Skin Leishmaniasis in an Infant in Bangui: First Documented Local Case in the Capital City of the Central African Republic and History of the Disease in the Country
The aim of this work was to report the first case of cutaneous leishmaniasis observed in an infant residing in the city of Bangui. A 12-month-old infant, residing in Bangui, was brought in for consultation on September 11, 2020 for ulcerated budding lesions. The history of the disease is said to date back to May 2020 (4 months) with papules that have grown to ulcerate secondarily. The careful interrogation did not find any notion of displacement out of town or of a similar injury in those around him. Physical examination showed ulcerations 3 to 5 cm in diameter, thickened margin, granulomatous background in places, covered with scabs or serum in the limbs; the hypotheses of leishmaniasis, yaws, tuberculosis and sarcoidosis have been mentioned. Histology found kinetoplasts and the parasitological sample showed very many amastigotic forms of leishmanias. Treatment with metronidazole failed and the child was referred for pentamidine. This case of leishmaniasis in an infant who has never left the city of Bangui the capital suggests the possibility of the disease spreading throughout the country
Introduction
Cutaneous leismaniasis are parasitic diseases with cutaneous tropism, linked to the inoculation of leishmanias by sandfly bite [1, 2]. The spread of leishmaniasis is worldwide with approximately 350 million people exposed, 12 million cases and an annual incidence of 400,000 new cases for 30,000 deaths; only Australia and the Antarctic are spared [3]. The visceral form without treatment progresses to death in 95% of cases. There is a classification according to clinical picture, regions and species (visceral leishmaniasis in Asia, the New World, Africa; cutaneous leishmaniasis of the old world and cutaneous or cutaneous-mucous leishmaniasis of the New World). Old world cutaneous leismanioses are generally caused by Leishmania (L) major, responsible for the Oriental bud in its classic wet or rural form, L tropica responsible for a dry form with a human reservoir and L aetiopica which may be at the origin of cutaneous forms in southern Europe and the Maghreb [3, 4]. The first case of leishmaniasis reported in the Central African Republic in
2003 was imported from Amtiman, southern Chad [5]. The aim of this work was to report the first case of cutaneous leishmaniasis observed in an infant residing in the city of Bangui.
Observation
A 12-month-old female infant residing in Galabadja sinistré quarter, 8th district of Bangui was brought in for consultation on September 11, 2020 for ulcerated budding lesions. The history of the disease is said to date back to the beginning of May 2020 (4 months) with papules which have grown to ulcerate secondarily. The careful interrogation did not find any notion of displacement out of town or of a similar injury in those around him. He was unsuccessfully treated in a health center with ampicillin, gentamycin and ceftriaxone. Physical examination showed ulcerations 3 to 5 cm in diameter, thickened margin, granulomatous background, in places covered with scabs or serum in the limbs (Figure 1).

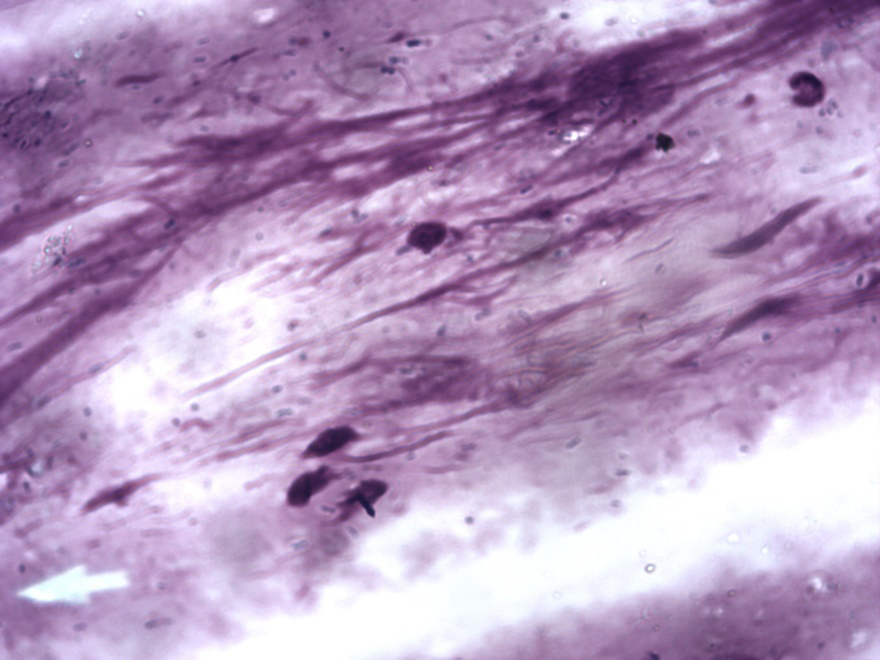
The hypotheses of leishmaniasis, yaws, tuberculosis and sarcoidosis have been mentioned. Histology found an acanthotic epidermis; the dermis, which is the site of a predominantly histiocytic polymorphic granuloma. There is no suppuration; Examination of macrophages has sometimes shown cytoplasmic inclusions which may be necessary for kinetoplasts. There is no sign of malignancy. The histology conclusion was in favor of leishmaniasis and the parasitological sample taken on November 2, 2020 showed very many amastigotic forms of leishmanias (Figure
3). The HIV serology came back negative. The child was put on metronidazole 40 mg / kg / day for 20 days and local treatment with polyvidone iodine without success; the lesions multiplied and worsened. Faced with this worsening, the child was referred to pediatrics for the possibility of starting an antimony derivative or Amphotericin B; unfortunately these molecules were not available. The dermatology service was obliged to refer him to the neglected tropical diseases department for the benefit of pentamidine from the tripanosomiasis program. The child returned 2 weeks later without treatment and with new lesions on the rest of the body including the scalp. Faced with this situation, we proposed her evacuation to the Bamako Dermatological Hospital in Mali for medical treatment and surgical repair of the deformities of the feet. Unfortunately, the child died during the medical evacuation procedures.


Discussion
This case concerns a female infant. Cutaneous leishmaniasis affects both sexes and all age groups. However, the sex ratio is frequently in favor of males and the age groups most affected are those from 0 to 15 years [6, 7, 8]. The infant had never left Bangui town or been to outlying areas. It is most likely a local, urban case, which testifies to the presence of infected sandflies in the city and of a possible reservoir. According to the WHO [7] and certain authors [9, 10] the first case of visceral leishmaniasis was reported in the country (Ubangui Chari) in 1949, a second case confirmed in a child in the Bangui region and 3 others in 1969 [11]. The first case imported into the Central African Republic from Amtiman (southern Chad) was reported 17 years ago by Kélémbho, et al. [5]. Another case on a nurse from Birao (North East of the country, on the border of Chad and Sudan) was observed in the dermatology department in 2005 without this being reported (Figure 4). Since that time, politico-military events have shaken Chad and the Central African Republic causing displacement of populations on both sides including the sending of Chadian soldiers to Bangui and the return of Central African refugees from Chad. Indeed, it is known that climatic and environmental changes, associated with population movements, create favorable conditions for the emergence of leishmaniasis [7, 12]. The lesions were on the exposed areas and were moist, similar to the case of Kélémbho, et al. [5]. The clinically suggested diagnosis, guided by histology, was confirmed by parasitology as is often the case [3, 13]. The species diagnosis was not possible for technical platform reasons. However, the species identified by Kélémbho, et al. was L. major. Heid also reported that L. major is common in urban areas [3]. The infant was put on metronidazole. Kélémbho, et al. [5] obtained a cure within 3 weeks of treatment with metronidazole. However, the WHO retains the protocol for antimony derivatives [3].
Several trials have concerned the use of antimycotics including ketoconazole, itraconazole and liposomal amphotericin B. Some authors speak of pentamidine [3]. Local medicinal and physical treatments are also available depending on the clinical aspects and the field with variable results [6]. Failure of metronidazole treatment for 3 weeks suggests the presence of a species other than L. major from Kélémbho, et al. The provision of central laboratories with species diagnostic products and antimines is needed in the country.
Conclusion
This case of cutaneous leishmaniasis in an infant who has never left the city of Bangui, the capital, suggests the possibility of local circulation of the disease requiring an epidemiological investigation and special attention in view of the establishment of the disease. A specific program to combat this disease.
References
-
Wery M (1995) Protozoologie médicale, Université francophone. De Boeck-Larcier, Bruxelles, pp: 123.
-
Dedet JP (2000) La lesihmaniose. Presse Med 29: 1019.
-
Heid E (1999) Dermatologie et infections sexuellement transmissibles. Jean-Hilaire S, Edouard G, Paul L, Jean- Marie L (Eds.), 4th (Edn.), Paris.
-
Aoun K, Abda IB, Bousslimi N, Bettaieb J, Siala E, et al. (2012) Caractérisation comparative des trois formes de leishmaniose cutanée endémiques en Tunisie. Annales de Dermatologie et de Vénéréologie 139(6-7): 452-458.
-
Kassa-Kelembho E, Kobangue L, Huerre M, Morvan JM (2003) Premier cas de leishmaniose cutanée d’importation à Bangui en République Centrafricaine: efficacité du métronidazole. Med Trop 63: 597-600.
-
Gangneux JP (1999) Traitement de la leishmaniose viscérale : modalités récentes. Presse Med 28: 2057- 2066.
-
OMS. La leismaniose: principaux faits.
-
Agarbi Fatima Zzahra (2013) La leishmaniose cutanée; aspects clinique, thérapeutique et évolutif (a propos de 40 cas). Mémoire de spécialité en dermatologie, FES, MAROC
-
Desjeux P(1991) Information on the epidemiology and control of the leishmaniasis by country or territory.
-
Bernard BOUA (2010) Programme national de lutte contre les maladies tropicales négligées en République Centrafricaine, Ministry of Health ; Conultative Meeting on the contol of leishmaniasis in the African Region WHO/AFRO Addis Ababa.
-
Cagnard V, Lindrec A (1969) A case of vl in bangui, central african republic. Med Trop 29(4): 531-535.
-
Maazoun R, Lanotte G, Pasteur N, Rioux JA, Kennou MF, et al. (1981) Écologie des Leishmanioses dans le sud de la France-16. Contribution à l’analyse chimiotaxonomique des parasites de la leishmaniose viscérale méditerranéenne. A propos de 55 cas. Annales de Parasitologie humaine et comparée 56(2): 131-146.
-
Slaheddine Belhadj J, Hone Hicheri-Helali, Kalthoum Kallel, Emira Kaouech, Hajer Abaza, et al. (2005) Place de la culture dans le diagnostic Parasitologique des leishmanioses Viscé rales et cutanées: expérience tunisienne. Revue Française des Laboratoires 369: 41- 44.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling