Alopecia Areata
Background: Alopecia areata is a kind of recurring, non-scarring hair loss that can affect any hair-bearing location and exhibit itself in a variety of ways, causing emotional and psychosocial discomfort. Despite the availability of its treatment, many individuals suffering from AA refused to seek it due to misconception and lack of faith in its effectiveness. The objective of this study is to describe clinical presentation and outcome of an AA treatment. Methodology: Patient with the early stage of AA is involved in this case presentation with a scalp analysis performed to determine the cause of his hair loss. Treatment of intralesional triamcinolone acetonide is administered over the course of 2 months, complemented by Prednisone, Minoxidil and Vitamin C. Result: Rapid hair growth after 3rd injection of triamcinolone and 10mg of Prednisone in the patchy bald area, with the gradual growth of the hair base which completely covers the bald area in just 3 months. Conclusion: It is important to raise awareness among the general public of the option available to them should they suffer from AA with detailed clinical presentation and outcome of an AA treatment.
Introduction
Individuals with alopecia areata are dispersed around the globe, with those affected demanding treatment and diagnosis as their hair loss develops. Hair loss impairs a patient’s confidence and morale, necessitating urgent study to prevent and treat hair loss. As a result of their unusual appearance, patients with alopecia areata (AA) endured significant physiological, psychological, and social problems. In individuals with alopecia areata, there is a gradual onset of hair loss all hair on the scalp, often characterized as an unexpected bald spots occur in patches, as the hair follicles generate a chemical signal that triggers an immune response against them. This results in the loss of hair from these follicles. As long as the immune system continues to attack the follicles, no new hair will form.
On a social level, adults have lost their jobs, been harassed and treated with discrimination due to their appearance. The majority of individuals with AA often express concerns about their condition in relation to physical symptoms, emotional health, mental health, social functioning, and other aspects of everyday functioning. The common issue among people suffering from AA is the misconception or even lack of trust and awareness in the available treatments for this type of hair loss. Some patients who were consulted by us were even doubtful of the effectiveness of the available treatment, albeit choosing to carry through with it anyway as it is more of a risk-taking decision for them. In this paper we will elaborate the process of diagnosing and treating an individual with AA to demonstrate the reality of how this condition is treatable and the reliability of this treatment. This may help AA patients to be more confident with their choice, without feeling like they are blindly taking chances.
Patient and Method
A 55-year old Malaysian Chinese man presented a progressive Alopecia Areata in the parietal region. Based on his general health history, the patient does not have any medical problem and was enduring a stressful period of 6 months prior to his visit to the clinic due to his working condition. He started to notice a small bald patch in early 2021 after a trip to a barber. Initially, he thought the barber had mistakenly shaved off his hair around that area and did not take the matter any further. However, the patch began expanding later on and his friends started to notice the hair loss and point it out to him. Gradually, he became more aware and insecure with the widening patch. He visited the clinic on 3 October 2021 and came with the above complaint. He expressed his main concern, which is AA, without having any particular treatment in mind regarding his AA, thus he was advised on the matter and informed of the suitable treatment involved. Patient has never experienced any balding prior to this.
The pull test was performed on an area with hair growth to determine the diagnosis of his hair loss condition. Using the thumb, index, and middle fingers, around 50-60 hairs were gripped at their bases and pulled away from the scalp gently. Over 10% of the hair strands were extracted from the scalp, indicating active hair loss and a diagnosis of alopecia areata.
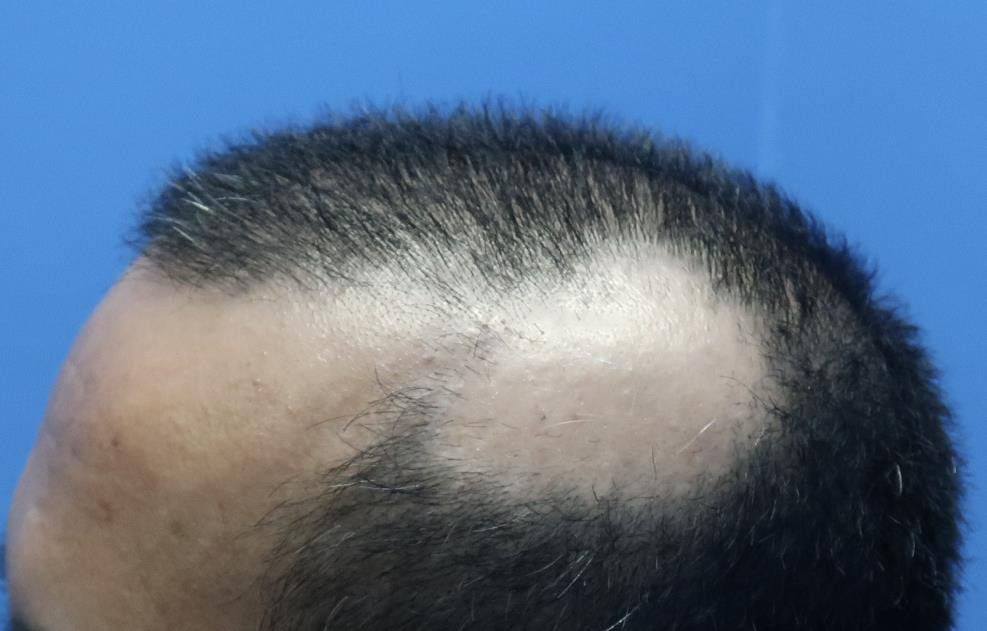
According to the analysis, his scalp displays patchy alopecia consisting of oval-shaped and flesh-colored lesions (Figure 1). Further assessment of the scalp shows broken hair shafts and the examination of the hair follicles under a microscope reveals the presence of oddly shaped hair, thinner closer to the scalp and resembles an exclamation point, as characterized by a distal broken shaft tip and a proximal club-shaped root.
Based on the history and physical examination findings, the patient had no underlying comorbidity that may have contributed to his hair loss and he was diagnosed with AA.
Treatment
For a treatment, intralesional triamcinolone acetonide is injected intradermally on the scalp using a 30-gauge, 0.5- inch needle. The maximum volume each session is 3 mL. The treatment is repeated every two weeks until the condition is resolved, up to 2 months, from October 2021 until November 2021.
Further treatment involving 20mg of Prednisone are prescribed orally for alternate-day dosing for 2 weeks. After that, the dose is reduced to 10 mg and is prescribed for alternate-day for 2 weeks, and the same dosage is repeated for another 2 weeks. The dosage is reduced to 5 mg and prescribed for alternate-day for 2 weeks. The patient eventually quit prednisone as he was afraid of side effects which might include temporary atrophy and telangiectasia.
Additionally, topical minoxidil (5% solution) is also prescribed to the patient as an effort to accelerate hair regeneration and prevent further hair loss progression. Patient is advised to apply it 2-3 times a day A supplement of Vitamin C was prescribed for 3 months for the daily consumption of 1000mg to boost the patient’s hair growth.
Result
To better supervise the outcome, the patient is asked to return for a follow up after every week. A photograph of the scalp is taken during each visit to record the progress. The successful outcome of the treatment is evidenced by the restoration of the hair growth over the period of 3 months.
The hair growth did not become noticeable in the first 4 weeks. The first Triamcinolone injection treatment starts on 3 October 2021 (Figure 2). As can be seen in Figure 3, there is not much change observable. At this stage, the patient starts to take Prednisone orally. However, the result drastically happens after the third injection (Figure 4). The hair starts growing, initially concentrated in a random pattern (Figure 5), and after 2 weeks, the base of the hair growth starts to gradually spread across the bald spot (Figure 6). In his final visit, the hair has fully accumulated and covered the previously bald spot (Figure 7). With this, the treatment concluded as the hair has shown a normal growth and completely covered the patchy area.
We called the patient in the following month to ask about his condition, if there’s anything unusual with his hair growth and whether or not there needs to be another follow up session but he gave a positive feedback saying his hair has been growing well since our his last visit and that he could barely tell the which part of his scalp was bald as the newly hair grown is properly blended with other hair.






Conclusion
Although Alopecia Areata does not present harm, it definitely affects an individual suffering from it greatly especially in a social and emotional context. The best that can be done is for experts in the field of hair restoration to raise awareness and educate the general public about the availability of its treatment. As seen in this case of a man suffering from AA, the whole treatment took less than 6 months and this is owing to the fact that his condition is addressed at its early stage. For some individuals who may contemplate whether a treatment for AA is worthy or not, this study should serve as an example of how painless and easy the treatment is, as well as proving its reliability so an AA patient can make a smart and quick decision.
References
-
Bajaj D, Devrajani B, Shah Z, Ghauri R, Matlani B (2008) Treatment of extensive alopecia areata with oral prednisolone mini-pulse regimen. Journal of Pakistan Association of Dermatologists 18(4).
-
Barletta M, Gasques L (2020) Successful treatment of alopecia areata patches with triamcinolone acetonide using MMP®: Report of 2 cases. Skin Appendage Disorders 6(4): 229-234.
-
Darwin E, Hirt PA, Fertig R, Doliner B, Delcanto G, et al. (2018) Alopecia Areata: Review of Epidemiology, Clinical Features, Pathogenesis, and New Treatment Options. Int J Trichology 10(2): 51-60.
-
Fernando T, Goldman RD (2020) Corticosteroids for alopecia areata in children. Canadian family physician Medecin de famille canadien 66(7): 499-501.
-
Fenton DA, Wilkinson JD (1983) Topical minoxidil in the treatment of alopecia areata. BMJ 287(6398): 1015- 1017.
-
Kumaresan M (2010) Intralesional steroids for alopecia areata. International Journal of Trichology 2(1): 63.
-
Seetharam KA (2013) Alopecia areata: An update. Indian Journal of Dermatology, Venereology, and Leprology 79(5): 563.
-
Trüeb RM, Dias MF (2017) Alopecia areata: A comprehensive review of pathogenesis and management. Clinical Reviews in Allergy & Immunology 54(1): 68-87.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling