The Use of Dalmatian Tansy - Pyretrin - D and Mandelic Acid in the Care Supporting the Treatment of Rosacea Caused by Demodecosis
Demodecosis is a disease caused by the toxic effects of demodicosis metabolites which contaminate the environment of the sebaceous glands. Sensitive skin is probably most often caused by the development of demodecosis, in the course of which parasites from Demodex folliculorum and Demodex brevis families residing inside the sebaceous glands cause the accumulation of toxic compounds from faeces and dead parasites. This phenomenon increases with age and is associated with slower self-cleaning of the epidermis, leading to secondary infections and the development of rosacea. The proposed cleansing by exfoliation, based on the phenomenon of crystallization of mandelic acid peeling, enables the cleansing of sebaceous glands and preparation of the skin for the application of biocidal products (Dalmatian tansy extract). The paper presents a comprehensive in-office and home procedure as well as the advantages of cooperation between a dermatologist and a cosmetologist in the treatment of rosacea. The aim of the study was to present the results of care with Pyretrin-D products during the dermatological treatment of rosacea and demodecosis.
Joanna Igielska-Kalwat1,2* and Ewa Kilian-Pięta2
Introduction
The treatment procedure in demodicosis requires care that increases the effectiveness and allows to maintain effective operation in the period of remission. The technology of cosmetics and the care procedure using Dalmatian tansy and mandelic acid is based not only on the active effect of pyrethrins, but also on the pH value which affects the chemical tolerance of cosmetics or drugs and the microbiological efficiency of the hydrolipid barrier. Both can cause dysbiosis after treatment is completed, manifested by recurrence of lesions in the form of bacterial complications. Introducing lowered pH care seems to be a solution to reduce this risk.
The etiopathogenesis of demodecosis is complex and not fully confirmed. Based on our own observations, it was found that the inflammatory changes that accompany demodecosis can be compared to the mechanism of atopic dermatitis (AD) caused by contact with house dust mite faeces [1]. Erythema, skin sensitivity to factors such as temperature changes, cosmetics intolerance, flaking, dryness, itching, and eczema are typical symptoms of the dysfunction of the epidermal- lipid barrier.
In the case of the facial skin, where the activity of the sebaceous glands (the natural habitat of Demodex mites as opposed to other parts of the body) is naturally increased, the risk of the toxic effects of these mite metabolites increases [2].
This may be favored by environmental conditions in human skin which result from the disturbance of the natural process of exfoliation and renewal of the epidermis, leading to slower self-cleaning of the sebaceous glands from Demodex faeces (guanine and protease). The inflammatory reaction, manifested initially by the skin’s sensitivity to cosmetics and external factors, is probably associated with a high concentration of guanine and proteases [3].
Guanine, present in mite droppings, is a toxic compound and a strong allergen which is probably responsible for immunological reactions. Cysteine and serine stratum corneum proteases have also been observed in mite droppings, such as scabies, Demodex and house dust mites [4].
Their increasing activity and concentration within the sebaceous glands may have a direct impact on the coherence of the epidermal-lipid barrier. The association with increased Before After activity of stratum corneum proteases and decreased activity of inhibitors such as cystatin is the result of increased epidermal pH (towards alkalization) and TEWL index. It was observed in patients with AD who also had a decrease in the concentration of ceramics and an increased concentration of free fatty acids and sterols in lipids [5].
Case Report
At the Dermatology Center, research was conducted on a group of 50 patients diagnosed with Demodex infestation; they were treated dermatologically. Despite the standard treatment, they experienced relapses. A closer look at care with the use of cosmetics was therefore needed at the beginning of the present research. The photos (Figures 1,2) show the effect of in-office and home care procedures proposed at the Symbiosis Dermatology Center in patients who came in after several years of rosacea treatment with tetracyclines and metronidazole, with complications excluding oral treatment. Figure 1 shows a patient with dominant hypertrophic changes (phymatous rosaceae).

Figure 2 shows a proband with papular eruptions, an advanced condition of rosacea caused by secondary bacterial infections - the most common reason for visiting a dermatologist. It has been observed that this form requires not only elimination of parasites and exfoliation, but also antibacterial treatment. The combination of hygiene according to the proposed procedure, exfoliation using the in-office method and treatment with antibiotic therapy or metronidazole, allows not only the disappearance of symptoms, but also maintaining the effects after the end of antibacterial therapy.

In the “before” photos of both probands, we can observe the skin before new care procedures, after long-term treatment with tetracyclines and metronidazole and the use of micellar fluid without rinsing it with water. Symptoms resolved while taking medication and relapsed after the end of therapy. Demodecosis was diagnosed, and in-office and home care procedures were introduced. In the “after” photos we can see the effects: healthy skin, disappearance of symptoms and of the Demodex infection. For home care, products from the Pyretrin-D series produced in the Symbiosis Laboratory were used. They are intended to effectively eliminate problems related to a Demodex infection. They are recommended for sensitive skin and for people struggling with erythema and rosacea. Incidentally, the use of antimicrobial active substances has become part of the desired trends regarding skin care during the coronavirus pandemic.
The series included the following products: Micellar foam with Dalmatian tansy intended for washing and cleansing the face, eyes and eyelashes. A special light foam formula is designed to be applied to the skin in combination with running water. It is recommended as a washing method during antibiotic therapy or treatment with antiparasitic preparations and exfoliating products. Then the probands applied a face tonic with mandelic acid, dalmatian tansy, tea tree oil and geranium oil, which aims to restore the proper pH value of the skin. In the following step, the volunteers applied the Pyretrin-D normalizing serum. The last stage of the home care procedure was the application of a normalizing and moisturizing cream, the main ingredients of which are Dalmatian tansy extract and black cumin oil [6].
Conditions for the Use of Cosmetics
The probands applied the cosmetics twice a day, in the morning and in the evening (at similar times) at the site of the onset of dermatosis (face). The method and sequence of application was presented by the researcher. When using cosmetic formulations it was not allowed use other care products on the tested area. The tested preparations had to be used regularly. Use of the products should be discontinued immediately in the event of any irritation or allergy symptoms. Unexpected side effects had to be reported to the person conducting the trial. The research was conducted following the approval of the Bioethics Committee, resolution number 640/20 [7].
The in-office treatment was the first step in the preparation of the experiment. Home care, on the other hand, was the second stage aimed at eliminating the skin problems faced by the patients. The participants of the study underwent the Pyretrin-D treatment at the Symbiosis Dermatology Center. It is a procedure in the field of therapeutic cosmetology supporting the treatment of demodecosis (infection with Demodex), developed by specialists from Centrum Dermatologii Symbiosis Sp. z o.o.
It consists in cleansing the skin by exfoliation with a specially developed chemical peeling with extracts of tansy, mandelic acid, tea tree oil and geranium oil. Before that, the skin is cleaned via ultrasound cavitation. The procedure of the treatment is carried out in such a way that it is possible to combine the in-office treatment with dermatological and ophthalmic treatment (ocular Demodex infection) without irritation (Figure 3).

| No. | Action | Backtocomfort® product |
|---|---|---|
| 1 | Make-up removal and washing with foam and water, cavitation | Micellar foam Pyretin-D |
| 2 | Toning and cleansing the skin | Micellar tonic Pyretrin-D |
| 3 | Serum application | Pyretrin-D Serum |
| 4 | Application of a moisturizing and normalizing product | Professional Mask and Pyretrin-D Cream |
| 5 | Application of a biocidal drug according to medical recommendations | Solantra cream (iwermektyna) |
Table 1: Activities in the in-office procedure.
This procedure depends on the condition of the skin which determines the intensity of one’s initial use of the exfoliating product. The natural adaptation of the skin to an acidic environment is individual and may initially manifest as redness burning of the skin. The product is then offered for the first 2 weeks of treatment only in the evening; after that it should be applied twice a day. The effect of complete adaptation and tolerance of successively applied products results in a significant clinical improvement.
The main purpose of the treatment is to empty the skin pores by non-invasive cleansing and to chemically damage adult mites. The skin is fresh and not irritated immediately after the treatment, while a slight reddening may appear on the following day. Another goal of the treatment is to cleanse the skin of metabolites and allergens that are toxic to the skin and that result from the aforementioned infection with Demodex which contaminate the area of the sebaceous glands, causing erythema, burning and discomfort. The peeling is a cosmetic product that additionally has a proven antibacterial effect against Cutibacterium acnes and Staphylococcus aureus; it supports dermatological procedures in the treatment of rosacea caused by Demodex infection.
The treatment is also recommended for people with sensitive skin and seborrhea. The procedure was performed on the first day and at various intervals depending on the condition of the skin [6].
Measurement of Skin Biophysical Parameters
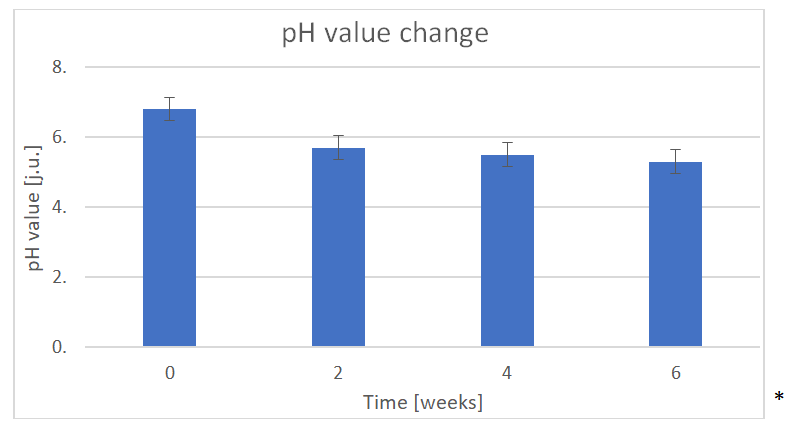
Measurements of biophysical parameters were carried out with the use of a set of probes MPA 580Courage + Khazaka electronic GmbH connected with a computer and equipped with a probe for measuring air temperature and humidity. All measurements were carried out on 50 probands’ T-zones (cheeks, chin and forehead), i.e. the places where cosmetics were applied. The tests were performed before the start of the treatment and home care (test zero), and after each in-office treatment. In this paper, we mainly look at skin pH measurement, which was tested using a pH meter. The results are given on a pH scale that defines the concentration of hydrogen ions. The skin pH value depends on factors related to the epidermis and glandular secretion. The pH of the epidermis is the key index informing about the skin’s susceptibility to infection or keratosis disorders and seborrhea, because the acidic pH level maintains the natural microflora of the skin. On the other hand, alkaline value intensifies the development and penetration of harmful microorganisms, causing infections. The pH value also contributes to the resistance of sensitive skin, the reactivity of which depends on its changes during care activities such as washing, application of serums, creams or tonics. An allergic to cosmetics is often confused with the reactivity to changes in the pH on the surface of the epidermis during the application of individual products, which should be selected after testing the discussed epidermal parameter.
The graph below shows the average change in pH of the probands. It should be remembered that the subjects (n = 50), apart from test zero, were subjected to the treatment and care application with the Pyretrin-D series (Figure 3). The results were averaged. All measurements were made on the cheeks and in the T-zone.
In demodicosis, the skin is contaminated “from the inside” with mite feces, giving symptoms similar to those caused by AD in people allergic to house dust mites. As a consequence, in demodicosis, apart from dermatological and ophthalmic treatment aimed at biocidal activity, it is necessary to develop appropriate hygienic habits in the patient, in order to cleanse the skin of pathogens.
These habits should come down to thorough daily washing of the skin with foam and water, toning and exfoliation. These activities are to, at the same time, a) gradually lower the skin’s pH to acidic due to antibacterial prophylaxis and b) raise the skin’s chemical tolerance threshold and reduce its sensitivity. There has also been widespread overuse of antibiotic therapy and a lack of research into demodicosis in people with symptoms of rosacea. In some patients, the longest treatment with tetracyclines lasted up to 2 years, with the simultaneous prohibition of washing the skin with water. In fact, care should be based on thorough washing with water and mild surfactants, saponins and active compounds supporting the anti-infective effect. In order to improve comfort during the use of the exfoliating procedure in the treatment of demodecosis, it is suggested to use strong antioxidants that protect the skin against chemical stress, as well as components that supplement and activate the production of the NMF. It is also advisable to use soothing base ingredients that actively rebuild the epidermal barrier and are biocompatible with intercellular cement. During the treatment of demodecosis, the skin should be moisturized and not lubricated with barrier emollients that passively inhibit TEWL and may intensify the incubation of Demodex. It is also worth paying attention to the toxicity of the mass decay of Demodex, which in the case of a biocidal action conducted without cleansing may aggravate the symptoms due to the amount of residual allergen in the skin. Therefore, it is very important to cleanse the skin properly, both before starting treatment and during therapy. Initially, cleansing should be performed in the beautician’s office under the supervision of a cosmetologist, using the proposed chemical peeling with mandelic acid in a water-alcoholic solution, which enables exfoliation by acid crystallization on the skin. Taking into account the advantages of the proposed procedures, based on many years of observation and individual search for the best solution for sensitive skin caused by demodecosis, close cooperation between a dermatologist and a cosmetologist seems particularly reasonable. Dermatological treatment of demodecosis, based on a medical consultation and therapeutic instructions for home use, and cooperation with a cosmetologist who performs cleansing treatments with the proposed method, in the office and at home, significantly increase the effectiveness of the therapy [8].
Acquired sensitivity to cosmetics in the course of demodecosis may be caused by the weakening of the lipid-epidermal barrier and an increase in the pH of the epidermis. The interaction of guanine and proteases present in the faeces of this parasite may result in an immune response and activation of protease inhibitors, which in turn inhibit the synthesis of NMF and lipids. Disturbance of the integrity of the lipid-epidermal layer is characterized by increased penetration of irritating or allergenic components. Worsening symptoms of skin “sensitivity” to cosmetics may also be the result of the way it is cleansed.
Based on own research and observations conducted on patients with confirmed Demodex infection at the Symbiosis Dermatology Center, it is assumed that washing with micellar water only had the greatest influence on the severity of the infection and symptoms of demodicosis (in the form of sensitive skin). Such actions resulting from the commonly held belief that water should not be used for cleansing. Studies have shown that the use of washing with only micellar liquid can significantly increase the number of Demodex specimen and, at the same time, disturb the removal of their faeces from already weakened epidermis. The toxic effect of guanine and the disturbance of the natural physiological exfoliation of the skin may lead to cumulative doses (higher concentration) and increase the skin’s sensitivity to substances present in the cosmetic. Symptoms similar to a frequently reported problem, i.e. allergy to cosmetics in demodicosis may also be caused by the increased sensitivity of the TRPV1 receptor (transient receptor potential vanilloid subtype) [9]. A very important factor affecting enzymatic processes participating in cell proliferation is the pH value. In healthy children after birth, its value is close to neutral, i.e. circa pH 6.5. It changes after a few weeks and reaches the value of 5.3 - 5.9 (as in adult skin). The pH value of the epidermis is influenced by endo- and exogenous factors, such as phospholipase A2, NMF components, sweat and sebum components, bacterial metabolites, or organic and inorganic chemical compounds applied to the skin [10, 11, 12].
It was found that the acquired sensitivity to cosmetics in the course of demodecosis is caused, among others, by the weakening of the lipid-epidermal barrier and an increase in the pH value of the epidermis [13].
This receptor is sensitive to many chemical stimuli, including exposure to temperatures greater than 42° C. It also activates after attaching protons (at low pH), which may explain their excitability when using an emulsion with a pH value of 5.5. Skin infected with demodicosis, similarly to healthy skin, becomes more alkaline immediately after washing with soap. Under pathological conditions, the use of soap may lead to a much greater difference in the pH of the lipid barrier, perceived by the receptor as a chemical burn. These symptoms may be aggravated by the increased contact of the cosmetic ingredients with infected skin. In the case of healthy skin, the ingredients do not penetrate that deeply and do not irritate. In the Pyretrin-D series, citric, lactic and almond acids are responsible for regulating the pH value of the skin, the effectiveness of which depends on the pH of the cosmetic. To increase its availability, the active acidity of the cosmetic must be low. After an analysis of Figure 3, it was noted that the pH value of the probands during the study changed on average from an alkaline pH to a pH of 5.5, which is the desired effect.
The mandelic acid has a strong exfoliating effect on the surface of the epidermis, but due to the relatively large particle size, the degree of its penetration is lower compared to glycolic acid. Due to such properties, mandelic acid is a mild exfoliant and does not irritate the skin [14].
Mandelic acid has the smallest molecule among the α-hydroxy acids containing an aromatic group. It exists as two D- and L-enantiomers of mandelic acid. The chemical properties of mandelic acid are directly related to its structure, in which the hydroxyl group is located in the “α” position in relation to the carboxyl group. This structure enables the formation of a hydrogen bond, which increases the melting point and boiling point, and increases the acidic properties in comparison to other carboxylic acids (e.g. azelaic acid). Mandelic acid works against blackheads by dissolving the sebum and clearing the clogged outlets of the hair follicles from the residual sebaceous masses. During cosmetic cleansing, it facilitates the evacuation of the content of the sebaceous gland, thus reducing irritation and the risk of exacerbation of infection. In the treatment of rosacea, it probably minimizes or eliminates secondary bacterial infections to which the facial skin is exposed in the conditions of a weakened lipid barrier. Its keratolytic effect prevents the colonization and spread of Demodex mites on the surface of the skin and in the sebaceous glands. This compound is a valuable cosmetic raw material because it has a broad care spectrum, does not cause irritation and post- inflammatory hyperpigmentation of the skin, but its form of action on the epidermis depends on the base from which it is released [15].
Crystallization is one of the commonly used laboratory
techniques for the purification and separation of solids from solutions. This reaction was used for chemical peeling of the epidermis using a 50% aqueous-alcoholic solution of mandelic acid. The heat of the skin accelerates the evaporation of the solvent, causing the so-called snowing (Figure 4), i.e. the formation of acid crystals on the surface of the epidermis. Cleansing the skin by crystallization is initially based on swelling of keratin in the aquatic environment in the cells of the stratum corneum, denaturation by acid with simultaneous lipid washing and degreasing in the alcoholic environment. The acid dissociation reaction on the surface of the epidermis completes the crystallization process after complete evaporation of the solvent.

The crystallization of mandelic acid during peeling depends on the acid concentration used and the base. A lower concentration of the acid solution extends the crystallization time. The type of solvent used also determines the duration of the treatment and the degree of skin irritation. During the application tests performed at the Symbiosis Dermatology Center, it was shown that the most beneficial solution for skin contaminated with demodicosis is a 50% solution of mandelic acid in 70% ethanol with a pH value of 1.0. The short dissociation time, the maintenance of the hydrolipid barrier and the absence of erythema after washing turned out to be the optimal conditions for cleansing sensitive skin of excess sebum, blackheads, infection caused by demodecosis and secondary contamination from cosmetics. It has been found that cosmetics with mandelic acid effectively affect the exfoliation process only when they are in a concentration between 5-10% and the pH value is 3.0-4.5, and peels need to have the acid content above 40% with a pH value of 1.0- 1.5 [16].
As already mentioned, changes in pH on the epidermis surface depend, inter alia, on external factors such as, for example, the method of washing, the chemical composition of the washing product and the time of its use. Maintaining the physiological pH value while washing the skin depends not only on the pH of the product, but also on the type of surfactants used in the recipe. The effect of the functional groups of surfactants in solutions with a specific pH value is likely to affect the pH value of the epidermis, determining the so-called mildness or aggressiveness of the cleansing action. An example is the popular SLES, i.e. (ethoxylated) sodium lauryl ether sulfate, which, despite the fact that in the solution is acidic (pH value 5.5), when used for washing, does not guarantee the protection of physiological pH. This action can have a particularly negative effect when treating the skin with demodecosis with symptoms of skin over-reactivity to cosmetics, as it increases the risk of secondary infections. [17].
The use of mild cleansing agents and micellar structures in the formula make it possible to wash the skin and remove make-up. People struggling with skin imperfections, such as, for example, erythema, eczema or telangiectasia often use camouflage makeup. Agents responsible for sensory and adhesive properties, often used in covering foundations, may aggravate the degradation of the lipid barrier and contaminate the sebaceous glands. Classic make-up removal with cleaning milk or micellar liquid can deepen skin irritation due to rubbing with the simultaneous application of surfactants without diluting them with water. Such a method may cause a contact reaction that is often confused with an allergic reaction to the fragrance components of the product, and not to too much mechanical and chemical stimulus. Removing make-up in patients with demodecosis by washing the micellar foam with a pH value of 5.5 with water not only thoroughly removed makeup, but also allowed to wash the eye area thoroughly without excessive rubbing and irritation. The additional use of Backtocomfort® micellar fluid with the active ingredients and surfactants listed below (the same as in the foam, creating micellar systems), as well as tonic with almond acid with a pH value of 4.5, not only allowed to clean the skin without irritation, but also to prepare it for the application of other products, i.e. chemical peeling or serum. On the other hand, an extract obtained from Tanacetum cinerariifolum which contains the most pyrethrins (1-1.5%) has been used as biocides. Namely, it has been used as agents to combat parasites [18, 19, 20]. Pyrethrins work by paralyzing the nervous system and the muscular system of parasites. The mechanism of action of pyrethrins is called the knock- down effect. Therefore, the extract is used as a deterrent. In the discussed series, it has a regenerating, deterrent and anti-acne effect. It is also characterized by antiviral, anti- inflammatory, antiparasitic and antibacterial properties [20].
Conclusions
Taking into account the advantages of the proposed in-office and home care procedures, it is reasonable to establish close cooperation between a dermatologist and a cosmetologist regarding sensitive skin caused by demodecosis. The current concept of commonly used antibiotic therapy without individually selected hygiene and exfoliation of the skin seems irrational. In patients who used the Pyretrin-D series, a reduction or complete elimination of inflammation was noticed. Reduction of erythema and closing of the vessels on the nose and cheeks were also found in patients. Improvement in the protective mechanisms of the epidermis was found in all the testees. Thanks to that, the inner layers of the skin are better protected. This prevents infections caused by various microbes. People who struggled with the human Demodex (Demodex folliculorum) infection noticed a significant improvement. By eliminating the excrements of this mite, the existing inflammation improved. All patients noticed that their pores were open on the surface of the skin before the procedure and the application of cosmetics. After participating in the study, they were closed, thanks to which the sebaceous and sweat glands, through which sebum and sweat are secreted, were properly regulated. Patients were fully satisfied with the results. All assessed the effects of the preparations and treatments as effective and in line with the manufacturer’s declaration. The degree of acceptance of the preparations by the volunteers was very high. Further, the impressions of the probands participating in the study regarding the cosmetics used were very good. The concept of cooperation between a dermatologist and a cosmetologist proposed by the author assumes similar effectiveness. The treatment process can be much more comfortable from the sensory point of view, and the cure effect may be more long-lasting if the patient regularly visits the office. The cosmetologist can then identify undesirable side effects, revise the recommendations, and if the disease recurs, see symptoms more quickly and refer the patient to a doctor before symptoms reach an advanced stage. It is also important to educate the patients, who often, in the face of the awareness that they have parasites under their skin, despite visits to a doctor look for treatment methods on their own, deciding on risky unproven methods or preparations from the Internet.
Summing up, the proposed cleansing by exfoliating the skin infected with Demodex, systematic treatments and medical consultations seem to be a comfortable and effective method of treatment. Proper hygiene habits are decisive in maintaining the health of the skin struggling with the problem of demodecosis.
Acknowledgment
This work was financially supported by Dermatology Center Laboratory Symbiosis.
Conflicts of Interest
No conflicts of interest to declare. No identifiable patient information has been used however consent has been obtained from the patient for use in publication.
References
-
Akilov OE, Butov YS, Mumcuoglu KY (2005) Clinico- pathological approach to the classification of human demodicosis. J Dtsch Dermatol Ges 3(8): 607-614.
-
Raszeja-Kotelba B, Pecold K, Pecold-Stępniewska H, Dadej I (2004) Oczny trądzik różowaty – aktualne dane etiopatogenetyczne, kliniczne i terapeutyczne oraz opis trzech przypadków. Post Dermatol Alergol 2: 33-39.
-
Palmer C, Irvine A, Terron-Kwiatkowski A, Zhao Y, Liao H (2006) Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat Genet 38(4): 441-6.
-
Tsui F, Aono H (2012) Role of Transient Receptor Potential Vanilloid 1 in Inflammation and Autoimmune Diseases. Pharmaceutical Basel 5(8): 837-852.
-
Bohdanowicz D, Raszeja-Kotelba B (2001) Demodex w etiopatogenezie niektórych chorób _skóry_. Post Dermatol Alergol 18: 51-53.
-
Cork MJ, Robinson DA, Vasilopoulos Y, Ferquson A, Moustafa M, et al. (2001) New perspectives on epidermal barrier dysfunction in atopic dermatitis: gene – environment interactions. J Allergy Clin Immunol 118(1): 3–21.
-
Igielska – Kalwat J, Kilian – Pięta E (2021) The use of Dalmatian tansy and auxiliary substances as natural substitutes in the treatment of dermatosis. SSRG International Journal of Applied Chemistry 8: 1-9.
-
Corsini E, Galbiati V, Nikitovic D, Tsatsakis AM (2013) Role of oxidative stress in chemical allergens induced skin cells activation. Food Chem Toxicol 61: 74-81.
-
Caterina MJ, Julius D (2001) The vanilloid receptor: A molecular gateway to the pain pathology. Annu Rev Neurosci 24: 487-517.
-
Baranda L, Gonzalez-Amaro R, Torres-alvarez B, Alvarez C, Ramirez V (2002) Corelation between pH and irritant effect of cleansers marketed for dry skin. Int J Dermatol 41: 494-9.
-
Bem B (2004) Rola wyższych kwasów tłuszczowych w fizjologii skóry_._ Pol J Cosmetol 4: 93-101.
-
Bouwstra J, Honeywell-Nguyen PL, Gooris GS, Ponec M (2011) Structure of the skin barier and its modulation by vesicular formulations, Prog Lipid Res 4 caloric restriction, intermittent fasting, exercise and dietary phytonutrients: ‘‘Mitohormesis’’ for health and vitality. Med Hypotheses 66: 832-843.
-
Hachem JP, Crumrine D, Fluhr J, Brown BE, Feingold KR, et al. (2003) pH directly regulates epidermal permeability barrier homeostasis, and stratum corneum integrity/ cohesion. J Invest Dermatol 121(2): 345-53.
-
Taylor Mark B (1999) Summary of Mandelic Acid for the Improvement of Skin Conditions. Cosmetic Dermatology 1: 26-28.
-
Marczyk B, Mucha P, Rotsztejn H (2012) Działanie peelingów chemicznych naj częściej stosowanych w trądziku pospolitym. Dermatologia Kliniczna 14(4): 183-187.
-
Kurtzweil P (2002) Alpha Hydroxy Acids for Skin Care. FDA Consumer 1: 3-4.
-
Kozłowska U (2010) Peelingi chemiczne. Kosmetologia pielęgnacyjna i lekarska 1: 245-253.
-
Corsini E, Galbiati V, Nikitovic D, Tsatsakis AM (2013) Role of oxidative stress in chemical allergens induced skin cells activation. Food Chem Toxicol 61: 74-81.
-
Draelos ZD (2008) New channels for old cosmeceuticals: aquaporin modulation. J Cosmetic Dermatol 7: 83-89.
-
Erbagci Z, Erbagci I, Erkilic S (2003) High incidence of demodicidosis in eyelid basal cell carcinomas. Int J Dermatol 42(7): 567-571.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling