Diagnostic Usefulness of Dermoscopy in Differentiating Lichen Planus Pigmentosus from Ashy Dermatosis
Lichen planus pigmentosus is considered a rare variant of lichen planus. It is characterized by acquired dark brown to gray macular pigmentation localized on sun-exposed areas. As lichen planus pigmentosus, ashy dermatosis is also characterized by pigmented lesion and is commonly found in dark-skinned patients. It can be difficult to distinguish lichen planus pigmentosus from ashy dermatosis by the naked eye (1). Dermoscopy can be applied to skin lesions, revealing additional features that can be highly valuable for correct diagnosis. Skin lesions were evaluated via polarized dermoscopy. On dermoscopy, a brownish background with brownish – blackish globules and dots with a linear distribution were found in lichen planus pigmentosus. A bluish background with small bluish dots and globules and white areas were seen in ashy dermatosis. Dermoscopy could provide valuable information for the diagnosis of LPP and aids in differentiating it from ashy dermatosis.
El Kadiri S*, Baybay H, Douhi Z, Elloudi S and Fatima-Zahra M
Introduction
Lichen planus pigmentosus (LPP) is considered a rare variant of lichen planus. It is characterized by acquired dark brown to gray macular pigmentation localized on sun-exposed areas but also on unexposed areas. As lichen planus pigmentosus, ashy dermatosis is also characterized by pigmented lesion and is commonly found in dark-skinned patients. It can be difficult to distinguish LPP from ashy dermatosis by the naked eye [1].
Patients and observations
Case 1 A 15-year-old Moroccan boy presented with several itchy, brown-grayish, macules on his trunk and neck. The clinical examination found 0.5 – to 4.5 cms grayish, smooth, and well-defined macules (Figure 1a). Dermoscopy showed a brownish background with brownish – blackish globules and dots with a linear distribution (Figures 1b and c).

Figure 1a: Lichen plans pigmentosus . clinical image showing multiple brown—grayish macules on his trunk and neck.

Figure 1b: Dermoscopic image showing a brownish background with brownish- blackish globules and dots with a linear distribution ( Dermlite DL4, polarized mode).
Figure 1c: Dermoscopic image with high magnification.
Figure 1d: Histopathological examination showing pigmentary incontinence, melanophages, and a superficial perivascular lymphocytic infiltrate.
Histopathological examination of the biopsy samples showed pigmentary incontinence, melanophages, and a superficial perivascular lymphocytic infiltrate (Figure 1d). These features were compatible with the diagnosis of LPP. The patient was treated with Kligman’s formula with a 50% improvement.
Case 2 A 24-year-old Moroccan girl presented since 1 year with asymptomatic, grayish macules in the abdomen. She reported that they were initially erythematous without previous application of topical agent or plant. The clinical examination showed roundish 1- to 4 cms, grayish smooth macules in the abdomen (Figure 2a).
Figure 1a: Ashy dermatosis. clinical image with grayish macules in the abdomen.
Figure 2b: Ashy dermatosis. Dermoscopic image showing bluish background with small graiysh dots, whitish areas and rosettes (Dermlite DL4, polarized mode).
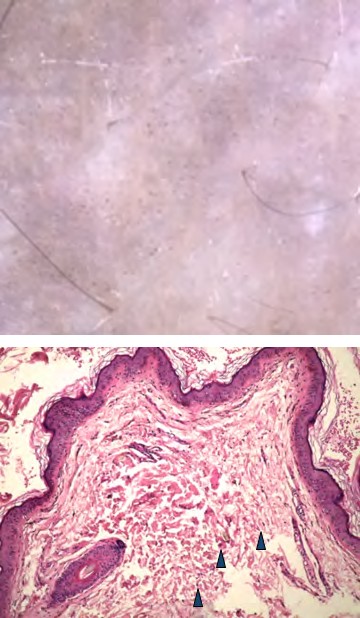
Figure 2c: Ashy dermatosis. Dermoscopic image with high magnification.
Figure 2d: Ashy dermatosis. Histopathological examination showing a pigmentary incontinence, melanophages without vacuolization of the basal cell layer.
Dermoscopy showed a bluish background with small bluish dots and globules with no particular distribution, white areas and rosettes (Figures 2b and c). Histopathological examination of the biopsy samples showed a pigmentary incontinence, melanophages without vacuolization of the basal cell layer (Figure 2d). These features were compatible with the diagnosis of ashy dermatosis. The patient was treated with topical tacrolimus with a 25% improvement.
Discussion
LPP is a rare disease considered as a variant of lichen planus and ashy dermatosis is also a rare inflammatory skin disease [1]. The two entities were thought to be the same pathology with two different names [2]. Some authors added Riehl’s melanosis classified them as acquired dermal macular hyperpigmentation [3]. They both have a chronic benign course of unknown etiology. Ashy dermatosis affects dark-skinned people, especially women in their first or second decade of life. LPP can affect the pediatric population and people until the 6th decade. Clinical presentation of LPP is characterized by frequently pruriginous gray brownish macules. Unlike LPP, ashy dermatosis is frequently asymptomatic and characterized by an erythematous phase which is often unnotified. In practice, these features are not always perceived by the patient [1]. Dermoscopy has been reported before to distinguish the two conditions [4]. Analyzing the background is very useful and essential in pigmentary disorders [5]. In LPP, the background is brownish contrary to AD which is more gray or bluish. This is correlated histopathologically to the presence of melanophages and melanin in the dermis [1]. In LPP, the deposit is more superficial compared to AD. The blue color is due to the Tyndall effect. The second feature to analyze is the size and color of dots and globules. In LPP they are larger and brownish than AD which they are small and grayish [4].
Conclusion
LPP and AD are two mysterious and constitutes a dilemma in practice to us dermatologists. Dermoscopy can be a clue for diagnosis allowing adequate therapeutic management.
References
-
Juan Carlos Robles-Méndez, Paulina Rizo-Frías, Maira Elizabeth Herz-Ruelas, Amit G Pandya, Jorge Ocampo Candiani (2018) Lichen planus pigmentosus and its variants: review and update. Int J Dermatol 57(5): 505- 514.
-
Vega ME, Waxtein L, Arenas R, Hojyo T, Dominguez-Soto L (1992) Ashy dermatosis and lichen planus pigmentosus: a clinicopathologic study of 31 cases. Int J Dermatol 31(2): 90-4.
-
Sarita Sasidharanpillai, Aparna Govindan, Kidangazhi Yathmana Ajithkumar, Saranya T Mahadevan, Valiyaveettil Bindu, et al. (2019) Histological Evaluation of Acquired Dermal Macular Hyperpigmentation. Indian Dermatol Online J 10(5): 542-546.
-
Enzo Errichetti, Vito Angione, Giuseppe Stinco (2017) Dermoscopy in Assisting the Recognition of Ashy Dermatosis. JAAD Case Rep 3(6): 482-484.
-
Vinod Kumar Sharma, Vishal Gupta, Piyush Pahadiya, Kamal Kumar Vedi, Sudheer Arava, et al. (2017) Dermoscopy and patch testing in patients with lichen planus pigmentosus on face: A cross-sectional observational study in fifty Indian patients. Indian J Dermatol Venereol Leprol 83(6): 656-662.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling