The Effectiveness of Virgin Coconut Oil Application on Improving the Skin Integrity of Preterm Infants; Systematic Review and Meta-analysis with Parameters Neonatal Skin Condition Score
Preterm infants have a greater susceptibility to serious infections because their skin barrier has not fully functioned properly. Early birth in preterm infants causes immaturity of the barrier development, in the form of a thinner stratum corneum. Therefore extra care is needed to maintain the integrity of their skin to prevent infection, where the main recommendation is the administration of emollients, such as coconut oil. Virgin coconut oil contains nutrients and lauric acid that are more maintained and higher than coconut oil. Changes in skin integrity can cause extensive skin damage and become risk factors for infection. Erythema or damage to the skin such as erosion, excoriation, or crusting can be an early symptom of life-threatening infection in preterm infants. Assessment of skin integrity can be assessed objectively using the Neonatal Skin Condition Score (NSCS). Virgin coconut oil as an emollient with its antimicrobial activity is expected to allow improvement of the barrier structure of the skin. Aim: The purpose of this study was to review previous studies to provide a systematic summary of the effectiveness of topical coconut oil in improving the skin integrity of premature infants. Methods: Searching the electronic database Pubmed-MEDLINE, Scopus, ProQuest, Cochrane library, ClinicalTrials.gov, and Google Scholar, found five most relevant articles included in the qualitative and two of those five articles included in the metaanalysis. Results: The meta-analysis of the effect of topical VCO compared with control on NSCS values in preterm infants showed the value of heterogeneity test with Tau2=0.04 df=1; p=0.13, I2=55%. The value of the Q statistic was z value = 5.23 (p < 0.001). This shows that the overall administration of topical VCO can significantly improve the value of NSCS on preterm infants. The results of the overall meta-analysis showed that the overall standardized mean difference in NSCS between the intervention group compared to control was -0.93[-1.28 -0.58] (p < 0.001). These results indicate that the overall NSCS value of the intervention group was significantly better than the control group. Conclusions: Data from a systematic review and meta-analysis showed that the application of VCO can provide significantly better results in improving the skin integrity of preterm infants.
Introduction
The skin barrier in preterm infants has not fully functioned properly, therefore they have a greater susceptibility to serious infections than those in normal infants. Global data show the neonatal mortality rate reaches 3 million per year, most of which are caused by complications due to preterm birth. In Indonesia, preterm infant occurrence is 15.5 per 100 live births with a death rate per year due to infection reaching 24-34% in 2010 [1, 2]. This high risk of death is due to the difficulty of preterm infants to adapt to life outside the womb due to the immaturity of their organ systems such as skin barrier [2, 3, 4]. Preterm infants need extra care to maintain the integrity of their skin through infection prevention, where the main recommendation is the administration of emollients [5, 6, 7, 8].
The Neonatal Skin Condition Score (NSCS) is one of the objective skin integrity assessment methods by observing the degree of erythema, dry skin condition, and skin damage (such as erosion, excoriation, or other forms of tissue discontinuity). A high score of the assessment result may indicate a change in skin integrity that may predispose the neonates to infection. This score has been developed to objectively assess baseline and post guideline skin conditions, particularly in research-based practice regarding neonatal skincare. The NSCS can describe the overall skin condition in neonates who are hospitalized and can identify those who need intervention by their subscale, resulting in 3 as the best score, and 9 as the worst score.
Coconut oil has now been widely studied and used as moisturizers, especially in developing countries, because the ingredients are easily available and the price is relatively affordable. This oil is distinguished based on the raw materials used and the manufacturing process into coconut oil (copra oil), which comes from dried coconut meat, and virgin coconut oil (VCO) which comes from fresh coconut meat (kernel), processed without the addition of heat or chemicals. It contains medium-chain fatty acids that play an important role in the formation of the skin barrier and lauric acid (monolaurate) that has antimicrobial activity [5, 9, 10]. In addition to antimicrobial activity, monolaurate has also been shown to have anti-inflammatory activity, including the ability to reduce pro-inflammatory cytokines [11, 12, 13]. This oil coat and occlude the barrier when applied to the skin, so that the stratum corneum is hydrated and TEWL can be slowed down. The provision of VCO as an emollient with its antimicrobial activity is expected to allow augmentation or improvement of the barrier structure of the skin [4]. The purpose of this study was to review previous studies to provide a systematic summary of the effectiveness of topical coconut oil in improving the skin integrity of premature infants.
Material and Methods
Data collection
Data collection was carried out online using electronic databases including Medline Pubmed, Scopus, ProQuest, ScienceDirect, SpringerLink, Elsevier Clinical Key, Cochrane library, ClinicalTrials.gov, as well as hand searching from libraries in Indonesia with a period until data analysis was carried out. The study sample size was all clinical trials with randomization regarding the administration of coconut oil in preterm infants’ skin according to the research criteria. The search for information sources is carried out until the data analysis was conducted. The following Medical Subject Headings (MeSH) terms are used to create two subgroups of citations, topical coconut oil for preterm babies and clinical trials.
Data analysis
Prior to data analysis, the collected data were checked based on their characteristics such as research title and year. Inclusion criteria include Research using topical coconut oil for preterm babies, clinical trials, subjects who were born at 20-37 weeks of gestation and had no pre-existing skin infections, and research outcomes in the form of NSCS or other scores assessed against similar clinical criteria. Exclusion criteria studies: written neither in Indonesian nor English, case report, serial case, letter, and literature review.
The systematic review and meta-analysis of weighted mean differences between the treatment and control groups were analyzed using the Cochrane systematic review software (Review Manager (RevMan) [Computer program] Version 5.3. Copenhagen: The Nordic Cochrane Centre).
Result and Discussion
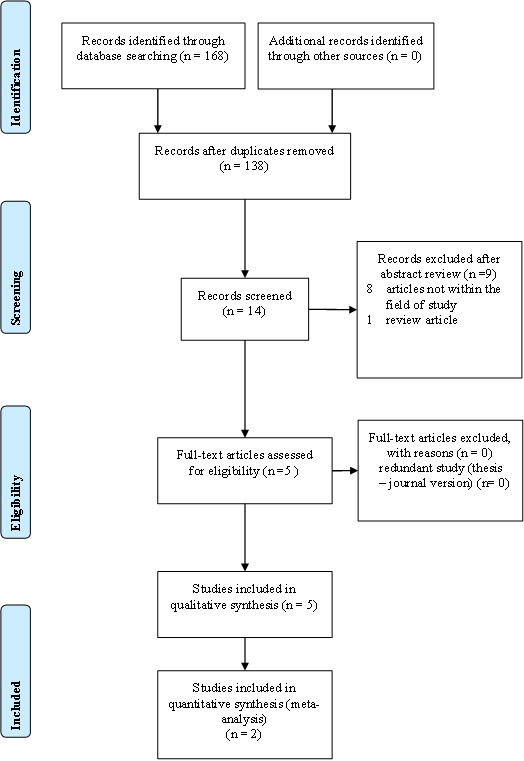
The search for research articles was conducted based on the 2009 Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) flowchart (Figure 1).
Data collection was carried out online using electronic databases including Pubmed-MEDLINE, Scopus, ProQuest, Scopus, Cochrane Library, ClinicalTrials.gov, and Google Scholar, as well as hand searching from libraries in Indonesia with a period until the analysis was carried out. The initial search collected 168 articles. After checking the title and removing duplication, there were 138 articles. A thorough assessment of 138 articles demonstrated that 14 article titles were considered relevant and included in the analysis. The abstracts of these articles were then reviewed, so that 9 articles were excluded, consisting of 8 primary research articles outside the topic of this meta-analysis, and 1 title is a review article. Five articles in the form of complete papers were assessed for feasibility and used in qualitative studies, while two of those five articles were used in quantitative studies to assess the effectiveness of VCO application in improving skin integrity of preterm infants.
Research Characteristics
The majority of the research locations were carried out in India (n=2), Pakistan (n=1), Australia (n=1) and the Philippines (n=1). All studies used a randomized clinical trial design. The total sample of 5 studies was 2,750 people. All studies selected a population of preterm newborns as research subjects, with various gestational ages, including 33 weeks with 12 hours of age, ranges >26 and <37 weeks, 37 weeks, <30 weeks, and 34 weeks with age < 72 hours. Two studies used topical coconut oil in the intervention group compared with the control group, while the other three studies used topical VCO as an emollient given to preterm infants compared to the control group. All studies used a control group that only received routine care for preterm babies in general, without additional treatment. Four out of five studies applied the oil with a frequency of 2x a day, while one study used oil 4x a day. The duration of the treatment was different, where 2 studies gave oil for 28 days, 1 study for 7 days, 1 study for 21 days, and 1 study for 14 days.
Result of Qualitative Data Analysis (Systematic Review)
Strunk, et al. 2017
This study was conducted in Australia on 72 preterm infants with gestational age <30 weeks and 24 hours postpartum. Subjects were divided into two groups, where 36 neonates in the treatment group received topical VCO, while 36 neonates in the control group did not receive the oil. Gestational age ranged from 23.7–29.9 weeks for the treatment group and 23.0–29.9 weeks for the control group. VCO was given twice a day at 5 mL/kg for 21 days by trained nurses, starting within 24 hours after birth. The oil is applied to the entire surface of the skin, except for the face, scalp, and the site of insertion of a catheter or drain, and is given with gentle strokes without massage. The process of giving coconut oil is done within 2-3 minutes. Both groups received routine care for neonates according to the latest guidelines in the NICU, where topical VCO was applied to the treatment group at the same time as routine care to avoid excessive contact with the baby [14].
The main results assessed in this study were the feasibility of using coconut oil in infants who were used as research subjects according to the study protocol, safety or incidence of skin irritation or local infection, and effectiveness in improving the skin condition of preterm infants assessed using NSCS by two independent examiners before the intervention, as well as on days 7, 14, and 21. Secondary outcomes in the form of mortality rates and the incidence of late-onset sepsis (LOS) will also be discussed in this chapter, while other results include weight gain, the incidence of body temperature instability, intraventricular hemorrhage, necrotizing enterocolitis, retinopathy of prematurity, and chronic lung disease will not be discussed further because they are not related to skin integrity.
The median value (IQR) of neonates in the treatment group, which was 1.312 (1.085-1.502) grams, showed better results than the control group, which was 1.296 (1.066- 1.492) grams on day 21. Mortality in the treatment group was 0 (0), while the control group is 4 (14).
Median (IQR) NSCS in the control group showed a decrease from a score of 3 (3–4) on the first day, to 4 (4–4) on day 21, while neonates in the intervention showed a stable median value from birth until the end of the intervention period, 3 (3-3); p = 0.01.
The use of coconut oil twice a day was considered very feasible. Undesirable events due to the use of coconut oil were not found in this study. The incidence of skin irritation showed equal results in both groups, where the treatment group got 9 events (25%), while the control group got 8 events (22.2%); p = 0.779. This study showed that the use of topical VCO as prophylaxis on the skin of preterm infants can result in significantly better skin integrity without any unwanted events.
Konar, et al. 2019
This study was conducted on 2,294 preterm newborns who were divided into two groups randomly using a computer program. Groups A and B consisted of 1146 and 1148 preterm newborns, respectively, with gestational age <37 weeks. The mean gestational age of the study population was 31.9±3.4 weeks, of which 50.4% of the infants were male. Neonates who were included in group A received 5 ml of VCO, four times a day. Coconut oil is applied with gentle massage by the nurse on duty (during hospitalization) and by the mother/family member (after discharge) to all body surfaces other than the face and scalp after they wash their hands thoroughly. Neonates included in group B received treatment in the form of gentle massage by the nurse on duty (during hospitalization) and by the mother/family member (after being discharged) without applying oil to the skin [15].
The results assessed in this study that related to skin integrity included skin condition scores and clinical conditions, which were assessed for the presence or absence of sepsis. Other outcomes such as weight gain, serum vitamin D3 level, and neurologic development were not discussed further because they were not related to skin integrity. Skin condition or integrity was evaluated using NSCS at 7, 14, 21 and 28 days of age. The score is determined based on three main parameters: dry skin, erythema, and damage or impaired skin integrity. The NSCS score is obtained by adding up the three scores.
No significant difference in mean NSCS was found between the two groups at study entry (4.9±1.1 compared with 5.0±1.0, p>0.01). However, during the study period it was found that there was a significantly better NSCS score in Group A compared to Group B on days 7, 14, 21 and 28 (p<0.01). The mean score of NSCS on day 28 of group A was 3.9±0.7, while group B was 4.8±1.0.
Earlier maturation was found in the skin of the neonates in Group A. The neonates in Group A were 0.31 times less likely (95% CI: 0.24–0.39) to have decreased skin maturity. Group A also showed a 0.45 times lower (95% CI: 0.39–0.53) probability of developing hypothermia and 0.62 times lower (95% CI: 0.58–0.67) of developing hypothermia. apnea. All of these observations were statistically significant (p<0.01). The incidence of late-onset sepsis (2.7% compared with 3.2%, p>0.01) and the incidence of rash (1.8% compared with 2.0%, p>0.01) were not significantly different between Group A and Group A. Group B. No significant side effects were found due to the use of coconut oil. This study shows that the use of coconut oil on the skin of neonates can help the process of skin maturity and prevent hypothermia in preterm neonates.
Nangia, et al. 2015
This study was conducted on 74 preterm newborns, by comparing the use of topical coconut oil (n=37) with the control group (n=37) for 7 days. Gestational age in the coconut oil group was 31.89±2.21 weeks and in the control group were 31.00±2.45 weeks. Both groups received standard preterm care. The treatment group was given coconut oil spread on the skin starting from under the neck, twice a day, starting at the age of 12-6 hours, while the control group was not given oil. For each session, the nurse on duty will apply 4 ml of coconut oil without massaging [16].
The outcomes assessed in this study were TEWL, skin swab results, and skin condition. The oil group TEWL was checked just before each oil application session using an evaporimeter instrument (VapoMeter®, Delfin Technologies limited, Kuopio, Finland). TEWL in the control group was checked every 12 hours for the first week after birth at the same time as the time of birth. The level of relative humidity and room temperature of the Neonatal Intensive Care Unit (NICU) (RHN and TN), as well as the micro environmental conditions of the infant (RHB and TB), were also recorded each time the TEWL examination was performed. Skin integrity was evaluated at the end of the first week after birth using SCGS by Lane and Drost, where a score of 0 represented the best skin condition and 9 represented the worst skin condition.
Culture examination of skin swab samples was performed at the end of the first week after birth to evaluate bacterial colonization in the skin. The officers who examined the skin scores, the microbiologist, and the officers who analyzed the data were not aware of the division of the study groups.
The oil group showed significantly lower TEWL values at all measurement points from 12 to 168 hours of age. The mean value of TEWL of the coconut oil group showed a significantly lower result, 15.67±8.67, than the control group, which was 25.64±26.43.
The skin condition showed good results in both groups, with the worst score obtained as much as 3, where the skin score was significantly better in the group that received oil. The highest score of skin conditions in infants after treatment in the oil group was 1 (54.05%), followed by a score of 2 (43.24%), and the least was a score of 3 (2.7%). The highest score in the control group was a score of 2 (70.27%), a score of 3 (18.92%), and a score of 1 (10.81%).
Culture examination of skin swab samples showed sterile results in 81% of infants in the oil group and 43% of infants in the control group. Seven infants in the oil group showed growth of gram-positive coccus bacteria, while in the control group, growth of gram-positive coccus bacteria was found in 16 infants, gram-negative bacilli in 4 infants, and mixed colonization in 1 infant.
Salam, et al. 2015
This study was conducted on 258 preterm babies born at Aga Khan University Hospital (AKUH), Karachi, Pakistan, with a gestational age range of >26 and <37 weeks for 28 days. The subjects were divided into two groups, the intervention group with coconut oil application and the control group. The treatment group was given 5 mL/kg of coconut oil, twice a day in all over the body surface (other than the face, scalp, and the location of the intravenous infusion line) for 2-3 minutes. All neonates in the treatment and control groups underwent the same routine care for premature infants [6].
The study was conducted for 28 days. Neonates in both study groups were monitored once a week after discharge from the hospital until 28 days of age. Mothers of neonates in the intervention group were trained to apply coconut oil twice a day at home until the baby was 28 days old and given a new supply of coconut oil in a sterile container once a week upon arrival for a control examination. Compliance with oil use was evaluated at each control visit by checking the volume of oil required to refill the previously supplied container to the brim.
The main assessment in this study is the incidence of hospital-acquired bloodstream infection (HABSI), which is defined as the presence of positive blood culture for any pathogenic organism. A blood culture is performed whenever the doctor suspects a systemic infection based on clinical signs, including lethargy, poor peripheral perfusion, fever or unstable body temperature, increased oxygen demand, abdominal distension, inability to eat, bradycardia, or apnea. The secondary outcomes evaluated included weight gain and skin condition, which were assessed daily by the nurse after the baby was bathed using a sponge in both study groups. The skin condition of the neonates was assessed based on the criteria used by Salam, et al. where the scores were 0: Skin intact; 1: Reddish skin; 2: Visible peeling skin and appearance of red spots; and 3: if there are bruises and abrasions. Mortality rates were also recorded at 28 days of age.
The incidence of HABSI was found to be greater in the control group than the treatment at the end of the study. A total of 38 neonates were recorded as having HABSI, with the most common etiologies being coagulase-negative Staphylococcus spp and Acinetobacter spp. Four neonates were known to be infected by Klebsiella pneumoniae, 3 neonates each by Pseudomonas spp and Staphylococcus aureus, 2 neonates each by Enterococcus spp and Candida albicans, and 1 neonate by Streptococcus spp. The treatment group showed lower HABSI overall, in which only 22 neonates developed an infection. Three of them were caused by Acinetobacter spp, 2 by Klebsiella pneumoniae, while the other 4 were caused by coagulase-negative Staphylococcus spp, Enterococcus spp, Candida albicans, and Staphylococcus aureus, respectively.
The use of coconut oil was proven to significantly improve skin integrity (p<0.0001), where 31% or 40 of 128 neonates in the control group showed impaired skin integrity with different degrees of severity; as many as 3 neonates were known to have a score of 3, 20 neonates showed a score of 2, 17 neonates with a score of 1, and 90 others with a score of 0. The treatment group showed fewer skin integrity disorders, namely only in 11% or 15 of 130 neonates, where 2 neonates showed a score of 3, 4 neonates with a score of 2, 9 neonates with a score of 1, and as many as 113 neonates (88.3%) showed a score of 0 or no skin disorders. The length of hospitalization was about 7 days in both groups, where the treatment group was 7.0 days, while the control group was 7.7 days (p=0.416). Undesirable side effects due to the use of coconut oil in the form of skin reactions, phototherapy burns, or other types of infection, were not found in the treatment group.
Bautista, et al. 2013
This study was conducted on 52 preterm infants with gestational age at birth 34 weeks, aged <72 hours to determine the effectiveness of topical VCO administration compared to the control group. The treatment group consisted of 24 infants, while the control group consisted of 28 infants. Infants in the treatment group received topical VCO twice a day for 14 days after being included as study subjects, at a dose of 4 g/kg body weight per session. Patients in the control group received routine skincare according to standards in the NICU, with minimal or no use of topical emollients. Both groups received the same general care [17].
The main outcome assessed was the incidence of nosocomial infections in the form of sepsis, both clinically diagnosed and supported by bacteriological examination results, pneumonia, meningitis, necrotizing enterocolitis, and urinary tract infections. Other secondary outcomes were not discussed further because they were not related to the skin integrity of preterm infants.
All patients underwent routine blood cultures at the start of the study within 48 hours of starting treatment. The results obtained were then compared with the results of blood and cerebrospinal fluid culture examinations performed on patients suspected of having sepsis. If the culture performed on a patient suspected of having sepsis showed the same type of organism as the initial culture, the patient was considered to have a persistent congenital infection and was excluded from analysis for nosocomial infection. Infants who are research subjects will be observed their development until the age of 28 days or until the patient is discharged.
The frequency of incidence of nosocomial sepsis in the control group showed higher results when compared to the intervention group, 12 of 28 (43%) compared to 9 of 24 infants (38%). However, this difference was not statistically significant (P=0.695). The mortality rate showed relatively similar results between the two study groups; where the group that received routine skincare showed a mortality rate of 14% and the topical VCO therapy group showed a mortality rate of 12%, P= 0.851.
Quantitative Data Result (Meta-Analysis)
Meta-Analysis of the Effect of Virgin Coconut Oil on Skin Integrity of Preterm Infants
The NSCS in the VCO group compared with control was presented in table 1. Table 1 showed that the intervention group had a lower NSCS after VCO administration, which was 0 ± 0.1 compared to the control group that did not receive oil, which was 0.67 ± 0.77. The lower NSCS was reported after VCO administration, which was -1 ± 0.96 compared to the control group, which was -0.2 ± 1 [15].
| Study or Subgroup | VCO | Control | ||
|---|---|---|---|---|
| Mean ± SD | (n) | Mean ± SD | (n) | |
| Strunk, et al., 2018 | 0.0±0.10 | 36 | 0.7±0.77 | 36 |
| Konar, et al., 2019 | -1.0±0.96 | 1146 | -0.2±1.00 | 1148 |
Table 1: The NSCS in the VCO group compared to control.
The results of the meta-analysis of the effectiveness of topical VCO on NSCS of preterm infants are shown in the following table:
| Study or Subgroup | Experimental (Coconut oil) | Control | Std Mean Difference IV, Random, 95% CI | Std Mean Difference IV, Random, 95% CI | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Total | Mean | SD | Total | Weight | |||
| Strunck, et al. 2018 | 0 | 0.1 | 36 | 0.67 | 0.77 | 36 | 29.00% | -1.21 I-1.71, -0.70] | |
| Konar, et al. 2019 | -1 | 0.96 | 1146 | 0.2 | 1 | 1148 | 71.00% | -0.82 [-0.90, -0.73] | |
| Total (95% CI) | 1182 | 1184 | 100.00% | -0.93 [-1.28, -0.58] |
Table 2: The meta-analysis of the effectiveness of topical VCO on NSCS of preterm infants.
Heterogeneity: Tau2 = 0.04; Chi2 = 2.25, df=1 (p=0.13); I2 = 55% Test for overall effect: Z = 5.23 (p < 0.00001) Table 2: The meta-analysis of the effectiveness of topical VCO on NSCS of preterm infants.
The mean difference between the treatment and control group in Strunk, et al.’s study was -1.21 (95% CI = -1.71 to -0.70) [14]. The mean difference between the treatment and control groups in Konar, et al’s study was -0.82 (95% CI = -0.90 to -0.73) [15]. Meta-analysis showed a heterogeneity test with I2=55% (p=0.13). The meta-analysis was carried out using a random-effect model. The results of the meta- analysis as a whole showed the overall effect of giving topical VCO to preterm infants in the treatment group compared to the control group on decreasing NSCS scores with a significant difference (p<0.001), with overall standardized mean difference -0,93 (95% CI= -1,28 s/d -0,58). These results indicate that the overall NSCS of the intervention group was significantly lower than the control group.
Risk of Bias from the Included Studies
The research articles included in the meta-analysis were 2 studies; Konar, et al. 2019; Strunk, et al. 2017 reported data with outcomes in the form of pre and post NSCS treatment using topical VCO. The risk of bias from studies included in the analysis, both qualitative and quantitative, was assessed using The Cochrane Collecting data - form for RCTs only and The Cochrane Collaboration’s tool for assessing the risk of bias in randomized trials, including randomization, allocation concealment, blinding of study subjects, blinding outcomes, incomplete outcome data, selection of reported outcomes, and other biases. The risk assessment of bias from each of these aspects is then converted according to Agency for Healthcare Research and Quality (AHRQ) standards. The risk assessment for bias is shown in Table 3. All studies have a high risk of bias for blinding personnel from the study because the clinical care team knows the division of research groups so that the type of intervention carried out does not allow blinding. The other reason was the inability to develop an appropriate placebo formulation to compare its effects with coconut oil and to mask the natural characteristic of this oil that made it impossible to blind the doctors and nurses at the time of administering emollients. That’s what makes these studies categorized as the medium quality of evidence. Thus, although the participants and personnel cannot be blinded in this study, this research can still be considered to have good quality.
| Random Sequence Generation | Allocation Concealment | Selective Reporting | Other Bias | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Standard AHRQ | |
|---|---|---|---|---|---|---|---|---|
| Strunk, et al. 2017 | Fair | |||||||
| Konar, et al. 2019 | Fair | |||||||
| Nangia, et al. 2015 | Fair | |||||||
| Salam, et al. 2015 | Fair |
Table 3: Risk of bias in studies used for systematic reviews and meta-analyses. Circle symbol of λ with a positive sign indicatin
Discussion
This study is a meta-analytic observational study, a systematic review and a meta-analysis on the effectiveness of VCO on improving the skin integrity of preterm infants with skin condition score parameters obtained from visual observations, NSCS. All studies showed better scores in the treatment group at the end of the study.
The first dan second previous study [14, 15], both used VCO in the intervention group and assessed skin condition at the beginning and end of the study using NSCS. Neonatal skin condition score in the study of Strunk showed the same median value in the treatment and control groups at the beginning of the study, but at the end of the observation, preterm infants in the control group experienced worsening of skin condition scores, from the median value (IQR) 3 (3-4) to 4 (4-4) at the end of the study. The group that received topical VCO had a stable median value (IQR) at the beginning and end of the study, which was 3 (3-3). The median value (IQR) was obtained from the correspondence between the researcher and the author of the article. The estimated mean ± SD of the research data is calculated using the formula x = (a+2m+b)/4; using the median (m), the range of the lowest (a) and the highest (b) [14].
The mean value of NSCS in Konar’s study in the two groups both decreased, but the results showed that the group that received VCO experienced better skin integrity improvement, where there was a decrease in the mean NSCS from 4.9±1.1 to 3.9 ±0.7, while in the control group 5±1 became 4.8±1 at the end of the treatment [14].
Some of the studies mentioned above also had other outcomes assessed related to skin integrity. Nangia, et al. 2015, investigated the effect of topical administration of coconut oil on TEWL values [15]. The results showed that the intervention group had significantly lower TEWL values at all measurement points from 12 to 168 hours of age. The mean value of TEWL of the coconut oil group showed a significantly lower result, namely 15.67 ± 8.67 than the control group, which was 25.64 ± 26.43. This is certainly related to the relationship between the TEWL value and the skin barrier function. As it is known that TEWL is the amount of water that evaporates passively through the skin to the external environment caused by the pressure of water vapor on both sides of the skin barrier. This TEWL value is often used as a marker of skin barrier function. A low value is considered an indicator of the presence of an intact or restored skin barrier. This is following the results of the study where the group of preterm infants who received coconut oil had better skin integrity conditions than the control group, in line with the TEWL value which was also lower in the intervention group compared to the control.
The incidence of nosocomial infections was also investigated by looking at the results of skin swabs, the presence or absence of sepsis, the incidence of HABSI, and the number of incidences of nosocomial infections. Another study applied swab the skin of preterm infants on the seventh day after treatment. Culture examination of skin swab samples showed sterile results in 81% of infants in the coconut oil group and 43% of infants in the control group. Seven infants in the oil group showed growth of gram- positive coccus bacteria, while in the control group, growth of gram-positive coccus bacteria was found in 16 infants, gram-negative bacilli in 4 infants, and mixed colonization in 1 infant. This statistically significant difference shows the effect of the protective properties of coconut oil on the occurrence of bacterial colonization on the skin with its antimicrobial activity, which comes mainly from monolaurin. The monoglyceride form of lauric acid works by disrupting microbial membranes and has been shown to have activity against various bacteria, fungi, and viruses that have a lipid envelope [15].
The other study assessed the incidence of HABSI at the end of the study, where it was found that the incidence was higher in the control group than in the intervention group. A total of 38 preterm infants were recorded as having HABSI, with the most common etiology being coagulase-negative Staphylococcus spp. and Acinetobacter spp. Four neonates were known to be infected by Klebsiella pneumoniae, 3 neonates each by Pseudomonas spp. and Staphylococcus aureus, 2 neonates each by Enterococcus spp. and Candida albicans, and 1 neonate by Streptococcus spp. The treatment group showed lower HABSI overall, in which only 22 neonates developed an infection. Three of them were caused by Acinetobacter spp, 2 by Klebsiella pneumoniae, while the other 4 were caused by coagulase-negative Staphylococcus spp., Enterococcus spp., Candida albicans, and Staphylococcus aureus, respectively. Some of these pathogenic bacteria which are normal flora on the skin include Coagulase-negative Staphylococcus spp., Pseudomonas spp., Streptococcus spp., and Candida albicans. The presence of these bacteria in the bloodstream or an increase in the number on the surface of the skin is an indication of infection [6].
Strunk, et al. 2017, reported a mortality rate of 0 (0) in the treatment group, while the control group was 4 (14). Late-onset sepsis during the intervention period in the intervention group was only found in 1 infant (2.8%) with the causative organisms S. marcescens, E. faecalis, S. warneri; while the control group had 4 infants caused by E. cloacae, E. faecalis, S. capitis, S. epidermidis, and S. aureus [14]. Some of these pathogens which are normal flora of the skin include S. wareri, S. epidermidis, and S. aureus. One of the factors that can cause this process is the presence of poor skin barrier integrity in the skin of preterm babies. Neonatal skin generally begins to be colonized by various types of microorganisms, including potentially pathogenic ones, within a few days after birth. The presence of poor skin integrity is a problem that is often encountered in preterm infants and can be associated with an increased risk of nosocomial infections because it can be a port of entry for various pathogens. The lower incidence of HABSI in the treatment group proves the antimicrobial activity of coconut oil, which can also improve the skin barrier structure of preterm babies so that they can carry out the skin barrier function properly.
Salam study showed that the use of coconut oil on the skin of preterm infants can help the process of skin maturity in addition to preventing hypothermia. These findings can be based on the effect of using emollients in providing essential fatty acid supplementation that can help the skin maturation process, and prevent the process of invisible water loss by reducing latent heat so that it will reduce the incidence of hypothermia. Thereby reducing the incidence of late-onset neonatal sepsis, indicated by a decrease in the incidence of late-onset sepsis in this study after the use of coconut oil in the treatment group, although the results were not statistically significant [6].
Another study related to the effectiveness of topical coconut oil on the skin integrity of preterm infants was also conducted with a different outcome, namely the incidence of nosocomial infections in the form of sepsis, both clinically diagnosed and supported by bacteriological examination results [17]. Nosocomial infection was defined as the incidence of localized or systemic infection with onset after birth, excluding the type of infection known to have been transmitted through the placenta or infection that started within 24-72 hours after birth. This means that in most cases of bacterial infection, symptoms and signs will begin to appear within 48 hours or so after the baby is started. Clinically diagnosed sepsis (clinical sepsis) is defined as the appearance of some signs and symptoms including instability of body temperature (hypothermia or hyperthermia), signs of organ hypoperfusion such as hypotension, slow capillary refill time, reduced urine volume, or the presence of significant metabolic acidosis, apnea and/or bradycardia, leukocytosis or leukopenia, or thrombocytopenia, with negative blood culture results. Sepsis supported by bacteriological examination results was defined as the appearance of various signs and symptoms above plus the discovery of a specific pathogen on one or more blood culture examinations, without finding other possible causes of infection. This study reported that the incidence of nosocomial sepsis in the control group who only received routine skincare, showed higher results when compared to the group receiving topical VCO, namely 12 of 28 (43%) compared to 9 of 24 infants (38%). However, this difference was not statistically significant, P=0.695. The mortality rate showed relatively similar results between the two study groups; where the group that received routine skincare showed a mortality rate of 14% and the topical VCO therapy group showed a mortality rate of 12%, with a P-value = 0.851.61 The occurrence of nosocomial infections in preterm infants was still closely related to the fragile factor of the skin barrier which was not fully developed so that It has the potential to be one of the entrances for various pathogenic bacteria. It is well known that the application of coconut oil can accelerate the maturation of the skin barrier and improve its function to reduce the risk of infection. The results that were not significantly different between the treatment and control groups in this study could be influenced by other factors, such as the sample size being too small compared to other studies.
All of the studies mentioned above showed an improvement in skin integrity in preterm infants which can be seen from the better score of the skin condition in the treatment group compared to the control group, the presence of a significantly decreased TEWL in the treatment group, better results in skin swab culture, the number of lower incidence of HABSI, and lower incidence of nosocomial infections in the group receiving coconut oil. However, this research has some limitations, such as there is no suitable placebo formulation that can be developed to compare its effect on topical coconut oil, all the participants who apply coconut oil cannot experience the blinding process related to the nature and aroma of coconut oil, there are differences in the frequency and duration of studies, also there are several studies that have not used NSCS in clinically assessing the skin integrity of preterm infants.
Conclusion
The results of a systematic review and meta-analysis showed that the application of virgin coconut oil can provide significantly better results in improving the skin integrity of preterm infants.
References
-
Darmstadt GL, Ahmed S, Ahmed NU, Saha SK (2014) Mechanism for prevention of infection in preterm neonates by topical emollients: A randomized, controlled clinical trial. Pediatr Infect Dis J 33: 1124-1127.
-
Sulistiarini D, Berliana SM (2016) Faktor-faktor yang memengaruhi kelahiran prematur di Indonesia: Analisis data Riskesdas 2013. E-Journal WIDYA Kesehatan dan Lingkungan 1(2): 109-115.
-
Darmstadt GL, Dinulus JG (2000) Neonatal skin care. Ped Clin North Am 47: 757-782.
-
Rowell VM, Dillague KM, Tjundawan BS (2008) Novel antibacterial and emollient effects of coconut and virgin olive oils in adult atopic dermatitis. Dermatitis 19(6): 308-315.
-
Salam RA, Darmstadt GL, Bhutta ZA (2015) Effect of emollient therapy on clinical outcomes in preterm neonates in Pakistan: a randomised controlled trial. Arch Dis Child Fetal Neonatal 100(3): F2105.
-
Jurica SA, Čolić A, Gverić-Ahmetašević S, Lončarević D, Filipović-Grčić B, et al. (2016) Skin of the very premature newborn - Physiology and care. Paediatria Croatica 60(1): 21–26.
-
Kusari A, Han AM, Virgen CA, Matiz, C, Rasmussen M, et al. (2019) Evidence-based skin care in preterm infants. Pediatric Dermatology 36(1): 16-23.
-
Elmore LK, Nance G, Singleton S, Lorenz L (2014) Treatment of dermal infections with topical coconut oil, A review of efficacy and safety of Cocos nucifera L. in treating skin infections. J Nat Med 6(5): 1-14.
-
Deen A, Visvanathan R, Wickramarachchi D, Marikkar N, Nammi S, et al. (2021) Chemical composition and health benefits of coconut oil: an overview. Journal of the Science of Food and Agriculture 101(6): 2182-2193.
-
Newell-Fugate AE, Lenz K, Skenandore C, Nowak RA, White BA, et al. (2017) Effects of coconut oil on glycemia, inflammation, and urogenital microbial parameters in female Ossabaw mini-pigs. PLoS One 12(7): e0179542.
-
Kim S, Jang JE, Kim J, Lee YI, Lee DW, et al. (2017) Enhanced barrier functions and anti-inflammatory effect of cultured coconut extract on human skin. Food Chem Toxicol 106(Pt A): 367-375.
-
Varma SR, Sivaprakasam TO, Arumugam I, Dilip N, Raghuraman M, et al. (2018) In vitro anti-inflammatory and skin protective properties of Virgin coconut oil. Journal of Traditional and Complementary Medicine 9(1): 5-14.
-
Wan X, Wang W, Liu J, Tong T (2014) Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 14: 135.
-
Strunk T, Pupala S, Hibbert J, Doherty D, Patole S (2018) Topical Coconut Oil in Very Preterm Infants: An Open- Label Randomised Controlled Trial. Neonatology 113(2): 146-151.
-
Konar CM, Islam K, Roy A, Ghosh T (2019) Effect of Virgin Coconut Oil Application on the Skin of Preterm Newborns: A Randomized Controlled Trial. Journal of Tropical Pediatrics 66(2): 1-7.
-
Nangia S, Paul VK, Deorari AK, Sreenivas V, Agarwal R, et al. (2015) Topical oil application and trans-epidermal water loss in preterm very low birth weight infants—A randomized trial. Journal of Tropical Pediatrics 61: 414- 420.
-
Bautista R, Mantaring J, Anna OL (2012) A Randomized, Controlled Trial of Topical Application of Virgin Coconut Oil in the Prevention of Nosocomial Infections in Neonates Born ≤ 34 Weeks Gestational Age. Acta Med Philipp 46(4): 18-23.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling