Fatal Hepatitis Associated with Nivolumab and Ipilimumab Combination Therapy in the Patient with Malignant Melanoma
Immune checkpoint inhibitors are a common treatment for various malignancies, but these therapies are associated with several, immune-related adverse events. We report herein a case of fatal hepatitis caused by nivolumab and ipilimumab combination therapy in the patient of malignant melanoma. Physicians should be aware of the possibility of potentially fatal liver injury resulting from immune checkpoint inhibitors treatment and initiate countermeasures as soon as signs of liver injury become apparent.
Introduction
Immune checkpoint inhibitors (ICIs) are a common treatment for various malignancies. ICIs can be used against advanced stage melanoma not only in anti-PD1 or anti- CTLA-4 monotherapy but also in combination therapies. Despite their significant clinical benefits, these therapies are associated with several, immune-related adverse events (irAEs). Although an algorithm has been developed to handle irAEs, few previous studies have examined serious liver injuries associated with ICI administration. Herein we report a case of fatal hepatitis in a patient receiving nivolumab (anti- PD-1) and ipilimumab (anti-CTLA-4) combination therapy for melanoma. Although pulse methylprednisolone and plasmapheresis were administered, the liver failure led to thrombotic thrombocytopenic purpura (TTP) and eventual death.
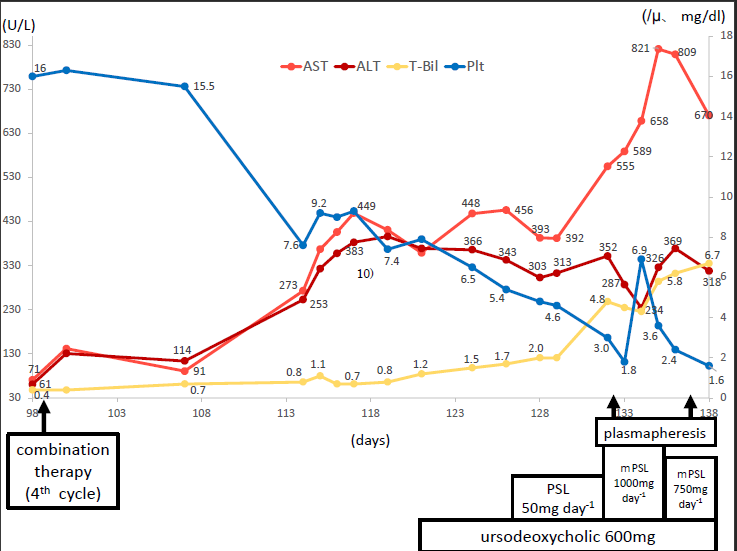
A 62-year-old female patient presented with a pigmented macule on the right, lower leg which had been present since age 11 years and became elevated three years prior to her visit. Malignant melanoma was diagnosed based on histopathological findings (Figure 1). Analysis of a sentinel lymph node biopsy specimen returned positive, and the lymph node was dissected after tumor resection. Advanced stage IIIb melanoma pT3aN1bM0, was diagnosed. Because ICIs were not able to be administered as adjuvant therapy, interferon-β was injected locally. At postoperative three years, a lung metastasis was detected, and nivolumab monotherapy was initiated. Despite 23 cycles of the therapy, the metastasis enlarged (Figure 2a-d). Ipilimumab was therefore added to the treatment regimen. After two administration of this combination therapy, the patient complained of malaise and loss of appetite. Her serum adrenocorticotropic hormone (ACTH) and cortisol levels decreased, and her response on a corticotropin releasing hormone (CRH) tolerance test and insulin tolerance test was poor (Figure 2e). She was diagnosed with sequel adrenal hypofunction possibly associated with the combination therapy. The therapy was therefore discontinued. Her symptoms were improved after hydrocortisone 15 mg/day and levothyroxine 75 μg/day administrations, and the combination therapy was resumed. Around the time the adrenal hypofunction was detected, a 3-cm diameter patch of hair loss appeared, which gradually expanded to cover the entire scalp. Alopecia areata was diagnosed, and steroid ointment was prescribed to no effect (Figure 2f). After four cycles of combination therapy, she complained of malaise again. Laboratory tests indicated not only a low cortisol level (4.08μg/dl), but also common terminology criteria for adverse events (CTCAE) version 4.0 grade 3 liver dysfunction with rapid AST and ALT elevation. Because hepatitis B surface (HBs) antigen, HBs antibody, hepatitis C virus antibody, anti-nuclear antibody, and anti- smooth muscle antibody were negative, autoimmune hepatitis was denied. Thus, the hepatitis was determined to be caused by ICI administration, and the patient was given ursodeoxycholic acid and prednisolone 50 mg/day as countermeasures. Despite these treatments, the AST and ALT levels continued to rise, and pulse methylprednisolone 1000 mg was added but failed to ameliorate the hepatitis. Fever, renal failure, unconsciousness, decreased platelets, and schizocytes developed, and TTP appeared as a complication. Plasmapheresis was performed, the patient succumbed to her condition (Figure 3).
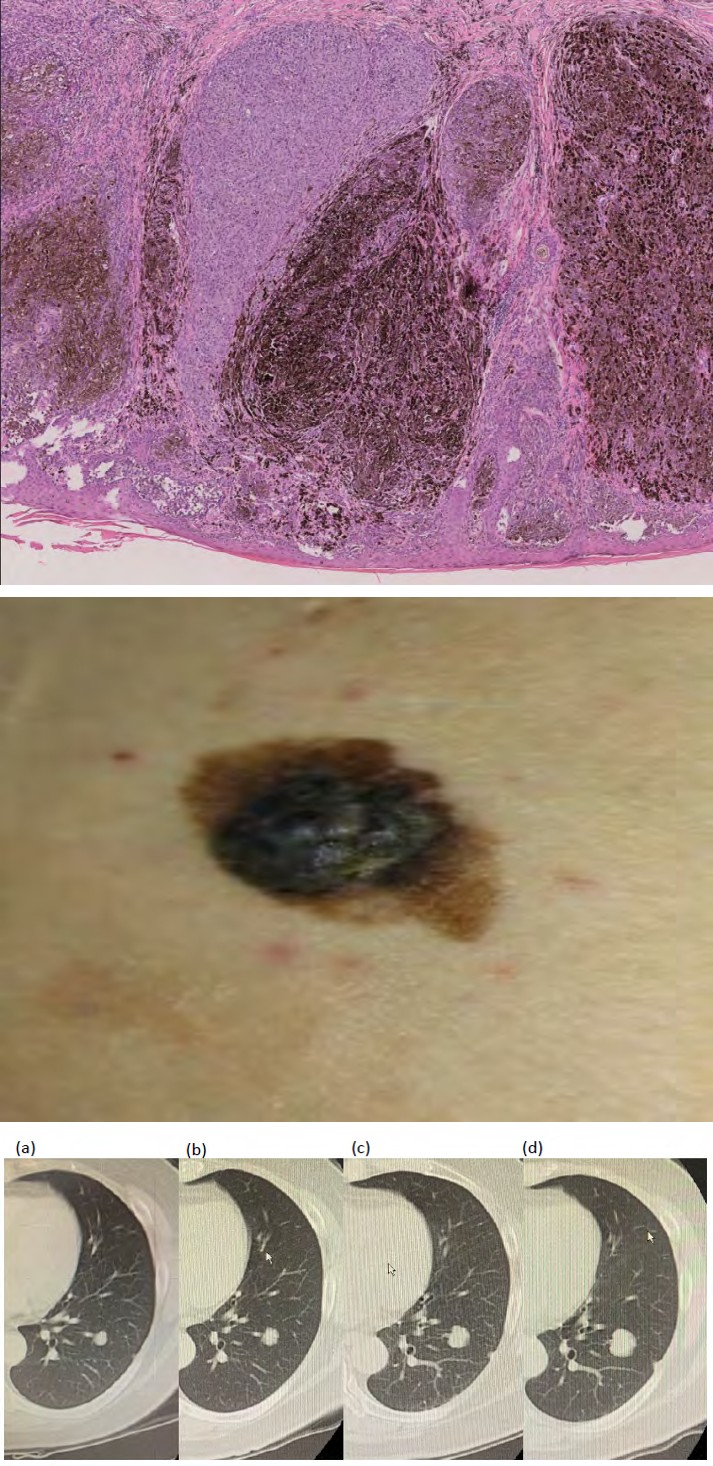
1(a) 1(b) Figure 1(a) Focal, blackish nodule on right lower limb. (b) Histology. Hematoxylin and eosin staining showing solid nest formed from atypical cells. There was an increased number of melanin granules (×20).
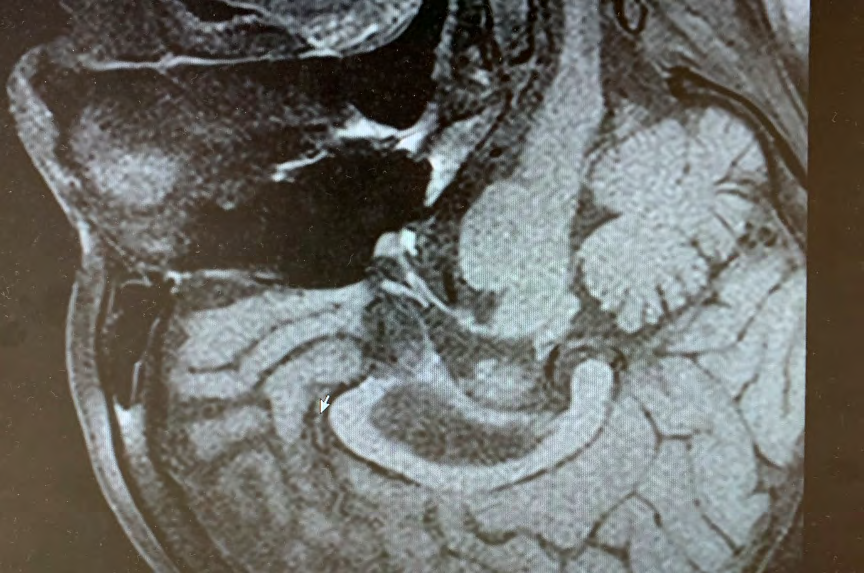
2(e) 2(f) Figure 2: Computed tomography of chest. Arrow indicates lung metastasis. (a) Before nivolumab, (b) after 10 cycles, (c) after 15 cycles, (d) after 23 cycles (>20% enlargement). (e) Head MRI during adrenal hypofunction. No tumorous lesion was found in the pituitary gland. The posterior lobe showed an area of signal intensity on T1W1 imaging. (f) Sparse hair and 3-cm diameter alopecia in the occiput.
Discussion
ICIs enhance the immune system’s ability against cancer. Within the past ten years, various forms of ICI have been approved for use against 14 kinds of malignancy. The five- year survival rate in patients with advanced stage melanoma was 44% in a nivolumab monotherapy group and 26% in an ipilimumab monotherapy group in comparison with 52% in a combination therapy group [1], demonstrating the remarkable efficacy of combination therapy against this disease.
Despite their efficacy, ICIs are associated with a variety of irAEs. A previous study reported irAEs in 87%, 86%, and 96% of patients with advanced melanoma in a nivolumab, ipilimumab, and combination therapy group, respectively; the respective rate of grade 3 and 4 irAEs was 23%, 28%, and 59% [1]. Combination immunotherapy demonstrated a significantly increased risk of irAEs, but this effect was observed when nivolumab and ipilimumab were administered either concurrently or sequentially [2]. In particular, hepatitis of all grades occurred in up to 33% of patients receiving combination therapy compared with a rate of 62% for skin disorders and 48% for colitis. However, the rate of high-grade irAE (grades 3-4) manifesting as hepatitis was only 20% while that of skin disorders and colitis was 6% and 15%, respectively. Thus, while the frequency of hepatitis as an irAE was not high, the cases were likely to be severe.
Hepatitis reportedly occurs 5-12 weeks after the start of therapy [3]. As hepatitis is diagnosed on the basis of abnormal changes in AST, ALT, and total bilirubin, periodic monitoring is necessary. Possible risk factors for hepatotoxicity include concomitant use of ICIs, coexistence of other irAEs, underlying chronic comorbidities, and high- dose ICI administration (e.g., the ipilimumab dosage for melanoma is 3 mg/kg and 1 mg/kg for renal carcinoma) [4]. Additionally, increased levels of antinuclear antibody, extractable nuclear antigen antibody, and anti-smooth muscle antibody were reported as irAE risk factors [5]. On the other hand, because differentiating irAE hepatitis from autoimmune hepatitis solely on the basis these laboratory findings is difficult, a liver biopsy should be performed to confirm the diagnosis. High-grade hepatitis associated with ICI use demonstrated a histopathologic pattern similar to that of acute hepatitis [6] and was also characterized by increased portal vein and panlobular, CD8-predominant T-cell infiltration [7] and fibrin-ring granulomas, especially in patients receiving anti-CTLA-4 antibodies [4]. The inflammatory infiltrates in hepatitis caused by ICIs mainly comprised activated lymphocytes and histiocytes, with only very few or no plasma cells [8]. In autoimmune hepatitis by contrast, plasma cell infiltration is a major finding. These histological features are useful for distinguishing irAE- related hepatitis from autoimmune hepatitis.
A previous study of lethal, toxic effects associated with ICI use reported that the mortality rate resulting from hepatotoxicity was 10% to 17% of all reported cases of irAE- related hepatitis, which was the second highest rate after pneumonitis-related morality in patients treated with anti- PD-1 or anti-PD-L1 antibodies [9]. However, the differences in the frequency of fatal hepatitis for each type of carcinoma remains unclear.
In the present case, grade 3 hepatitis occurred after the fourth course of nivolumab plus ipilimumab combination therapy. If ursodeoxycholic acid had been switched to high- dose PSL administration at an early stage, the patient’s outcome might have been better. The worsening hepatitis led to the emergence of TPP as a complication. Despite pulse methylprednisolone and plasmapheresis, the liver injury progressed to grade 5. According to the recent report, the use of mycophenolate moferil (MMF) can improve liver function in steroid-refractory irAE hepatitis [10]. In our case, renal dysfunction (CCr 48ml/min) and thrombocytopenia prevented us to administer MMF. Because MMF may make the renal function worse and proceed thrombocytopenia. Although a single toxic effect caused death in most patients receiving ICI [9], in the present case, the combination therapy led to multiple, concurrent irAEs with alopecia areata and adrenal hypofunction manifesting before the fatal hepatitis. Hitherto there have been no reports of grade 5 hepatitis associated with ICI use in patients with malignant melanoma. In conclusion, speedy assessment and appropriate treatment are necessary when liver dysfunction is found in a patient receiving ICIs.
References
-
Larkin J, Chiarion-Sileni V, Gonzalez R, Jacques Grob J, Rutkowski P, et al. (2019) Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med 381: 1535-1546.
-
Zarrabi K, Wu S (2018) Risk of liver toxicity with nivolumab immunotherapy in cancer patients. Oncology 94: 259-273.
-
Postow AM (2015) Managing immune checkpoint- blocking antibody side effects. Am Soc Clin Oncol Educ Book pp: 76-83.
-
Jennings JJ, Mandaliya R, Nakshabandi A, Lewis HJ (2019) Hepatotoxicity induced by immune checkpoint inhibitors: a comprehensive review including current and alternative management strategies. Expert Opin Drug Metab Toxicol 15: 231-244.
-
Giannicola R, D’arrigo G, Botta C, Agostino R, Del Medico P, et al. (2019) Early blood rise in auto-antibodies to nuclear and smooth muscle antigents is predictive of prolonged survival and autoimmunity in metastatic- non-small cell lung cancer patients treated with PD-1 immune-check point blockade by nivolumab. Mol Clin Oncol 11: 81-90.
-
Koelzer HV, Rothschild IS, Zihler D, Wicki A, Willi B, et al. (2016) Systemic inflammation in a melanoma patient treated with immune checkpoint inhibitors-an autopsy study. J Immunother Cancer 4: 13.
-
Kim WK, Ramaiya HN, Krajewski MK, Jagannathan JP, Tirumani SH, et al. (2013) Ipilimumab associated hepatitis: imaging and clinicopathologic findings. Invest New Drugs 31: 1071-1077.
-
Martin DE, Michot JM, Papouin B, Champiat S, Mateus C, et al. (2018) Characterization of liver injury induced by cancer immunotherapy using immune checkpoint inhibitors. J Hepatol 68(6): 1181-1190.
-
Wang YD, Salem JE, Cohen VJ, Chandra S, Menzer C, et al. (2018) Fatal toxic effects associated with immune checkpoint inhibitors. JAMA Oncol 4: 1721-1728.
-
Omori G, Takada K, Murase K, Hayasaka N, Nakamura H, et al. (2020) Successful mycophenolate mofetil treatment of a patient with secere steroid-refractory hepatitis evoked by nivolumab plus ipilimumab treatment for relapsed bladder cancer. Clin Case Rep 9(2): 654-659.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling