Evaluating the Long-Term Outcome of the Ablative Lasers in the Treatment of Facial Angiofibromas in Tuberous Sclerosis: A Two- Year Follow-Up Study
Background: Tuberous sclerosis (TS), a genetic multisystem disorder, is characterized by widespread hamartomas in multiple organs. The classic clinical symptoms consist of angiofibromas, epilepsy, and developmental delay. Dermatological change is one of the major features. Bilateral facial angiofibromas (FA), a common form of presentation, cause significant cosmetic, medical, and emotional problems. The emerging treatment for skin lesions is laser therapy. However, there is no report on the long-term outcome of combined use of ultra-pulse carbon dioxide (UPCD) laser and ablative fractional (AF) Er: YAG lasers to treat skin lesions in patients suffering TS. Methods: A retrospective study, conducted from March 2014 to July 2018, investigated 9 patients from the Northwest part of China who had TS treated with a sequential treatment of UPCD laser and AF Er: YAG laser. Results: The sequential use of the UPCD and AF Er: YAG laser is a safe and effective method for the treatment of FA in patients suffering TS with satisfactory long-term outcomes. Conclusions: The sequential use of the UPCD and AF Er: YAG laser is a safe and effective method for the treatment of FA in patients suffering TS with satisfactory long-term outcomes.
Introduction
Tuberous sclerosis (TS), a genetic multisystem disorder with a birth morbidity rate of 1 in 6000 to 10,000, is characterized by the widespread nonmalignant hamartomas in multiple organs, especially in the skin and central nervous system [1, 2]. The classic clinical triad consists of facial angiofibromas (FA), epilepsy, and developmental delay. However, dermatologic disorders are among the primary characteristics of TS occurring in about 90% of patients and appear shortly after birth [3], so different treatment methods associated with FA have been described in the literature [2,4-
7]. In our study, the choice of treatment for angiofibromas is laser therapy.
Recently, different lasers are available for the treatment of angiofibromas [4, 5, 6, 7], including Er: YAG, dye, and ultra- pulse carbon dioxide laser (UPCDL). Because of its full- thickness skin involvement, it is important, for FA treatment, to choose a modality that reaches the appropriate depth to improve the dermal fibrosis and vasodilatation while concomitantly treating the superficial nodules. Considering the Fractional Photothermolysis (FP) and different depth of penetration,we combine UPCD and AF Er: YAG lasers to treat FA, aiming to improve aesthetic results in patients affected by TS. Few studies sequential combining UPCD and AF Er: YAG lasers to treat skin lesions in the same patient, however, there is no report on the evaluation of long-term outcome we decided to apply this combination to 9 patients with TS.
Materials and Methods
Subjects
From 2014 to 2018, 9 patients (5 female and 4 male) all with facial AF from the Northwest part of came to our Skin & Laser Centre of the second affiliated hospital of Xi’an Jiaotong University, particularly FA. The mean age of the patients was 18.7 years (range 16–21 years) and Fitzpatrick skin type III to IV. All patients or their parents denied a family history of TS (Table 1). The patients were examined before the treatment. The diagnosis was based on diagnostic criteria identifying major and minor features (1). None of these patients presented with epilepsy, but all presented with failure in school, not ruling out emotional embarrassment.
| No. | Gender | Years | Family history (+/-) | Epilepsy (+/-) | Laser therapy | Treatment times | Follow-up (6 months) after the last sequence | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Evaluation of outcome | Recurrence/ complications | Satisfaction score | |||||||||
| Size | Numbers | Color | |||||||||
| 1 | F | 19 | - | - | UPCD/Er:YAG | 2 | 5 | 4 | 4 | No | 8 |
| 2 | F | 18 | - | - | UPCD/Er:YAG | 2 | 5 | 4 | 4 | No | 8 |
| 3 | F | 16 | + | - | UPCD/Er:YAG | 2 | 5 | 5 | 5 | No | 10 |
| 4 | F | 21 | - | - | UPCD/Er:YAG | 3 | 5 | 5 | 5 | No | 10 |
| 5 | M | 20 | - | - | UPCD/Er:YAG | 2 | 5 | 4 | 4 | No | 8 |
| 6 | M | 17 | - | - | UPCD/Er:YAG | 3 | 5 | 5 | 5 | No | 10 |
| 7 | F | 19 | - | - | UPCD/Er:YAG | 1 | 5 | 3 | 4 | No | 6 |
| 8 | M | 20 | - | - | UPCD/Er:YAG | 2 | 5 | 4 | 4 | No | 8 |
| 9 | M | 18 | - | - | UPCD/Er:YAG | 2 | 5 | 5 | 4 | No | 8 |
Table 1: Patient information and results of laser treatment.
FA, among the most frequently reported symptoms, was evident in all the patients. Physical examination showed that angiofibromas were located on the bilateral cheeks, nasolabial fold, nose, and a plaque on the forehead. The counts of the lesion were more than 20. In the majority of the patients, they were multiple, up to 0.5 cm in size. They appeared as fibrous lesions on the face, separated from each other. No patient previously had undergone any treatment.
Exclusion criteria included a history of hypertrophic scarring or keloid formation, isotretinoin therapy within 6 months, use of iron supplements or an anticoagulant, a history of active or recurrent herpes simplex, presence of infected skin lesions, a history of a photosensitivity disorder, pregnant or breastfeeding, suntan, Fitzpatrick skin type V or VI, or herpes simplex in the treatment area, use other light- based treatment and refusal to give signed informed consent.
The treatments were performed with the approval of the hospital’s medical ethics committee, and informed consent was obtained from all patients included in the study.
Operation
Before treatment, patients cleaned their face with mild soap and got topical anesthetic with a topical anesthetic applied 60min before treatment or a general anesthetic until patients cannot feel the pain. Sequential treatment of UPCD (Lumenis, U.S.A.) laser and AF Er: YAG (Sciton Profile, U.S.A.) lasers was performed. The first treatment was performed with UPCD laser to deal with the larger angiofibromas, at selected intensities ranging from 10 to 15 W and energy ranging from 50 to 100mJ according to the type of skin and different scan sizes, with no overlap. For the second treatment, AF Er: YAG laser was performed by fractional mode for residual nodules and the scanning mode with adjustable scanning depth and spot size to flatten the FAs. During the treatment, the area was wiped with saline- moistened gauze. Each patient received laser treatment by a single operator using an identical technique. The treatment was repeated every 6 months and the treatment times depended on patients. Every patient was followed up for 6 months and treated at least one time. The lesion size, counts, and color were evaluated based on the following classes: 1 (severe aggravation), 2 (mild aggravation), 3 (unvaried), 4 (mild improvement), and 5 (strong improvement).
Post-Operation
After completion of all the procedures, ice packs for 30- 60min, a topical growth factor for three to four times per day for the first 1 weeks, and collagen mask for 2 weeks were informed to promote the repair, and moisturizing cream and sunscreen were applied to the treated skin. A topical antibiotic was administered immediately and daily after treatment. Oral clarithromycin 500 mg twice daily was given for 6 days. To avoid the irritation of the treated area, patients were educated not to use topical retinoid creams. Every patient received an investigation to evaluate their discomfort derived from the skin lesions on the face during the 6 months of treatment.
Statistical analysis
Statistical analysis was performed by using Prism version 6.0 software (GraphPad, La Jolla, CA). Linear regression was used for the analysis of correlations between treatment sequences and satisfactory results.
Results
All 9 patients showed obvious improvement in their skin lesions. The effect was evident even after the first treatment. They all completed the study protocol. The treatments were well-tolerated by the patients, except that the UPCD laser resurfacing was more painful than the other laser treatments.
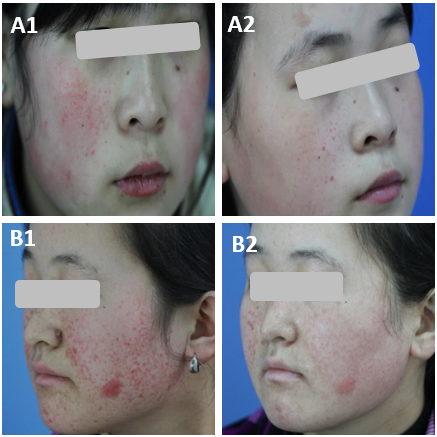
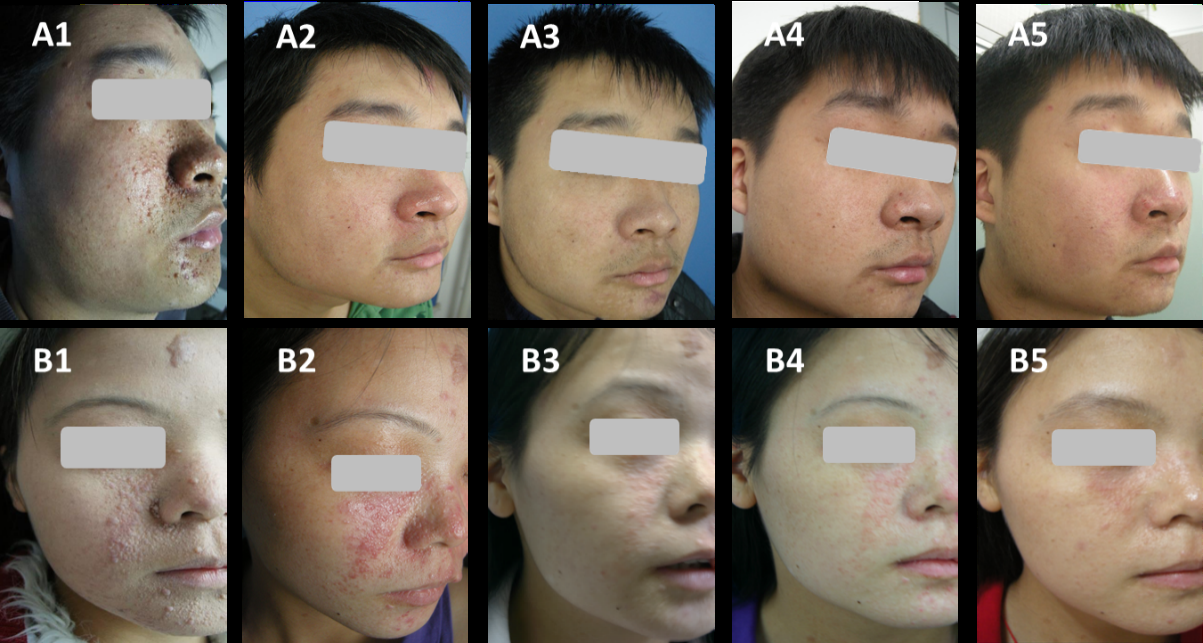
The clinical pictures of the patients before laser treatments and during follow-up visits at 6 months were evaluated by an experienced plastic surgeon who did not take part in the study. As shown in Table 1, which presents the results of laser treatment, three different parameters were considered: size, counts, the color of the lesion. The effect was obvious, reflecting the reduced size, counts, and color of lesions (Table1, Figure 1). To obtain the ideal effect, some patients chose more than one sequence.
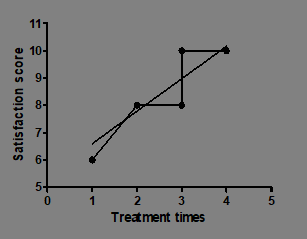
We also asked the patients to evaluate the results of their last sequential treatments with choices ranging from 1 (no improvement) to 10 (maximum improvement). Of the 9 patients, three (33.3 %) reported a score of 10, five (55.6 %) reported a score of 8, and one (11.1 %) reported a score of 6. There is a positive correlation between treatment sequences and satisfactory results (r2=0.8176, P=0.008. Figure 2).
Considering the appealing short-term effects after the sequential therapy treatment, we followed up with patients to evaluate the long-term effect. Phone calls were adopted and pictures were taken when they returned to the hospital.
Among 9 patients, 3 were lost follow-up, therefore, 6 were able to undergo follow-up. For all 6 patients, 5 had follow-up for 2 years and remained desirable results (Figure 3) while 1 experienced recurrence 2 years later.
Side effects were limited to transient erythema, edema, and minor bleeds in each patient. No patients showed infection, scarring, or signs of hyperpigmentation or depigmentation.
Discussion
This is the first study, to the best of our knowledge, to investigate the effectiveness of sequential use of UPCD and AF Er: YAG lasers to treat facial AF. All the patients obtained great improvement even after the first laser therapy, as indicated by corresponding fall in size, counts, and color of lesions. There were only transient erythema, edema, and minor bleeds in all patients, which were relieved within one week. No permanent side effects, such as infection, hyperpigmentation, hypopigmentation, and scarring, were fed back.
Up to now, lasers have become a popular treatment option and many laser therapies were available for patients with facial AF. However, it is still a challenge for FA treatment because of not complete removal, higher recurrence as well as permanent sides. As its superficial penetration, the copper vapor and argon lasers are only useful for flat red AF [5]. On the other hand, the higher electrical power of argon laser causes thermal injury and digital vascular dysfunction [8]. The pulsed dye is mainly for flat vascular- type AF because of its selective destroy of blood vessels [9]. Considering its heat diffusing out into adjacent tissue, which leads to hypertrophic scarring, continuous wave CO2 laser is restricted [10]. To remove superficial lesions, improve the deep structure of angiofibromas and speed up the healing, we creatively combined two different lasers, UPCD and AF Er: YAG lasers, to treat FA in TS patients.
As for UPCD laser, because of its predominant coagulative and necrotic effect [11], it is a common method for the treatment of FAs, especially for the big lesion. On the other hand, UPCDL leads to homeostasis by sealing the small cutaneous blood vessels, which, to some extent, reduces the risk of edema, hematoma, and infection. To reduce the risk of hyperpigmentation and scar caused by heat impacting of UPCD laser and speed up the healing process, we chose UPCD laser for raised and big size lesions only one pass, which restricted its deep action. Then, we chose AF Er: YAG laser to damage the root of lesions.
The AF Er: YAG laser, with a wavelength of 2940 nm, is absorbed by the superficial skin layers, hence the depth of penetration is only 1μm. But the tissue ablation with an Er: YAG laser does not exhibit necrotic areas, permitting multiple passes without dehydration or necrosis during the same session [12]. Besides, Sciton Profile Er: YAG system showed that multiple passes produce photothermally related effects in the dermis [13], thus can do harm to the deeper lesions.
In our study, a topical anesthetic or general anesthetic was applied depending on patients’ choice before the use of UPCD and Er: YAG lasers. Considering the longer time for treatment and obvious pain during treatment, general anesthesia was more optimal, which not only greatly reduced the intraoperative pain, but did a favor to complete the removal of skin lesions. Therefore, anesthesia, to some degree, influenced the effect. The patient who experienced relapse was probably because of the intolerable pain led by topical anesthetic and only one sequential treatment.
We have used two different lasers on the same patient, combined the horizontal effect (coagulative and necrotic effect) and vertical effect (depth), to improve the FA. The AF Er: YAG laser reduced lesion thickness, while the UPCD laser improved the size, the counts, and the color of the FAs. Of course, further studies with larger sample sizes and objective evaluation of histological changes were needed to evaluate the clear effect.
Conclusion
Our observations demonstrate that the sequential use of UPCD and AF Er: YAG lasers is an effective and safe treatment for FA in patients affected by TS, with satisfactory long-term outcomes.
Funding
The National Natural Science Foundation of China (Project No. 81803137), the new seedlings of science and technology in the Second Affiliated Hospital of Xi’an Jiaotong University (No. RC(XM)201807).
Competing Interests
The authors declare no competing interests.
Ethical Approval
The treatments were approved by the hospital’s medical ethics committee.
Informed consent
All patients provided written informed consent before their inclusion in the study.
Conflict of interest
The authors declare no conflict of interest.
References
-
Randle Stephanie C (2017) Tuberous Sclerosis Complex: A Review. Pediatric Annals 46(4): e166-171.
-
Kohrman MH (2012) Emerging treatments in the management of tuberous sclerosis complex. Pediatr Neurol 46(5): 267-275.
-
Jacks SK, Witman PM (2015) Tuberous Sclerosis Complex: An Update for Dermatologists. Pediatric Dermatology 32(5): 563-570.
-
Salussolia CL, Klonowska K, Kwiatkowski DJ, Sahin M (2019) Genetic Etiologies, Diagnosis, and Treatment of Tuberous Sclerosis Complex. Annual Review of Genomics and Human Genetics 20(1): 217-240.
-
Ma G, Wu P, Lin X, Chen H, Li W, et al. (2014) Nd:YAG laser for “fractional” treatment of angiofibromas. Int J Dermatol 53(5): 638-642.
-
Biondo G, Greco S, Mavilia L, Mercuri SR (2014) Treatment of nodular facial angiofibromas in tuberous sclerosis, using ultrapulse carbon dioxide laser. Clin Exp Dermatol 39(6): 738-740.
-
Fioramonti P, De Santo L, Ruggieri M, Carella S, Federico LT, et al. (2014) Co2/Erbium:YAG/Dye laser combination: an effective and successful treatment for angiofibromas in tuberous sclerosis. Aesthetic Plast Surg 38(1): 192- 198.
-
Pauling JD, Shipley JA, McHugh NJ (2010) Impaired digital vascular function mimicking Raynaud’s phenomenon as a complication of argon laser therapy in tuberous sclerosis. Microvasc Res 80(1): 2.
-
Mills C, Lanigan S (1995) Treatment of multiple angiofibromata with the pulsed dye laser. Journal of Dermatological Treatment 6(4): 237-238.
-
Papadavid E, Markey A, Bellaney G, Walker NPJ (2002) Carbon dioxide and pulsed dye laser treatment of angiofibromas in 29 patients with tuberous sclerosis. Br J Dermatol 147(2): 337-342.
-
Xu Y, Deng Y (2018) Ablative Fractional CO2 Laser for Facial Atrophic Acne Scars. Facial Plast Surg 34(2): 205- 219.
-
El-Khalil H, Alzanina M, Lweesy K, Alshare A (2019) Investigation of laser pulsing parameters’ importance in Er:YAG laser skin ablation: a theoretical study conducted via newly developed thermo-mechanical ablation model. Int J Hyperthermia. 36(1): 613-624.
-
Trelles MA, Vélez M, Mordon S (2008) Correlation of histological findings of single session Er:YAG skin fractional resurfacing with various passes and energies and the possible clinical implications. Lasers Surg Med. 40(3): 171-177.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling