Effectiveness of Ceramide Moisturizer in Atopic Dermatitis Systematic Review and Meta-analysis with Transepidermal Water Loss Parameters
Background: Atopic dermatitis (AD) is a chronic pruritic inflammatory disorder characterized by skin barrier dysfunction. This dysfunction manifests as increased transepidermal water loss (TEWL) and increased penetration of allergens and infectious agents, leading to inflammation and itching. Atopic dermatitis most commonly occurs in children, but can also be found in adults. Dryness and barrier dysfunction in atopic dermatitis are considered to be caused by a decrease in ceramide levels in the stratum corneum. Topical moisturizers, such as ceramide, are considered to be able to solve this problem by acting as a barrier repair agent. Objective: To prove the effectiveness of topical ceramide moisturizer compared to other topical moisturizers against atopic dermatitis. Methods: The result of an electronic database search of Medline, Pubmed, Scopus, EBSCOhost, ProQuest, Google Scholar, Cochrane library, ClinicalTrials.gov, and others found 6 articles included in the qualitative review (n = 270 subjects) and 3 articles (n = 32 subjects) were included in the meta-analysis. Results: Meta-analysis showed that the group of patients with atopic dermatitis who used topical ceramide moisturizer showed a difference in TEWL score before and after treatment, and the mean difference showed a negative value. This suggests that there was a decrease in TEWL scores after using topical ceramides Moisturizer. The control group also had similar mean TEWL score decrease. This suggests that other moisturizers can also reduce TEWL scores in the control group. The largest decrease in TEWL scores was found in Tabri, et al's 2018 study, which showed mean ±SD -24.46+5.53 reduction after using topical ceramides. The lowest decrease in TEWL scores was found in Kircik et al.'s 2014 study using topical petrolatum, which showed mean±SD -2.175±7.43. The result of the heterogeneity test showed the value of p = 0.478, I2 = 0.000. This shows the data is homogeneous, and thus the analysis was carried out using a fixed- effect model. Statistical data obtained showed that topical ceramide moisturizer given to atopic dermatitis (p=0.168) produced no significant results. Conclusions: The results of the meta-analysis were not statistically significant. However, in the ceramide moisturizer group, the overall trend of TEWL score decrease was greater than in the control group. The findings of the qualitative analysis revealed that using a topical ceramide moisturizer may lower the TEWL score and enhance skin barrier function in atopic dermatitis patients and that it had the same effect as other topical moisturizers.
Introduction
Atopic dermatitis (AD) is a chronic pruritic inflammatory disorder characterized by a breakdown of the skin barrier. Changes in the barrier allow allergens and infectious organisms to penetrate deeper into the skin, resulting in chronic inflammation. Atopic dermatitis is an example of an inflammatory skin condition with skin barrier dysfunction characterized by increased transepidermal water loss (TEWL), decreased stratum corneum hydration, increased pH, and decreased sebum levels/changes in lipid composition [1, 2, 3].
Skin barrier dysfunction in atopic dermatitis is mainly related to decreased levels of ceramides in the stratum corneum with manifestations of increased TEWL. Ceramides act as a water modulator and permeability barrier by forming a layered lamellar structure with other lipids between cells in the stratum corneum [4]. Matsumoto, et al. reported that the ceramide I, long-chain ceramide, decreased by 52% in atopic dermatitis [5]. In addition, ceramide V level in non-lesioned parts of the skin was raised, and ceramide I and ceramide III were reduced in lesioned parts of the skin [6, 7]. Moreover, the metabolism pathways such as ceramidase are overactive in the epidermis with atopic dermatitis [8]. In another study, Chermprapai, et al. postulated that in atopic dermatitis, free fatty acid concentration was decreased along with ceramide level [9].
The management of atopic dermatitis is mainly aimed at reducing signs and symptoms of the disease, preventing/ reducing recurrence, and changing the course of the disease [10]. The best therapeutic approach is to improve skin barrier function with regular use of moisturizers and avoidance of irritants [11]. According to a recent study, it was shown that a topical agent containing a mixture of the three main stratum corneum lipids consisting of ceramides, cholesterol, and free fatty acids in optimal proportions (3:1:1) can accelerate the restoration of the stratum corneum barrier [12, 13, 14]. Other studies have shown that adding ceramides to moisturizers or making moisturizers similar to natural lipids has beneficial effects; which acts as a barrier repair formulated to mimic natural ceramide composition found in healthy skin [4, 15].
TEWL measurement is a standard method to assess the function of the stratum corneum barrier by measuring water evaporation through the skin [16]. The purpose of this study was to evaluate the effect of ceramide topical moisturizers on improving the skin barrier of atopic dermatitis patients using the key parameter TEWL. Ceramide topical moisturizers are expected to be effective and clinicians may consider their topical application as an alternative for skin barrier repair, especially in atopic dermatitis.
Methods
Literature Search
This study was a systematic review and meta- analysis, and it followed the Cochrane handbook [17] and PRISMA statement [18] as guidelines. Literature search was performed on Pubmed-MEDLINE, Scopus, EBSCO, Cambridge Core, ProQuest, Cochrane Library, ClinicalTrials. gov, and Google Scholar database. Furthermore, reference lists of relevant publications and relevant literature reviews were searched to identify other eligible studies. Three reviewers independently conducted the literature search. The following terms were used for searching in PubMed- MEDLINE and Cochrane: ((“ceramides”[MeSH Terms]) AND “atopic dermatitis”[MeSH Terms] AND “transepidermal water loss”[MeSH Terms]. Other databases were also searched using similar.
Study Selection and Data Extraction
Studies were selected based on the 2009 PRISMA flowchart [18]. The abstracts of the citations obtained from the initial broad search were screened independently by three reviewers to identify potentially eligible studies. They used the predefined eligibility criteria to independently assess full-text articles of these studies for eligibility. Multiple publications from the same studies were included only if any additional information was available; otherwise, they were considered duplicates, and the information was used only once.
Eligibility criteria mentioned are as such: clinical trials with atopic dermatitis, and used topical ceramides as an interventional arm. The primary outcome of this study was TEWL. Data extraction was performed independently by the three reviewers using The Cochrane Collaboration data collection form for RCTs [17]. Any disagreements in the paper selection and data extraction were resolved by consensus.
Statistical Analysis
Meta-analysis was performed using weighted mean of mean differences between the treatment and control groups. Review Manager Version 5.4.1, was used in the analysis. The I2 was used to calculate the heterogeneity of each outcome. If no heterogeneity was found, data were analyzed using fixed-effects meta-analysis. However, if heterogeneity was found (I2 > 50%), random effect analyses would be used. When data from the article couldn’t be included in the meta- analysis, descriptive research was performed.
Assessment of Risk of Bias
The quality of evidence for each study was assessed using the Cochrane Risk of Bias Tool for Randomized Controlled Trials [19].
GRADE Evidence The key information concerning the quality of evidence was assessed as per GRADE guidelines [20]. All authors discussed and agreed with GRADE allocation.
Result
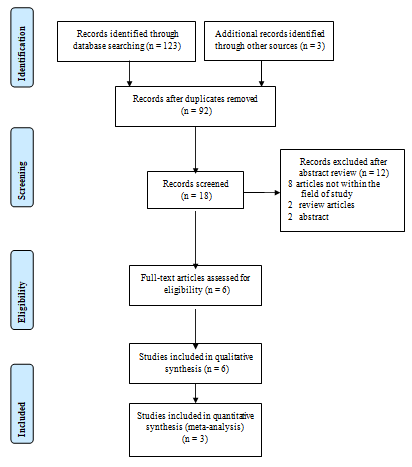
Initial searching of databases yielded 126 studies. Removal of duplicates and record screening reduced the number down to 18 relevant article titles. Their abstracts were then again screened to exclude 12 articles as follows: two review articles, eight research articles that were not relevant to the meta- analysis, and two abstracts. Finally, six complete articles were reviewed for eligibility, and none were found to be ineligible. Six research articles were used in qualitative studies and three articles in quantitative studies to assess the effectiveness of topical ceramides on the skin barrier conditions of atopic dermatitis [3, 15, 21, 22, 23, 24]. The selection process is presented in Figure 1.
Research Characteristics
The majority of the studies were carried out in Indonesia (n=3), followed by the United States (n=1), Australia (n=1), and the Netherlands (n=1). All of those studies were conducted between 2014-2021. The total sample from those 6 studies was 270 people, consisting of 214 adult patients, 16 pediatric patients, and 32 mixed pediatric-adult patients. The characteristics of included studies are presented in Table 1.
| No | Authors, Year | Country | Sample Size | Population | Study Arms | Frequency | Duration | |
|---|---|---|---|---|---|---|---|---|
| 1st Interventional Arm | 2nd Interventional Arm | |||||||
| 1 | Mustifah et al, 2017 | Indonesia | 14 | Adult (23-35 years) | ceramides cream | aloe vera cream | twice a day | two weeks |
| 2 | Tabri et al, 2018 | Indonesia | 16 | Child (2-4 years) | ceramides cream | petrolatum cream | twice a day | two weeks |
| 3 | Kircik et al, 2014 | USA | 10 | Child-Adult (above 7 years old) | epicream (ceramides) | eucerin lotion (petrolatum) | not mentioned | four weeks |
| 4 | Spada et al, 2021 | USA | 100 | Adult (18-73 years) | ceramides cream and ceramides cleanser | no | twice a day | four weeks |
| 5 | Umborowati et al, 2020 | Indonesia | 30 | Child-Adult (8- 18 years) | ceramide cream as the main ingredient added with menthol and polidocanol | placebo cream and placebo cleanser | twice a day | four weeks |
| 6 | Koppes et al, 2016 | Netherland | 100 | Adult (18-70 years) | Ceramide-Magnesium combination cream | unguentum leniens (em, also called cold cream, consists of Arachis oil (peanut oil), purified water, white beeswax, and glyceryl monooleate) | twice a day | six weeks |
Table 1: Characteristics of included studies.
Qualitative Data Analysis (Systematic Review)
Six literatures were analyzed qualitatively. Their results were as follows: Mustifah, et al. conducted a study on 14 atopic dermatitis patients and found that topical ceramide application twice a day for two weeks tended to decrease TEWL. Comparable results were found in the aloe vera group. Overall, it was found that TEWL scores were lower with ceramide cream than with aloe vera cream, but the difference was not significant: F value was 0.433, and p-value was 0.512. Since there was no significant difference in TEWL score, both products’ efficacy was assumed to be equal.
Tabri, et al. included 16 atopic dermatitis patients in their study. Topical ceramide was applied twice a day for two weeks. Compared to the initial TEWL measurement, all subjects significantly decreased the TEWL value. Compared to other moisturizers, ceramide cream had the greatest decrease in TEWL value, followed by lanolin, urea, and vaseline album. The decrease in TEWL value was more significant after 7 days of application than after 14 days, although the difference was not statistically significant.
Kircik, et al. conducted a study on 14 atopic dermatitis patients. Ceramide cream and petrolatum lotion were applied twice a day for four weeks. Although there was no statistically significant difference between the two groups in terms of overall median hydration improvement, it was higher in the topical ceramide group. Compared to baseline, ceramide cream enhanced overall median percentage hydration by 55 percent at week 4, while petrolatum lotion improved by 37 percent.
Spada, et al. conducted a study on atopic dermatitis patients. Ceramide cream and cleanser were applied twice a day for four weeks. Compared to the placebo, the ceramide cream and cleanser significantly improved barrier function, as indicated by a lower TEWL value.
Umborowati, et al. conducted a study on 30 atopic dermatitis patients. A ceramide-dominant cream with menthol and polidocanol was used twice a day for four weeks, and TEWL was significantly improved after cream application. The average TEWL level at the end of the study was decreased from baseline, and this significant decrease appeared as soon as 5 minutes after drug application.
However, there was no significant difference in TEWL decrease between 5 minutes and 1-week evaluation.
Koppes, et al. conducted a study on 100 atopic dermatitis patients. Patients were instructed to apply one fingertip unit (approximately 1g) of Cer-Mg cream twice daily for 6 weeks. The Cer-Mg treatment did not significantly change the TEWL from the baseline, while the EM treatment showed a significant increase in TEWL at 3 weeks. At both time intervals, the change in TEWL from baseline was substantially more significant following EM than Cer-Mg. The present study shows that, after 6 weeks of treatment, Cer-Mg cream offers benefits over high lipid-EM.
Quantitative Data Result (Meta-Analysis)
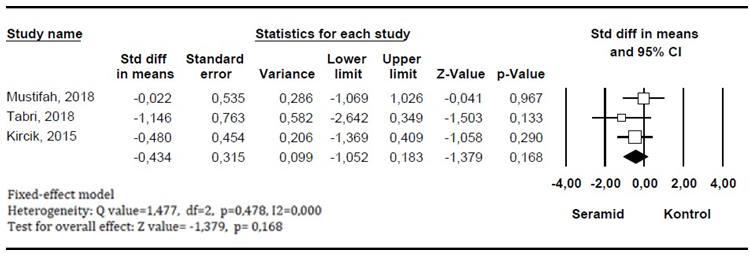
Meta-analysis was carried out using the studies by Mustifah, et al., Tabri et al. and Kircik, et al. The result of the meta-analysis showed that the overall mean difference in TEWL between the ceramide group and the control group was -0.434 ± 0.3146 (95% confidence interval = -1.052 to 0.183) with a p-value of 0.168. This shows that the overall trend of TEWL values’ decrease in the group receiving ceramides is more significant than that in the control group. However, due to the range of confidence intervals that include zero, the p-value is not significant (p = 0.168). Sensitivity analysis by excluding one of the studies included in the meta-analysis did not change the overall significance of the analysis.
Risk of Bias from the Included Studies
Mustifah, et al., Tabri, et al. and Kircik, et al. did not explicitly state how the randomization, random allocation, and blinding process were conducted. In the three studies, no source of bias from selective reporting, incomplete outcomes, or other bias was found. The research by Umborowati, et al. did not perform randomization methods and allocation concealment, thus putting it the too low quality of evidence. The study by Spada, et al. had a high risk of bias from incomplete outcome data. The research by Koppes, et al. had a high risk of bias by not blinding participants and personnel.
Research by Koppes, et al. and Spada, et al. had a low risk of bias from other assessment categories, and so they were categorized as the fair quality of evidence. Table 2 shows the risk of bias in the included studies.
GRADE Evidence The quality of evidence in the meta-analysis was assessed using GRADE. The certainty of the evidence for TEWL outcome between ceramide to other moisturizers was downgraded due to the imprecision factor caused by wide CIs in one of the studies. The GRADE assessment of the meta- analysis is presented in Table 3.
| Random Sequence Generation | Allocation Concealment | Selective Reporting | Other Bias | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Standard AHRQ | |
|---|---|---|---|---|---|---|---|---|
| Mustifah et al. 2017 | ? | ? | + | + | ? | ? | + | fair |
| Tabri et al. 2018 | ? | ? | + | + | ? | ? | + | fair |
| Kircik et al. 2014 | ? | ? | + | + | ? | ? | + | fair |
| Spada et al. 2021 | + | + | + | + | + | + | red | fair |
| Umborowati et al. 2020 | red | red | + | + | + | + | + | poor |
| Koppes et al. 2016 | + | + | + | + | red | + | + | fair |
Table 2: Risk of bias of included studies
| Certainty assessment | No of patients | Effect | Certa inty | Import ance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No of studies | Study design | Risk of bias | Inconsi stency | Indirect ness | Impreci sion | Other considera tions | Ceramide | Control | Relative (95% CI) | Absolute (95% CI) | ||
| Transepidermal Water Loss | ||||||||||||
| 3 | randomiz ed trials | not serious | not serious | not serious | serious | None | 21 | 21 | - | SMD 0.434 SD lower (1.052 lower to 0.183 higher) | Mode rate | IMPORT ANT |
Table 3: GRADE Assessment of meta-analysis.
Discussion
There is a change in typical skin characteristics in atopic dermatitis, resulting in skin barrier dysfunction. Abnormal protein (filaggrin and related proteins) and lipid metabolism, especially ceramides, are responsible for the complex pathophysiology of atopic dermatitis. Ceramides act as water- binding molecules in the extracellular space of the stratum corneum [25]. Decrease in ceramides level might be due to increased sphingomyelin deacylase activity and decreased ceramide synthesis by keratinocytes, resulting in increased TEWL, dry skin, and susceptibility to environmental irritants and allergens [26].
New formulations, such as therapeutic moisturizers (e.g., ceramide moisturizers), have been created in recent years to replace deficient substances involved in the dry skin mechanism and restore the natural balance of the epidermal barrier. The use of ceramide moisturizers has advantages over other types of moisturizers due to their ability to penetrate the skin, affect the structure and function of the barrier, promote epidermal differentiation, and correct ceramide deficiency among corneocytes, which are among the etiologies of atopic dermatitis [27, 28]. Research reports show that adding ceramides to moisturizers or making natural (synthetic) lipid-like moisturizers has a beneficial effect on the skin with atopic dermatitis. This synthetic ceramide moisturizer acts as a barrier repair and is formulated to mimic the natural ceramide composition found in healthy skin [4, 15].
The quantitative analysis from the studies conducted by Mustifah, et al., Tabri, et al. and Kircik, et al. showed similar results, in which the mean TEWL difference between the ceramide group and the control group had a negative value. This indicates a decrease in TEWL scores after treatment with topical ceramides compared to the control group. The overall mean different value of TEWL between the ceramide group and the control group was mean±SD -0.434±0.3146 (95% confidence interval = -1.052 to 0.183) with p-value = 0.168. This demonstrates that the overall trend of TEWL decrease in the ceramides group is more significant than in the control group, although the difference is not statistically significant.
A possible explanation for the statistically insignificant result may be the insufficient number of samples in the articles. Another potential cause for this is that environmental variables like humidity, temperature, and ventilation might alter the accuracy of the TEWL measurement; hence it is crucial to do it in controlled environments [29]. The studies conducted by Tabri, et al. and Kircik, et al. do not meet these criteria, so they may have measurement bias. The condition recommended by the European Group of Efficacy Measurement of Cosmetics and other Topical Products (EEMCO) is to set the examination room with limited circulation at a temperature of 20 – 22 ± 1°C with a relative humidity of less than 60% [30]. According to other research, moisture loss in the stratum corneum can occur when humidity levels are below 10% [31].
The qualitative analysis of studies by Mustifah, et al., Kircik, et al. and Koppes, et al., showed that there was a tendency for the value of TEWL to decrease, but the difference was not significant. Thus, it can be concluded that the ceramide group had equal effectiveness to other groups. The research by Tabri, et al. showed that using ceramide cream can significantly decrease TEWL compared to other moisturizers. The research by Spada, et al. showed that using ceramide creams and cleansers tended to decrease TEWL values compared to placebo significantly. Umborowati, et al. showed that the use of ceramide cream could maintain low TEWL levels with a regular application for 4 weeks.
Since there was no significant difference in TEWL between the two populations, this study did not discriminate between children and adults. This is consistent with the research, which claims that TEWL scores do not differ between children and adults [32].
The duration of therapy in this study ranged from two to six weeks. Johannesson and Hammar used dansyl chloride staining to examine the stratum corneum and found that the average rate of stratum corneum formation was 1.15+0.09 (mean+SE) layers per 24 hours. Given that the stratum corneum contains an average of 16 layers, the turnover time is 13.91 days. The average duration for stratum corneum turnover was 14 days, with layer creation occurring every 21 hours [33].
The frequency and duration of use of these moisturizers vary. The articles used in this study mentioned applying the Moisturizer two times a day, while other articles did not mention the frequency used. One article states that after a moisturizer is applied, its ingredients will stay on the skin’s surface, be absorbed into the skin, metabolized, or evaporate due to evaporation, regardless of whether the skin comes in contact with other ingredients or not. After 8 hours, only 50% of the moisture remains on the skin’s surface. Moisturizer should be applied between 1 to 3 times per day, depending on skin condition [34].
However, there were some limitations to this study. Research articles examining the effectiveness of ceramide for skin barrier repair were limited. The small number of subjects in the publications makes it difficult to generalize the findings, particularly for TEWL outcomes. Furthermore, there were discrepancies in the ambient circumstances of the included studies that did not fulfill the measurement standards, which could have affected the results.
Conclusion
Topical ceramide application may improve the skin barrier, characterized by a decrease in TEWL. However, compared to other examined moisturizers, the decrease in TEWL after ceramide application was not statistically significant. According to the GRADE evaluation, further study is needed to determine the efficacy of ceramide and other moisturizing treatments as barrier repair. Further research using TEWL measurement in a controlled environment with modified temperature and humidity might help to reduce the confounding effect. It would also be beneficial to have a control group with more participants.
References
-
Giam YC, Hebert AA, Dizon MV, Van Bever H, Tiongco- Recto M, et al. (2016) A review on the role of moisturizers for atopic dermatitis. Asia Pac Allergy 6(2): 120-128.
-
Moinzadeh P, Christopher P, Denton, Black CM, Krieg T (2019) Systemic Sclerosis. In: Kang S, Amagai M, et al. (Eds.), Fitzpatrick’s Dermatology in General Medicine. 9th (Edn.), McGraw-Hill Education, New York, pp: 1086- 1095.
-
Mustifah EF, Dewi SR, Hastuti R, Kariosentono H (2018) Perbandingan Fungsi Barrier Kulit Pasien Dermatitis Atopik antara Krim Aloe Vera dan Krim Seramid Penelitian Awal. Cermin dunia Kedokteran 45(8): 571- 575.
-
Elias PM, Wakefield JS, Man MQ (2019) Moisturizers versus Current and Next-Generation Barrier Repair Therapy for the Management of Atopic Dermatitis. Skin Pharmacol Physiol 32(1): 1-7.
-
Pappas A, Kendall AC, Brownbridge LC, Batchvarova N, Nicolaou A, et al. (2018) Seasonal changes in epidermal ceramides are linked to impaired barrier function in acne patients. Exp Dermatol 27(8): 833-836.
-
Pilgram GS, van der Meulen J, Gooris GS, Koerten HK, Bouwstra JA, et al. (2001) The influence of two azones and sebaceous lipids on the lateral organization of lipids isolated from human stratum corneum. Biochim Biophys Acta 1511(2): 244-254.
-
Pilgram GS, Vissers DC, van der Meulen H, Pavel S, Lavrijsen SP, et al. (2001) Aberrant lipid organization in stratum corneum of patients with atopic dermatitis and lamellar ichthyosis. J Invest Dermatol 117(3): 710-717.
-
Qurt MS, Esentürk İ, Birteksöz Tan S, Erdal MS, Araman A, et al. (2018) Voriconazole and sertaconazole loaded colloidal nano-carriers for enhanced skin deposition and improved topical fungal treatment. Journal of Drug Delivery Science and Technology 48(1): 215-222.
-
Rabionet M, Gorgas K, Sandhoff R (2014) Ceramide synthesis in the epidermis. Biochim Biophys Acta 1841(3): 422-434.
-
Catherine Mack Correa M, Nebus J (2012) Management of patients with atopic dermatitis: the role of emollient therapy. Dermatol Res Pract 2012: 836931.
-
Eichenfield LF, Tom WL, Berger TG, Krol A, Paller AS, et al. (2014) Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol 71(1): 116-132.
-
Man MM, Feingold KR, Thornfeldt CR, Elias PM (1996) Optimization of physiological lipid mixtures for barrier repair. J Invest Dermatol 106(5): 1096-1101.
-
Mao-Qiang M, Brown BE, Wu-Pong S, Feingold KR, Elias PM, et al. (1995) Exogenous nonphysiologic vs physiologic lipids. Divergent mechanisms for correction of permeability barrier dysfunction. Arch Dermatol 131(7): 809-816.
-
Man MQ, Feingold KR, Elias PM (1993) Exogenous lipids influence permeability barrier recovery in acetone- treated murine skin. Arch Dermatol 129(6): 728-738.
-
Tabri F, Yuniati L (2018) A Randomized, Double-Blind Clinical Trial Comparing the Effects of 1% Ceramide, 10% Lanolin And 10% Urea Cream in Improving Skin Barrier Function of Children with Mild Atopic Dermatitis. International Journal of Science & Healthcare Research 3(4): 152-157.
-
Kikuchi K, Asano M, Tagami H, Kato M, Aiba S, et al. (2017) Comparison of the measuring efficacy of transepidermal water loss of a reasonably priced, portable closed- chamber system device H4500 with that of rather expensive, conventional devices such as Tewameter((R)) and Vapometer((R)). Skin Res Technol 23(4): 597-601.
-
Higgins J, Thomas J, Chandler J, Cumpston M, Li T, et al. (2019) Cochrane Handbook for Systematic Reviews of Interventions. 2nd (Edn.), John Wiley & Sons, Chichester, UK.
-
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7): e1000097.
-
Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, et al. (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343: d5928.
-
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, et al. (2011) GRADE guidelines: 1. Introduction- GRADE evidence profiles and summary of findings tables. J Clin Epidemiol 64(4): 383-394.
-
Kircik LH (2014) Effect of skin barrier emulsion cream vs a conventional moisturizer on transepidermal water loss and corneometry in atopic dermatitis: a pilot study. J Drugs Dermatol 13(12): 1482-1484.
-
Koppes SA, Charles F, Lammers L, Frings-Dresen M, Kezic S, et al. (2016) Efficacy of a Cream Containing Ceramides and Magnesium in the Treatment of Mild to Moderate Atopic Dermatitis: A Randomized, Double- blind, Emollient- and Hydrocortisone-controlled Trial. Acta Derm Venereol 96(7): 948-953.
-
Spada F, Harrison IP, Barnes TM, Greive KA, Daniels D, et al. (2021) A daily regimen of a ceramide-dominant moisturizing cream and cleanser restores the skin permeability barrier in adults with moderate eczema: A randomized trial. Dermatol Ther 34(4): e14970.
-
Umborowati MA, Nurasrifah D, Indramaya DM, Anggraeni S, Damayanti, et al. (2020) The role of ceramide, menthol and polidocanol on pruritus, skin barrier function, and disease severity of mild atopic dermatitis. Journal of Pakistan Association of Dermatologists 30(1): 98-105.
-
Leung DY, Boguniewicz M, Howell MD, Nomura I, Hamid QA, et al. (2004) New insights into atopic dermatitis. J Clin Invest 113(5): 651-657.
-
Leung DY, Jain N, Leo HL (2003) New concepts in the pathogenesis of atopic dermatitis. Curr Opin Immunol 15(6): 634-638.
-
Ho VPY, Ma E, Liew HM, Ng MSY, Koh MJA, et al. (2020) Comparing the Potential for Irritation of a Ceramide- Based Moisturizer with a Urea-Based Moisturizer for Pediatric Atopic Dermatitis. Dermatol Ther (Heidelb) 10(4): 807-813.
-
Galli E, Neri I, Ricci G, Baldo E, Barone M, et al. (2016) Consensus Conference on Clinical Management of pediatric Atopic Dermatitis. Ital J Pediatr 42(1): 26.
-
Sotoodian B, Maibach HI (2012) Noninvasive test methods for epidermal barrier function. Clin Dermatol 30(3): 301-310.
-
Berardesca E, Loden M, Serup J, Masson P, Rodrigues LM (2018) The revised EEMCO guidance for the in vivo measurement of water in the skin. Skin Res Technol 24(3): 351-358.
-
White-Chu EF, Reddy M (2011) Dry skin in the elderly: complexities of a common problem. Clin Dermatol 29(1): 37-42.
-
Honari G, Maibach H (2014) Chapter 1: Skin Structure and Function. In: Maibach H, Honari G (Eds.), Applied Dermatotoxicology, Academic Press, Boston, pp: 1-10.
-
Johannesson A, Hammar H (1978) Measurement of the horny layer turnover after staining with dansyl chloride: description of a new method. Acta Derm Venereol 58(1): 76-79.
-
Purnamawati S, Indrastuti N, Danarti R, Saefudin T (2017) The Role of Moisturizers in Addressing Various Kinds of Dermatitis: A Review. Clin Med Res 15(3-4): 75- 87.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling