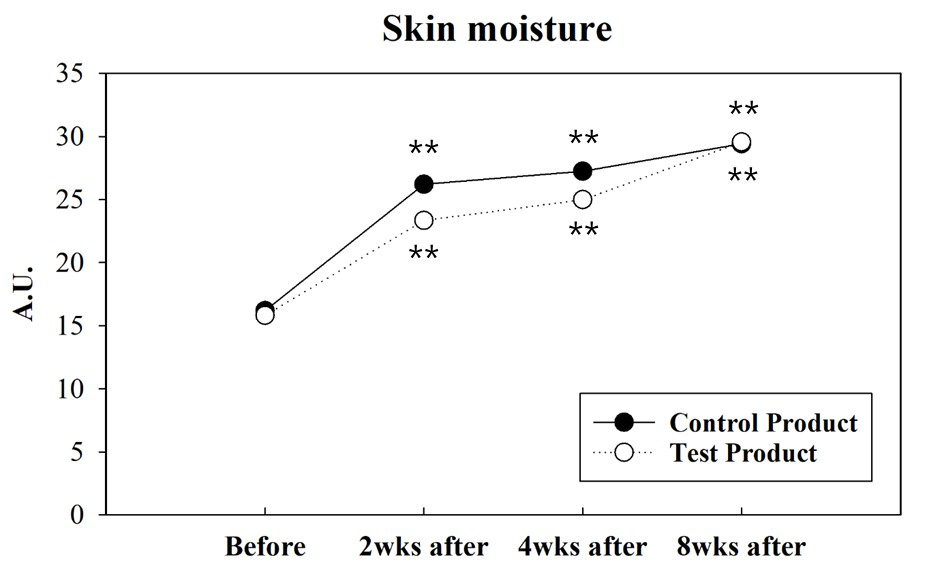
Figure 1: Measurement of skin moisture. The value of the test product significantly increased (p < 0.05) at 2, 4, and 8 weeks after product use, compared with before use. The value of the control significantly increased (p < 0.05) at 2, 4, and 8 weeks after product use, compared with before use. ** : p < 0.05 by repeated measures ANOVA, post-hoc Bonferroni correction The TEWL content of the test and control products significantly decreased (p < 0.05) 2 and 8 weeks after product use compared with before use. There were no significant differences 2, 4, and 8 weeks after product use compared with the control product (Table 3).
| Test product | Control product | |
|---|---|---|
| Before | 25.203 ± 13.493 | 27.668 ± 7.106 |
| 2 weeks after | 22.097 ± 8.242** | 27.340 ± 9.517 |
| 4 weeks after | 21.958 ± 8.729 | 27.926 ± 10.304 |
| 8 weeks after | 20.613 ± 7.936** | 25.915 ± 10.331 |
Table 3: Measurement of transepidermal water loss, g/m2h. (Mean ± SD). **: p < 0.05 by repeated measures ANOVA, post-hoc Bonferro
To confirm that strengthening the skin barrier by moisturizing the skin relieves itching, the following tests were conducted. A VAS score of pruritus was measured to compare the score before and after using test products to evaluate the degree of itchiness. The VAS score of the test product significantly decreased (p < 0.017) at 2, 4, and 8 weeks after product use, compared with before use. The VAS score of the control product significantly decreased (p < 0.017) at 2, 4, and 8 weeks after product use compared with before use. There was a statistically significant difference (p < 0.05) between the two groups at 8 weeks after product use (Figure 2, Table 4). Through the primary efficacy test, it was confirmed that Aptamin® Mist enhances skin moisture and relieves itching to protect the skin barrier.
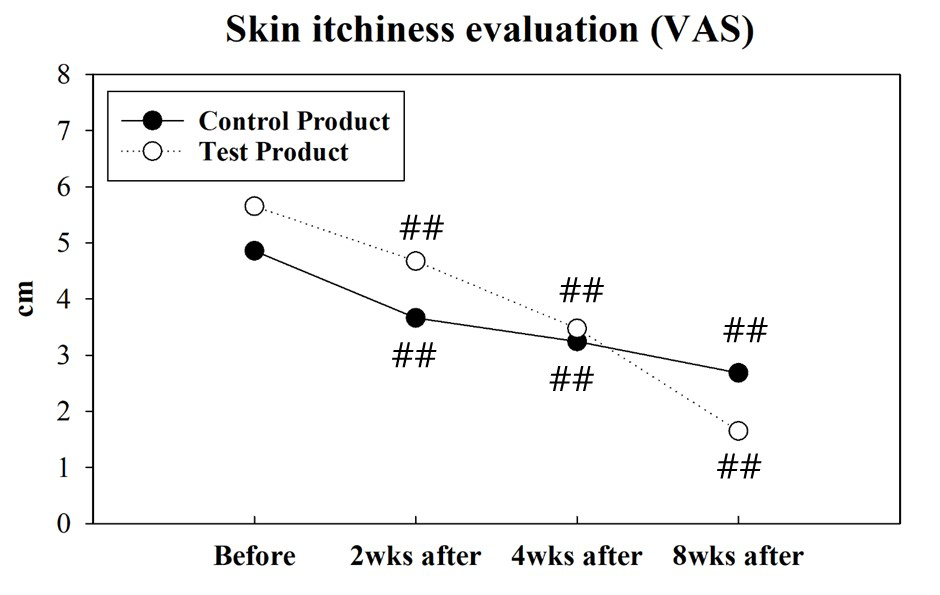
Figure 2: Measurement of skin itchiness (VAS). The value of the test product significantly decreased (p < 0.017) at 2, 4, and 8 weeks after product use, compared with before use. The value of the control product significantly decreased (p < 0.017) at 2, 4, and 8 weeks after product use, compared with before use. ##: p < 0.017(= 5%/3) by Friedman’s test, post-hoc Wilcoxon signed-rank test with Bonferroni correction.
Secondary Efficacy
During the secondary efficacy study, there was a significant decrease in the SCORAD index for the test group compared with before use (Figure 3). The SCORAD index of the test product significantly decreased (p < 0.05) at 2, 4, and 8 weeks after product use, compared with before use. There were no significant differences at 2, 4, and 8 weeks after product use, compared with the control product. As a result of the two products, the SCORAD index significantly decreased (Figure 3, Table 5).
| Test product | Control product | |
|---|---|---|
| Before | 40.134 ± 11.835 | 33.732 ± 10.821 |
| 2 weeks after | 33.301 ± 12.401** | 27.754 ± 12.015## |
| 4 weeks after | 28.345 ± 10.854** | 24.232 ± 9.352## |
| 8 weeks after | 23.046 ± 10.367** | 20.787 ± 11.696## |
Table 4: Measurement of the SCORAD index, MSI. (Mean ± SD). **: p < 0.05 by repeated measures ANOVA, post-hoc Bonferroni correcti
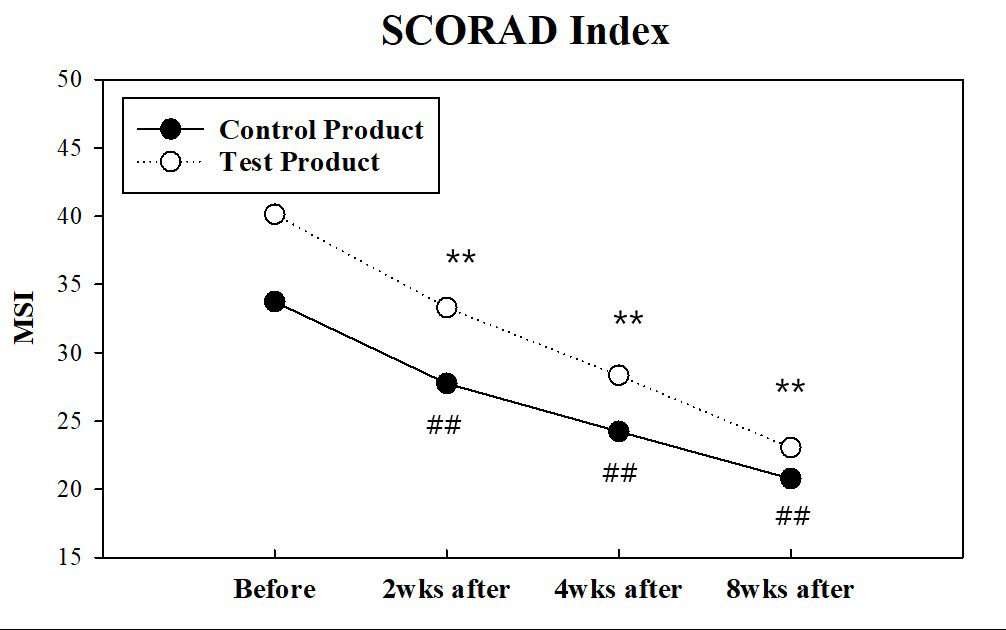
The value of the test product significantly decreased (p < 0.05) at 2, 4, and 8 weeks after product use, compared with before use. The value of the control product significantly decreased (p < 0.017) at 2, 4, and 8 weeks after product use, compared with before use.
**: p < 0.05 by repeated measures ANOVA, post-hoc Bonferroni correction.
##: p < 0.017(=5%/3) by Friedman’s test, post-hoc Wilcoxon signed-rank test with Bonferroni correction.
We conducted the Subject’s Global Assessment. The efficacy of the test product was surveyed after test product use to determine whether there was an improvement in skin itchiness. Based on the subject survey, the resulting values were calculated as percentages. As a result of the Global Assessment of Efficacy survey on the effect of improved skin itchiness the need to improve awareness of itching, 95.652% and 87.500% of the participants positively answered in the test and control group, respectively (Table 6).
The skin pH of the test and control products were not significantly different at 2, 4, and 8 weeks after product use compared with before use. There were no significant differences at 2, 4, and 8 weeks after product use, compared with the control product (Table 7). Both groups were not sensitive to pH and remained stable.
| Improvement effect on skin itchiness | Number of participants (percentage, %) | Average | Standard deviation | |||||
|---|---|---|---|---|---|---|---|---|
| 4 | 3 | 2 | 1 | 0 | ||||
| Test product | n | 5 | 13 | 4 | 1 | 0 | 2.957 | 0.767 |
| % | 21.739 | 56.522 | 17.391 | 4.348 | 0 | |||
| Control product | n | 4 | 8 | 9 | 2 | 1 | 2.5 | 1.022 |
| % | 16.667 | 33.333 | 37.5 | 8.333 | 4.167 |
Table 5: Result of the Global Assessment of Efficacy. 4: Very good, 3: Good, 2: Moderate, 1: Bad, 0: Very bad
| Test product | Control product | |
|---|---|---|
| Before | 6.963 ± 0.280 | 6.869 ± 0.328 |
| 2 weeks after | 6.845 ± 0.082 | 6.841 ± 0.133 |
| 4 weeks after | 6.853 ± 0.103 | 6.914 ± 0.228 |
| 8 weeks after | 6.903 ± 0.071 | 6.845 ± 0.149 |
| Test product | Control product | |
| Before | 31.091 ± 1.079 | 31.404 ± 1.182 |
| 2 weeks after | 31.030 ± 1.589 | 31.700 ± 1.142 |
| 4 weeks after | 31.022 ± 1.534 | 31.288 ± 1.355 |
| 8 weeks after | 30.987 ± 1.763 | 31.746 ± 1.081 |
| **: p < 0.05 by repeated measures ANOVA, post-hoc Bonferroni correction. | ||
| ##: p < 0.017(= 5%/3) by Friedman’s test, post-hoc Wilcoxon signed-rank test with Bonferroni correction. | ||
| ‡: There were no significant differences between the two groups (p < 0.05 by Mann–Whitney U test). |
Table 6: Measurement of skin pH. (Mean ± SD). ##: p < 0.017(=5%/3) by Friedman’s test, post-hoc Wilcoxon signed-rank test with Bo
The skin temperature of the test and control products were not significantly different at 2, 4, and 8 weeks after the product was used, compared with before use. There were no significant differences at 2, 4, and 8 weeks after product use, compared with the control product (Table 8).
**: p < 0.05 by repeated measures ANOVA, post-hoc Bonferroni correction.
##: p < 0.017(= 5%/3) by Friedman’s test, post-hoc Wilcoxon signed-rank test with Bonferroni correction.
‡: There were no significant differences between the two groups (p < 0.05 by Mann–Whitney U test).
Safety Assessments
Subject survey results and visual assessment by the researcher were evaluated after test product use. There was no report on adverse effects incurred by patients during the application period of rest from the test product. There were no skin abnormalities based on the physical examination administered by a dermatologist (Table 9). As a result of the participants surveyed about safety, there were no symptoms related to skin adverse effects (Table 10).
| Test product | Control product | |
|---|---|---|
| Erythema | ND | |
| Edema | ND | |
| Scaling | ND |
Table 7: Result of the visual assessment. Abbreviations: ND: Not detected.
| Test product | Control product | |
|---|---|---|
| Stinging | ND | |
| Burning | ND | |
| Tightness | ND | |
| Prickling | ND |
Table 8: Result of subject survey. Abbreviations: ND: Not detected.
Discussion
In this clinical trial, we demonstrated the clinical efficacy and safety of Aptamin® Mist in the treatment of mild AD. Aptamin® Mist significantly increased skin moisture and then reduced the pruritus of VAS and the SCORAD Index.
The mechanism by which the complex compound of Aptamin® C and vitamin C was effective against AD may be due to the synergistic effect of each component. The effect of vitamin C on AD was studied previously and could be explained by antihistamine and anti-inflammatory capacity [18, 19]. However, we used 0.1% of vitamin C (low dosage) in the Aptamin® Mist. Nevertheless, it was effective for moisturizing and relieving itching. Aptamin® C is an innovative DNA aptamer that maximizes the antioxidant efficacy of vitamin C by binding to the reduced form of vitamin C and delaying its oxidation [20, 21]. Furthermore, Aptamin® Mist demonstrated antioxidant capacity by inhibiting reactive oxygen species and anti-inflammation.
AD is a chronic, relapsing inflammatory skin disease that is commonly associated with atopy. The disease typically presents in early childhood and is associated with dry, itchy skin. In practice, preventive and therapeutic measures are the two most important facets in the management of AD. Preventive measures refer to proper and frequent skin lubrication by a topical application of moisturizers and bathing. However, when these preventive measures fail to control disease exacerbation, therapeutic measures such as topical/systemic corticosteroids, antibacterials, and various immunomodulating agents may be required to control skin inflammation.
This study provides clear evidence of the superiority of Aptamin® Mist in increasing skin hydration and decreasing the pruritus VAS and SCORAD index. Aptamin® Mist was manufactured in a minimum aqueous formulation consisting of water, s-DNA Aptamer-2, L-ascorbic acid, hyaluronic acid, and 1,2-hexanediol. We used a control product, Cetaphil® RestoraDerm moisturizer cream. This product is a cream formulation that is known to be excellent for atopy. It should be noted that there was a similarity between the Aptamin® Mist, which is a minimum aqueous formulation, and Cetaphil® RestoraDerm, which is a cream formulation.
Conclusions
Participants with dry skin who used the test product, Aptamin® Mist, showed improvement in the measurement of skin moisture content, SCORAD index, and VAS scale after 8 weeks of treatment. Using Aptamin® Mist, participants exhibited an approximately 116% improvement in the skin moisture content and a SCORAD improvement rate of
42%. Therefore, Aptamin® Mist is expected to be a potent ingredient for cosmeceutical developments in the treatment of AD.
References
-
Bieber T (2008) Atopic dermatitis. N Engl J Med 358(14): 1483-1494.
-
Bieber T (2010) Atopic dermatitis. Ann Dermatol 22(2): 125-137.
-
Thomsen SF (2014) Atopic Dermatitis: Natural History, Diagnosis, and Treatment 2014: 354250.
-
Rerknimitr P, Otsuka A, Nakashima C, Kabashima K (2017) The etiopathogenesis of atopic dermatitis: barrier disruption, immunological derangement, and pruritus. Inflamm Regen 37: 14.
-
Maeve K, Audrey DG, Jonathan OB H, Deirdre M, Linda EC, et al. (2015) Skin barrier dysfunction measured by transepidermal water loss at 2 days and 2 months predates and predicts atopic dermatitis at 1 year. J Allergy Clin Immunol 135(4): 930-935.
-
Linde YW (1992) Dry skin in atopic dermatitis. Acta Derm Venereol Suppl 177: 9-13.
-
Agrawal R, Woodfolk JA (2014) Skin barrier defects in atopic dermatitis. Curr Allergy Asthma Rep 14(5): 433.
-
Eichenfield LF, Tom WL, Chamlin SL, Feldman SR, Hanifin JM, et al. (2014) Guidelines of care for the management of atopic dermatitis. J Am Acad Dermatol 71(1): 116-132.
-
Wong ITY, Tsuyuki RT, Cresswell-Melville A, Doiron P, Drucker AM (2017) Guidelines for the management of atopic dermatitis (eczema) for pharmacists. Can Pharm J 150(5): 285-297.
-
Schandra P, Niken I, Retno D, Tatan S (2017) The Role of Moisturizers in Addressing Various Kinds of Dermatitis: A Review. Clin Med Res 15(3-4): 75-87.
-
Fougerousse AC (2021) At the Dawn of a Therapeutic Revolution for Atopic Dermatitis: An Interview with Dr Anne-Claire Fougerousse. Dermatol Ther (Heidelb) 1: 1-8.
-
Justine F, Nanette BS (2018) Oral supplements in atopic dermatitis. Clin Dermatol 36(5): 653-658.
-
Drucker AM, Eyerich K, de Bruin-Weller MS, Thyssen JP, Spuls PI, et al. (2018) Use of systemic corticosteroids for atopic dermatitis: International Eczema Council consensus statement. Br J Dermatol 178(3): 768-775.
-
Simpson E, Trookman NS, Rizer RL, Preston N, Colón LE, et al. (2012) Safety and Tolerability of a Body Wash and Moisturizer When Applied to Infants and Toddlers with a History of Atopic Dermatitis: Results from an Open- Label Study. Pediatric Dermatology 29(5): 590-597.
-
Simpson E, Dutronc Y (2011) A new body moisturizer increases skin hydration and improves atopic dermatitis symptoms among children and adults. J Drugs Dermatol 10: 744-749.
-
Jonca N (2019) Ceramides metabolism and impaired epidermal barrier in cutaneous diseases and skin aging: focus on the role of the enzyme PNPLA1 in the synthesis of v-O- acylceramides and its pathophysiological involvement in some forms of congenital ichthyoses. OCL 26: 17.
-
Cha HJ, He C, Zhao H, Dong Y, An IS, et al. (2016) Intercellular and intracellular functions of ceramides and their metabolites in skin (Review). Int J Mol Med 38(1): 16-22.
-
Johnston CS, Martin LJ, Cai X (1992) Antihistamine effect of supplemental ascorbic acid and neutrophil chemotaxis. J Am Coll Nutr 11(2): 172-176.
-
Ellulu MS, Rahmat A, Patimah I, Khaza’ai H, Abed Y (2015) Effect of vitamin C on inflammation and metabolic markers in hypertensive and/or diabetic obese adults: a randomized controlled trial. Drug Des Devel Ther 9: 3405-3412.
-
Alexander S, Vinoth S, Rafal D, George WJ, Batchelor RH, et al. (2018) Inhibition of vitamin C oxidation by DNA aptamers. Aptamers 2: 28-35.
-
Choi S, Han J, Kim JH, Kim AR, Kim SH, et al. (2020) Advances in dermatology using DNA aptamer “Aptamin C” innovation: Oxidative stress prevention and effect maximization of vitamin C through antioxidation. J Cosmet Dermatol 19(4): 970-976.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling