A Humectant-Rich Moisturizer Reduces Xerosis in Diabetic Feet and Susceptibility to an Irritant in Healthy Skin
Xerosis and fissuring of the feet are common in healthy individuals and can also be a subtle sign of diabetes. Removal of dryness and hyperkeratosis with moisturizing creams with keratolytic substances may potentially weaken the skin barrier and make skin more susceptible to external insults. Aim: The objective of this investigation was to study the effect of a humectant-rich cream containing keratolytic and desquamating substances (15% alfa-hydroxy acids, 10% alcohols, and 15% urea) in xerotic feet in patients with diabetes and in healthy skin. Methods: The investigation was an interventional, bilateral, randomized, clinical study with concealed allocation, and evaluator-blind expert evaluation, self-assessment and using non-invasive instruments. In addition, healthy skin was patch- tested with the irritant sodium lauryl sulfate (SLS). The Swedish Ethical Review Authority approved the investigation. Results: At inclusion of the 25 diabetic patients, the median severity of the dryness of the feet was scored to be moderate, and the median severity of the cracks was scored to be mild. Treatment of the feet with the cream significantly reduced the severity of the symptoms, p<<0.05. The patients too noted a significant improvement in their skin condition. Treatment of healthy skin on the volar forearm (n=13) increased skin hydration (capacitance, p<0.05), but did not give any differences in skin barrier function to water (transepidermal water loss, TEWL) or in skin erythema between the treated and untreated arm at days 10 and 20, substantiating absence of irritation from the treatment. However, after exposure to the irritant SLS, the skin was less irritated in the treated arm compared to the untreated, measured as TEWL. Erythema tended to be lower in the treated arm. Conclusion: The humectant-rich cream reduced hyperkeratosis on the feet and increased its barrier resistance to the irritant.
Introduction
Xerosis and fissuring (cracking) of the feet are common in healthy individuals and can also be a subtle sign of diabetes. As many as 80% of patients with diabetes show dryness and fissures, which serve as a portal of entry for bacteria, associated with increased risks of skin infections [1]. The lifetime risk of diabetic patients developing a foot ulcer may be as high as 25%, which eventually may lead to amputation.
Moisturizers rich in humectants are used to overcome xerosis. However, cosmetic moisturizers may lack in efficiency and are not allowed to be marketed in the European Union on hyperkeratotic skin diseases with injured and broken skin, whereas more efficient moisturizers regulated as topical pharmaceuticals and medical devices are allowed in the treatment of hyperkeratosis [2, 3, 4, 5]. Removal of dryness and hyperkeratosis with humectants and keratolytic substances reduces the cohesion between the corneocytes and decreases the number of cell layers in the hyperkeratotic skin. This may weaken the skin barrier [4], keep it intact [5] or strengthen the barrier function [6], depending on the composition of the moisturizer. In healthy skin, similar effects have been noted, where changes in the skin barrier function and increased or decreased in susceptibility to external stressors have been noted [3, 5, 7, 8, 9].
The objective of this investigation was to study the effect of a humectant-rich cream containing keratolytic and desquamating substances (15% alfa-hydroxy acids, 10% low molecular weight alcohols, and 15% urea) on xerosis and cracks the diabetic foot and on skin barrier function and susceptibility in healthy forearm skin.
Material and Methods
The investigation was a post-market interventional, bilateral, randomized, clinical study with concealed allocation, and evaluator-blind expert evaluation, self- assessment and using biophysical instruments. One group of participants consisted of 25 patients with diabetes while the other group consisted of 13 participants with healthy forearms. The Swedish Ethical Review Authority approved both studies, and they were conducted in compliance with the protocol, the General Data Protection Regulation (EU) 2016/679, the Swedish Act concerning Ethical Review of Research involving Humans (2003:460) and the ethical principles of the latest revision of the Declaration of Helsinki as adopted by the World Medical Association.
The test product was a substance based medical device containing aqua, urea, lactic acid, sodium lactate, glycolic acid, tartaric acid, sodium gluconate, panthenol, glycerin, caprylyl glycol, PEG-20 methyl glucose, methyl glucose sesquistearate, butyrospemum parkii butter, octyldodecanol, behenyl alcohol, simmondsia chinensis seed oil, saccharide isomerate, sodium hyaluronate, polyacrylate-1 crosspolymer, methyl methacrylate crosspolymer, retinyl palmitate, pH ca 4, (Footmender All in One Diabetic, Footmender AB, Stockholm, Sweden).
Male and female diabetics > 18 years old, providing written and informed consent were included if they had xerosis or fissures corresponding to at least grade 3 in their feet, Table 1. Pregnancy and other interfering concomitant medication or the use of topical stay-on products were not allowed.
The diabetic patients (n=25) applied the cream once-daily for 2 weeks in one of the feet, and the healthy volunteers applied the product twice daily for 3 weeks on one of the forearms in (n=13). The contralateral part served as the untreated control. Allocation of the test products was conducted using randomly permuted blocks of 4 to reduce variations due to left–right differences.
The expert assessment of skin dryness and fissures on the feet was performed using category scales from 1 to 6 (Table 1) [5]. The self-evaluation of dryness was reported on a visual analogue scale, VAS, (days 0, 7 and 14) where the left end on the line corresponded to extreme dryness and the right end to normal skin. The patients also graded their satisfaction on a 5-graded scale, where 1: ”very dissatisfied”, 2: “somewhat dissatisfied”, 3: ”no opinion”, 4: ”fairly satisfied” and 5: “very satisfied”.
| Rating | Severity | Description Xerosis | Description fissures |
|---|---|---|---|
| 0 | No dryness, soft skin | No fissures, soft skin no dryness | |
| 1 | Mild | Few minute flakes, dusty appearance | Xerosis (≥1 according to above) and hardened skin |
| 2 | Many undifferentiated skin flakes, generalized dusty appearance | Fissuring between scales, shallow fissures, no redness | |
| 3 | Some polygonal scales, defined scaling with flat borders | In-between 2 and 4 | |
| 4 | Moderate | Moderate number of polygonal scales, well-defined heavy scaling with raised borders, | Moderate deep fissuring between scales, potential redness |
| 5 | Large number of polygonal scales, and hardened skin | Severe deep fissuring, potential redness | |
| 6 | Severe | Score 5 and fissuring between scales | Deep erythematous fissuring, several fissures |
Table 1: Grading of the degree of severity of xerosis and fissuring [5].
Bioengineering techniques were used to monitor the effects on the healthy forearms by the treatment. The arms were cleansed in the morning before measurements.
Skin hydration was analysed by measurement of skin capacitance with a Corneometer® CM 825 (Courage+Khazaka electronic GmbH, Germany). The mean value from 5 readings (arbitrary units, AU) was used in the calculations. Skin colour (erythema) was measured using DermaLab® Combo (Cortex Technology, Denmark). The mean value from 4 readings was used in the calculations. Skin transepidermal water loss (TEWL) was measured with an AquaFlux AF200 (Biox Systems Ltd, UK). After application of the probe onto the skin, TEWL was recorded until the standard deviation of the values was 0.075 g/(sq.m h) where after the measurements stops (<70 s). The mean value from 3 measurements were used.
In addition, skin sensitivity was evaluated after treatment for 3 weeks by challenging the skin with an aqueous solution of 1% sodium lauryl sulfate (SLS). Exposure of the skin to SLS was done using patch test with 50 µl on one layer of filter paper in aluminium Finn chambers, Ø 12 mm. The subjects removed the SLS patches after 24 h, rinsed the skin with water and visited the clinic the day after for evaluation of the irritation. The reaction was assessed with the instruments and visually on a scale ranging from 0 to 4 according to the European Society of Contact Dermatitis (ESCD) guideline on clinical scoring of acute SLS irritant reactions [10].
GraphPad Prism version 6.01 for Windows was used for calculations and graphs (GraphPad Software, USA, www. graphpad.com). The Wilcoxon matched-pairs signed-rank test was used on paired data to test for differences. P < 0.05 was considered as significant.
Results
All included diabetics (13 men, 12 women) fulfilled the study with full set of data, and all included healthy volunteers (n=13) fulfilled the study. The mean daily dose on the foot was 1.7 g ± 0.56 g (n=25), and on the forearm 0.62 g ± 0.56 g (n=12). The median age of the 25 diabetic patients (24 with type 2 diabetes,1 type 1) was 74 years, range 52-87 years, mean 73 years ± 8 years.
The only reported adverse reaction was a temporary burning sensation in the feet in one of the 25 diabetics upon application, whereas no adverse reaction was noted in the forearm.
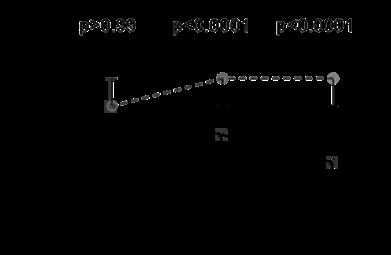
At inclusion, the median severity of the dryness of the feet was scored to be moderate, and the median severity of the cracks was scored to be mild. There were no differences between the feet at inclusion, Figure 1. Treatment of the feet with the cream for one and two weeks significantly reduced the severity of dryness and cracks in the treated skin, p<<0.05, Figure 1. After 2 weeks, all patients scored 2 or less severe symptoms of dryness and less than score 3 on cracks, Figure 1.
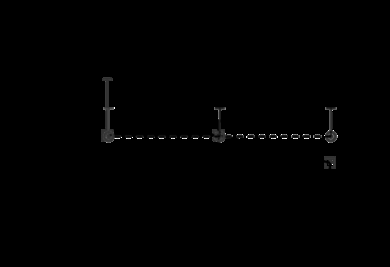
The patients graded the dryness on the feet to 0.4-0.5 on the VAS at inclusion, Figure 2. After treatment for 7 days, the patients noted a significant improvement in their skin condition to median 0.70, which improved further during the next week to median 0.78, Figure 2.
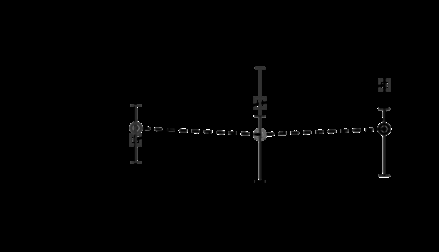
Figure 2: Self-assessment of the severity of dryness and fissures in the feet at inclusion, at days 7 and 14, as judged by the patient on a visual analogue scale (VAS), where 0 corresponds to “extreme dryness/cracks, worse than ever” and 1 corresponds to “no issues, excellent foot”, n=25. The continuous line (squares) corresponds to treated skin and the dotted line (circles) corresponds to untreated skin. Median value and interquartile range_._ The patients rated the change in skin dryness symptoms to median 5 (mean 4.5) on the 5-grade scale, which was statistically different to the hypothetical value “no change” (= grade 3, p<0.0001). The patients rated their satisfaction to “fairly satisfied” (grade 4) to “very satisfied” (grade 5), with median 5 (mean 4.6, p<0.0001). Patients also noted that the skin became softer, elastic and less yellow/brown.
Treatment of healthy skin increased skin hydration (capacitance, p<0.05), but no differences in skin barrier
function to water (TEWL) or in skin erythema were detected between the treated and untreated control at days 10 and 20, substantiating absence of irritation from the treatment (data not shown). However, after exposure to the irritant SLS, the skin was less irritated in the treated arm compared to the untreated, measured as TEWL, Figure 3. The measurement of colour did not reach statistical significance between the arms, and neither did the visual grading of colour detect differences between the arms, although erythema tended to be lower in the treated arm Figure 3.
Discussion
The degree of dryness and cracks decreased significantly in the diabetic feet by the humectant-rich formulation. Both the expert and the patients judged the skin to improve significantly. All patients were also satisfied by the treatment. The magnitude of the improvements was clinically relevant and in agreement with the improvements noted in a previous clinical study on essentially the same combination humectants and keratolytics in dry feet of other origins [5]. In the previous study, the hyperkeratotic stratum corneum layer also was detected to become thinner by the treatment, but no weakening in the skin barrier function was detected [5].
In the present study, the degree of improvement in dryness scores after 14 days of treatment appeared to be greater than that reported in previous studies on hyperkeratotic feet in patients with diabetes using other moisturizers [1, 11]. This may well be explained by the higher levels of urea and alfa- hydroxy acids in the present product compared to the other moisturizers (15% urea in the present cream vs 10% and 5%
in the other two, and 15% alfa-hydroxy acids in the present vs 4% and 1% in the other two). One potential limitation of the present study was its short period of treatment assessment. However, given the type of product (a moisturizer), no reduction in product efficacy related to duration of use is likely. However, this is true only if the cream does not worsen the skin condition by causing irritation or contact allergy. Moisturizers may contain allergens and irritants, such as essential oils or perfumes, which usually are contraindicated for the diabetic foot. In addition, some formulations may weaken healthy skin [7, 12, 13] and increase its susceptibility to external stressors, such as nickel and surfactants [3, 8, 9, 14].
The findings in the present study that no signs of irritation or weakening of the permeability barrier function were detected, whereas instead the susceptibility to the surfactant SLS was decreased, are therefore of clinical benefit related to the safe use of the cream in the diabetic foot. The barrier-protective effect is believed to be mainly due to the high content of urea [6, 15] in combination with the other functional ingredients.
It can thus be concluded that the humectant-rich moisturizing cream reduced hyperkeratosis on the feet in diabetic patients and gave protection against the external irritant in healthy skin.
Conflicts of Interest
Marie Lodén and Sophie Michelson acted as clinical trial consultants and were paid consultancy fees. Gunnar Wahlund was employed by the small enterprise manufacturer, who also sponsored the study.
Funding
Footmender AB, Sweden, sponsored the study.
References
-
Pham HT, Exelbert L, Segal-Owens AC, Veves A (2002) A prospective, randomized, controlled double-blind study of a moisturizer for xerosis of the feet in patients with diabetes. Ostomy/wound management 48(5): 30-36.
-
Lodén M, Wahlund G, Surber C (2020) Crossing the borders. Access to the different regulatory categories of the European skin care products. Household and Personal Care Today 15: 67-69.
-
Loden M (2012) Effect of moisturizers on epidermal barrier function. Clin Dermatol 30(3): 286-296.
-
Gånemo A, Virtanen M, Vahlquist A (1999) Improved topical treatment of lamellar ichthyosis: a double blind study of four different cream formulations. Br J Dermatol 141(6): 1027-1032.
-
Loden M, von Scheele J, Michelson S (2013) The influence of a humectant-rich mixture on normalz skin barrier function and on once- and twice-daily treatment of foot xerosis. A prospective, randomized, evaluator-blind, bilateral and untreated-control study. Skin Res Technol 19(4): 438-445.
-
Grice K, Sattar H, Baker H (1973) Urea and retinoic acid in ichthyosis and their effect on transepidermal water loss and water holding capacity of stratum corneum. Acta Derm Venereol (Stockh) 53(2): 114-118.
-
Buraczewska I, Berne B, Lindberg M, Törmä H, Lodén M (2007) Changes in skin barrier function following long-term treatment with moisturizers, a randomized controlled trial. Br J Dermatol 156(3): 492-498.
-
Zachariae C, Held E, Johansen JD, Menné T, Agner T (2003) Effect of a moisturizer on skin susceptibility to NiCl2. Acta dermato-venereologica 83(2): 93-97.
-
Lodén M (2016) Treatments Improving Skin Barrier Function. Current problems in dermatology 49: 112-122.
-
Tupker RA, Willis C, Berardesca E, Lee CH, Fartasch M, et al. (1997) Guidelines on sodium lauryl sulfate (SLS) exposure tests. A report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermatitis 37(2): 53-69.
-
Garrigue E, Martini J, Cousty-Pech F, Rouquier A, Degouy A (2011) Evaluation of the moisturizer Pedimed((R)) in the foot care of diabetic patients. Diabetes & metabolism 37(4): 330-335.
-
Danby SG, AlEnezi T, Sultan A, Lavender T, Chittock J, et al. (2013) Effect of olive and sunflower seed oil on the adult skin barrier: implications for neonatal skin care. Pediatric dermatology 30(1): 42-50.
-
Danby SG, Al-Enezi T, Sultan A, Chittock J, Kennedy K, et al. (2011) The effect of aqueous cream BP on the skin barrier in volunteers with a previous history of atopic dermatitis. Br J Dermatol 165(2): 329-334.
-
Held E (2001) So moisturizers may cause trouble! International journal of dermatology 40: 12-13.
-
Piquero-Casals J, Morgado-Carrasco D, Granger C, Trullàs C, Jesús-Silva A, et al. (2021) Urea in Dermatology: A Review of its Emollient, Moisturizing, Keratolytic, Skin Barrier Enhancing and Antimicrobial Properties. Dermatol Ther (Heidelb) 11(6): 1905-1915.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling