Three Cases of Nasal and Oral Mucosal Melanoma Showing Pseudo-Progression after Immune Check Point Inhibitor Treatment
Mucosal melanoma is rare, comprising fewer than 2% of all cases of melanoma. Its prognosis is poor, with the five-year survival rate being lower than in patients with cutaneous or uveal melanoma. The current absence of treatment guidelines contributes to the poor prognosis. Immuno-checkpoint inhibitors are known to cause pseudo-progression or immune- related adverse events (irAEs). Herein, we present three cases of mucosal melanoma of the head and neck treated with nivolumab, pembrolizumab, and ipilimumab. All three cases showed pseudo-progression after nivolumab treatment. In Case 3, seronegative rheumatic irAE with multiple muscle pain and arthralgia developed 30 months after nivolumab treatment although serological autoantibodies were negative. The response evaluation criteria in solid tumors (RECIST), which has long been the established method of assessing the treatment response in solid tumors, was ineffective for assessing the efficacy of immunotherapy due to immune-related patterns of response. Additional information concerning the incidence of immune- related responses is necessary to use the immune response criteria for treatment decisions.
Introduction
The malignant melanoma incidence continues to increase. Unresectable or metastatic melanomas have a poor prognosis, with a median survival time of six to eight months [1]. The immune checkpoint inhibitors (ICI), Anti-programmed death-1 (PD-1) antagonist (nivolumab, pembrolizumab) either alone or combined with CTLA- 4 antagonist (ipilimumab) is the standard treatment for metastatic melanomas [2] including mucosal melanomas in Japan.
Mucosal melanoma is rare. Its prognosis is poor, with the five-year survival rate being lower than that of cutaneous or uveal melanoma. There are currently no guidelines for staging or treatment [3].
The mucosal melanoma incidence differs by ethnicity. Among Caucasians, it accounts for less than 2% of all melanoma cases; in the Chinese population, the figure is 23% [4]. Mucosal melanoma is an aggressive subtype with a lower treatment response rate and shorter life expectancy to immunotherapy [4]. The response evaluation criteria in solid tumors (RECIST), the long standard assessment tool, is ineffective in evaluating the efficacy of immunotherapy due to some patients displaying immune-related responses not conforming to the RECIST criteria [5].
In ICI treatment, the tumor increases before responding to treatment in a phenomenon known as pseudo- progression, which may entail immune-related adverse events (irAEs). RECIST-based immune criteria (ir-RECIST) are recommended for assessing pseudo-progression [6]. Herein, we report three cases of mucosal melanoma with pseudo-progression and rheumatic irAE after PD-1 and CTLA-4 antibody treatment.
Case report
Case 1 A 79-year-old female patient presented a pigmented, nodular lesion on the anterior wall of the lower right concha. Malignant melanoma was diagnosed, and wide surgical excision and postoperative radiotherapy were performed in X-2 year. In Xyear, six courses of DAV-feron treatment with dacarbazine, nimustine, vincristine, and feron was administered every four weeks as adjuvant therapy after surgical excision of a brain metastasis. A loco-regional recurrence later detected in the posterior wall of the right nasal septum was surgically resected in X+2 year. In X+3 year, PET-CT revealed supraclavicular and mediastinal lymph node metastases, and second-line therapy with nivolumab 3 mg/kg was administered every three weeks. After 18 courses, new lymph node metastases developed on the bilateral neck (Figures 1A, 1B). After 34 courses, a lung metastasis developed, and from X+3 year, third-line therapy with ipilimumab 3 mg/kg was administered every three weeks. After the first cycle, treatment was stopped due to grade 2 pneumonia, and the patient was transferred to best supportive care (BSC).
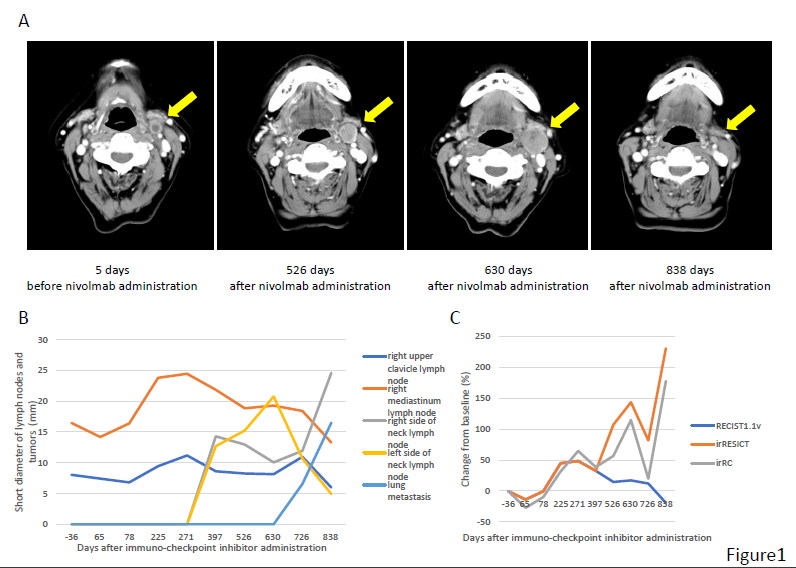
Figure 1: Metastasis to the lymph node on the left side of the neck during nivolumab treatment in Case 1 (A). Changes in metastatic tumor size in the lymph nodes and lung in Case 1 (B). The metastasis emerged after 18 courses increased from 13.2 mm to 23.1 mm (long diameter, +75%) after 30 courses, then decreased to 7.22 mm (-45%) after 39 courses (A, B). Changes from the baseline as assessed by RECIST, ir-RECIST, and ir-RC in Case 1(C).
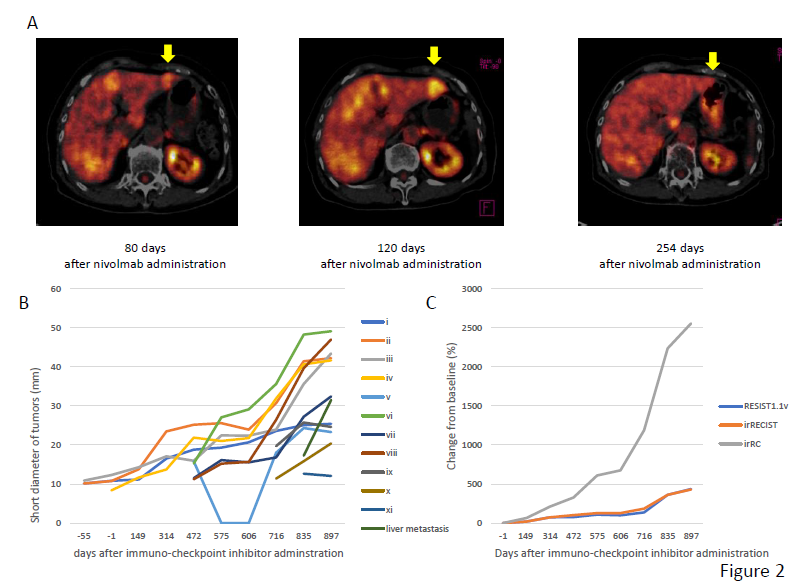
Case 2 A 60-year-old female patient presented with a black nodule on her gums, later diagnosed as malignant melanoma. After a wide surgical excision, postoperative DAV-feron treatment was administered every four weeks in Y year. In Y+2 year, DAV-feron treatment was stopped after a lung metastasis was found, and video-assisted thoracic surgery (VATS) was performed. In Y+3year, multiple lung metastases developed, and nivolumab 3 mg/kg was administered as second-line therapy every three weeks. After the fifth cycle, the patient experienced grade 1 vomiting which resolved spontaneously. One of the liver metastases was larger 120 days after treatment initiation. The SUVmax on PET-CT had also increased from 3.2 to 5.8, but was undetectable by day 254 (Figure 2A). However, follow-up CT five and ten months after treatment initiation revealed progression. Therefore, in Y+4 year, nivolumab was switched to third-line therapy with ipilimumab 3 mg/kg in four courses every three weeks. Follow-up CT revealed further lung metastases. In August 2016, nivolumab was restarted. However, due to progression of the lung and liver metastases, nivolumab was switched to pembrolizumab 2 mg/kg every three weeks in Y+5 year. Eight months later, pembrolizumab was stopped, and the patient was transferred to BSC (Figure 2B).
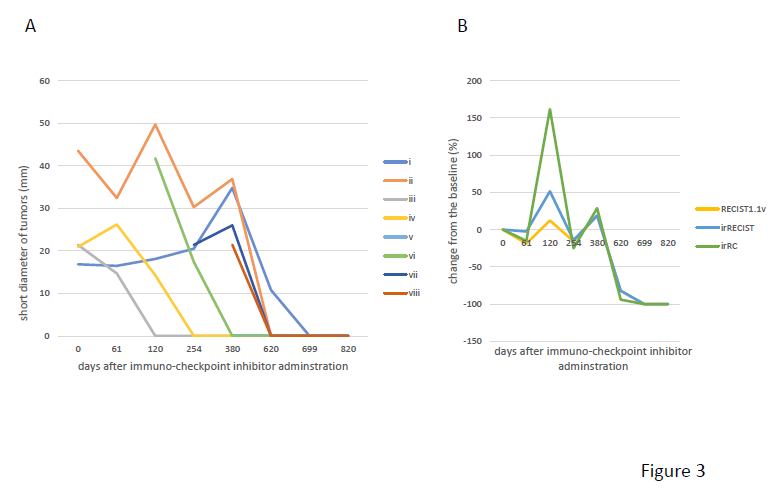
Case 3 A 79-year-old female patient presented with a tumor in the left ethmoid sinuse in Z year, which was later diagnosed as a malignant melanoma. She underwent wide surgical excision, postoperative heavy ion radiotherapy, and DAV- feron therapy. However, in Z+1 year, second-line therapy with nivolumab 3 mg/kg was administered every three weeks due to multiple liver metastases. From Z+1 year, a follow-up PET-CT and CT demonstrated disease progression until 12 months after treatment initiation. However, CT at 20 months revealed an increase in the diameter of one of the metastatic tumors. After 26 courses, the eight liver metastases resolved (Figure 3A). Muscle pain in multiple locations and arthralgia developed 30 months after treatment initiation. Laboratory tests were negative for serological autoantibodies (ANA<40, RF<5, anti-CCP antibody<0.6, C3 137 mg/d (normal range; 86-160mg/dL), C4 50.9mg/d (17-45 mg/dL). Nivolumab was stopped, and the disease was managed with oral prednisone. Follow-up PET-CT showed a complete treatment response. No BRAF mutation was detected in any of the cases.
Discussion
Since mucosal melanomas occur predominantly in the head and neck, they often lack subjective symptoms and are therefore frequently diagnosed at the advanced stage. Mucosal melanomas are an aggressive subtype resistant to conventional treatments for cutaneous melanoma. The reasons for the poor prognosis and the lower efficacy of ICI in mucosal melanomas are unclear. Unlike cutaneous melanomas, they rarely show BRAF mutations [6]; none of the present cases showed a BRAF gene mutation. However, other gene mutations have been reported in mucosal melanoma, such as c-KIT aberrations [7], RAS-mitogen-activated protein kinase pathway [8], and p16/ CDKN2A [9].
All the present cases showed pseudo-progression and received nivolumab. In Case 1, the lymph node on the left side of the neck markedly decreased after a period of growth. Similarly in Case 3, the eight liver metastases resolved after a period of growth. A previous study reported that 4% of patients with metastatic melanoma showed pseudo- progression after nivolumab treatment [10]. In another report, pembrolizumab and ipilimumab were associated with pseudo-progression in 2.8 and 8.9% of patients, respectively [11, 12].
Immune check point inhibitors cause a nonspecific overreaction of the immune system leading to immune- related adverse events (irAEs). In Case 2, vomiting and diarrhea were observed after the fifth cycle of nivolumab. The symptoms were grade 1 and resolved despite continued treatment. Case 3 showed a complete response to nivolumab but showed polymyalgia and arthritis development 30 months after treatment initiation. No autoantibodies were detected, and the patient was seronegative for rheumatic irAE. Calabrese, et al. [13] reported 13 patients with rheumatic symptoms during immunotherapy; 54%, 31%, and 23% had arthritis, sicca syndrome, and polymyalgia, respectively. Of the patients receiving immunotherapy, 38% were autoantibody-positive. Immunotherapy was stopped in 77% of these patients [13]. IrAEs reportedly correlate with the therapeutic effect of immunotherapy [14], with higher grade irAEs accompanying stronger therapeutic effects [15]. In Case 3, the patient received prednisone in addition to nivolumab for polymyalgia and polyarthritis and showed a complete response after experiencing grade3 irAEs.
Half the clinical trials to date have shown a small percentage of patients with immune-related responses, including pseudo-progression, not conforming to the RECIST criteria [5] despite irRECIST or irRC being the appropriate tool of evaluating ICI efficacy. Figures 1C, 2C and 3B show changes in the irRC from 100% to 1500% probably because the irRC formula multiplies the tumor diameter. The range of irRC results is relatively broad, and irRECIST may be more suitable for making treatment decisions. The immune response may differ depending on the tumor type and more data are necessary for optimal use of the immune response criteria.
References
-
Balch CM, Soong SJ, Gershenwald JE, Thompson JF, Reintgen DS, et al. (2001) Prognostic factors analysis of 17,600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol 19(16): 3622-3634.
-
Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, et al. (2015) Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N Engl J Med 373: 23-34.
-
Mihajlovic M, Vlajkovic S. Jovanovic P, Stefanovic V (2012) Primary mucosal melanomas: a comprehensive review. Int J Clin Exp Pathol 5(8): 739-753.
-
Wang X, Si L, Guo J (2014) Treatment algorithm of metastatic mucosal melanoma. Chin Clin Oncol 3(3): 38.
-
Chiou VL, Burotto M (2015) Pseudoprogression and Immune-Related Response in Solid Tumors. J Clin Oncol 33(31): 3541-3543.
-
D’Angelo SP, Larkin J, Sosman JA (2017) Efficacy and Safety of Nivolumab Alone or in Combination With Ipilimumab in Patients With Mucosal Melanoma: A Pooled Analysis. J Clin Oncol 35(2): 226-235.
-
Satzger I, Schaefer T, Kuettler U, Broecker V, Voelker B, et al. (2008) Analysis of c-KIT expression and KIT gene mutation in human mucosal melanomas. Br J Cancer 99(12): 2065-2069.
-
Lourenco SV, Fernandes JD, Hsieh R, Coutinho-Camillo CM, Bologna S, et al. (2014) Head and neck mucosal melanoma: a review. Am J Dermatopathol 36(7): 578- 587.
-
Hsieh R, Nico MMS, Coutinho-Camillo CM, Marcilei E Buim, Martin Sangueza, et al. (2013) The CDKN2A and MAP kinase pathways: molecular roads to primary oral mucosal melanoma. Am J Dermatopathol 35(2): 167- 175.
-
Topalian SL, Sznol M, McDermott DF, Harriet M Kluger, Richard D Carvajal, et al. (2014) Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J Clin Oncol 32(10): 1020-1030.
-
Hodi FS, Hwu WJ, Kefford R, Jeffrey S Weber, Adil Daud, et al. (2016) Evaluation of Immune-Related Response Criteria and RECIST v1.1 in Patients With Advanced Melanoma Treated With Pembrolizumab. J Clin Oncol 34(13): 1510-1517.
-
Wolchok JD, Hoos A, O’Day S, Jeffrey S Weber, Omid Hamid, et al. (2009) Guidelines for the evaluation of immune therapy activity in solid tumors: immune- related response criteria. Clin Cancer Res 15(23): 7412- 7420.
-
Rakoczi E, Szekanecz Z (2017) Pneumococcal vaccination in autoimmune rheumatic diseases. RMD Open 3(2): e000484.
-
Teulings HE, Limpens J, Jamsen SN, Aeilko H Zwinderman, Johannes B Reitsma, et al. (2015) Vitiligo- like depigmentation in patients with stage III-IV melanoma receiving immunotherapy and its association with survival: a systematic review and meta-analysis. J Clin Oncol 33(7): 773-781.
-
Downey SG, Klapper JA, Smith FO, James C Yang, Richard M Sherry, et al. (2007) Prognostic factors related to clinical response in patients with metastatic melanoma treated by CTL-associated antigen-4 blockade. Clin Cancer Res 13(22 Pt 1): 6681-6688.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling