Diagnosis and Expert Examination of Neoplasms of the Skin in Servicemen of the Armed Forces of Ukraine
Among the adult population in many countries, the military is at risk for developing malignant skin tumors which are associated with many risk factors including ultraviolet light. It is noteworthy that there are no clear criteria for the diagnosis of precancerous and tumorous skin diseases as well as the lack of recommendations for risk groups among servicemen and the diagnosis of malignancy of skin tumors among servicemen of the Armed Forces. A review of modern classifications of skin neoplasms and methods of early diagnosis of them, taking into account the prospects of early detection of melanoma and medical examination has been carried out. The early modern diagnosis of melanoma is emphasized to be associated with higher patient survival. Visual diagnosis must be supplemented by a dermoscopic examination and consultation with a dermatologist. There is a need within the military medicine of Ukraine to develop an algorithm for examining the patient and further examination in case of the presence of skin tumors. Multiple dysplastic nevi remain a complex diagnostic and treatment problem in modern dermatology. An important issue is the examination of the suitability for military service in case of the presence of multiple nevi.
Case Report
Multiple nevi (MN) remain a significant clinical problem in dermatological practice; the issue of their early diagnosis and subsequent management regarding the prognosis for health, performance of the patient’s duties especially with an intensive work regime, is essentially relevant [1]. In this context, the interpretation of the diagnosis and examination of MN in military personnel who are under conditions of increased stress and who have an increased risk of further transformation into a malignant neoplasm of the skin (melanoma) is becoming more urgent [2]. According to the literature data [3], MN are supposed to be a manifestation of the syndrome of dysplastic nevi and the risk of their malignant transformation is significant which suggests further observation of such patients by a dermatologist.
A case of MN diagnosis in a serviceman of the Armed Forces of Ukraine with subsequent exclusion of melanoma is being presented.
A patient J., born in 1997 who is a sub lieutenant of military service in the Armed Forces of Ukraine, was conscripted for military service in June 2020 being healthy according to the medical committee evidence (including a dermatologist one). During the subsequent medical examination in January 2021, the patient was diagnosed with MN during a dermatological examination. Consequently, an in-depth clinical and laboratory examinations were carried out. It was found that the patient had noted the presence of a large number of nevi since childhood and was consulted by a dermatologist and cosmetologist in 2006. Moreover, 2 melanocytic nevi were removed on his back. The examination of these sites revealed 2 scars with recurrent nevi (Figure 1). Also, when examining the skin of the trunk and extremities, more than 100 melanocytic nevi were detected (Figure 2), which made it possible to verify the diagnosis of MN - a syndrome of dysplastic nevi.
Dermatological status of the patient: multiple pigment spots, plaques and papules from 3-4 mm to 1.3 cm in diameter, without visible signs of inflammation, irritation or injury are observed on the skin of the scalp, face, trunk, upper and lower extremities (5 nevi on the buttocks). An ugly duckling sign was detected on the skin of the left axillary region (Figure 3).



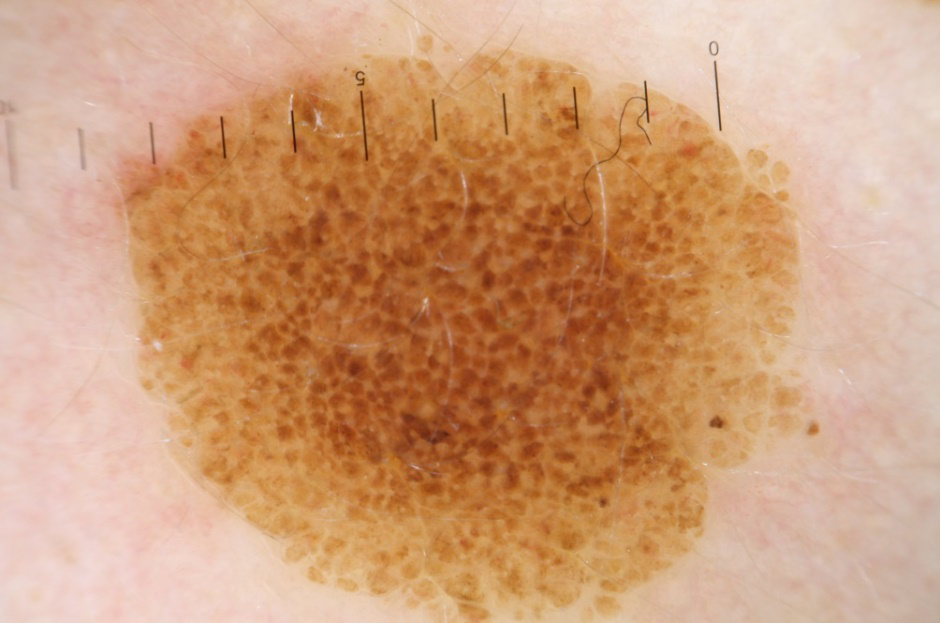
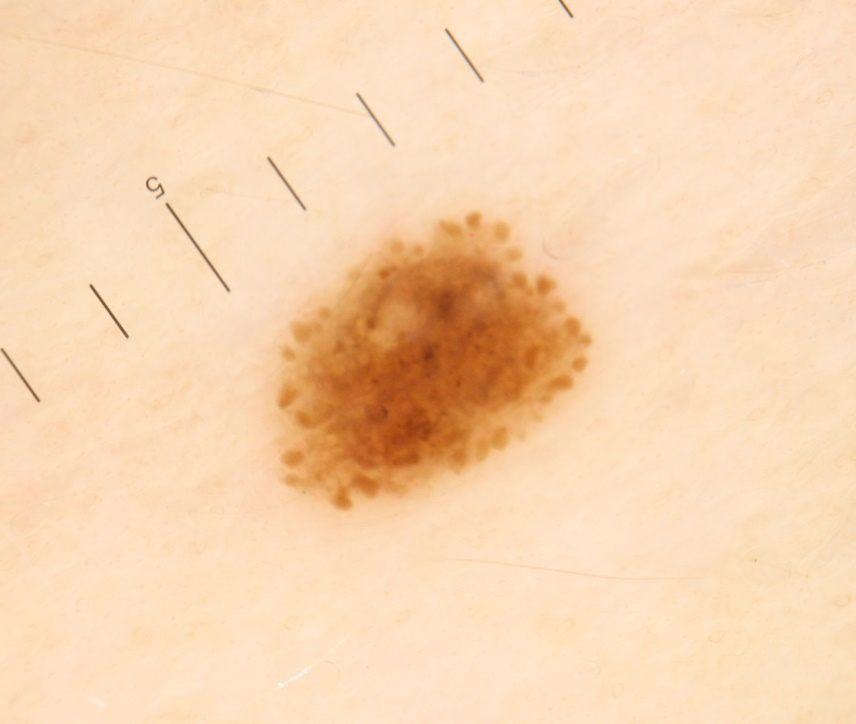
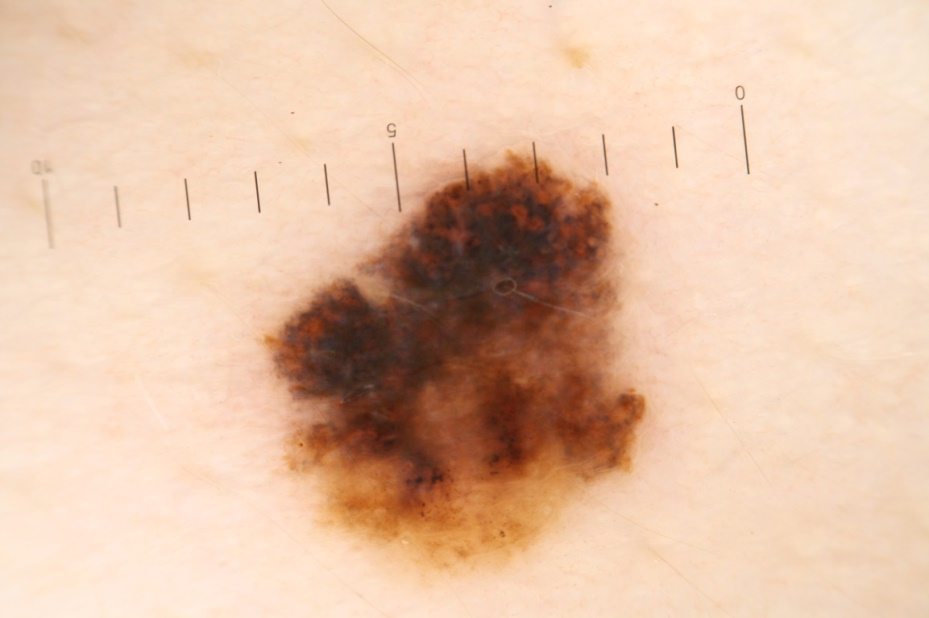
Dermoscopy suggested the following results (Table 1). Dermoscopic status: on the skin of the scalp, face, trunk, upper and lower extremities (5 formations on the buttocks) there are multiple melanocytic spots and plaques, both symmetrical and asymmetrical in shape and structure (with a papular element in the center of the spot) from 3 -4 mm to 1.3 cm in diameter, which are dermoscopically represented by typical globular and homogeneous patterns which are observed occasionally with elements of the reticular pigment network, light and light brown in colour. A symptom of fried- egg pattern is also often viewed (Figure 4). Dermoscopy index - 2.5. The dermoscopic image is consistent with simple melanocytic nevi and atypical Clark nevi. On the skin of the lumbar region on the left there is a symmetrical in shape and structure melanocytic spot, 3 mm in diameter, light brown in colour which is dermoscopically represented by a typical reticular pattern (Figure 5) with typical globules along the periphery of the formation (Figure 6). Dermoscopic index -1.5, dermoscopic image corresponds to either melanocytic formation in the growth phase or Spitz-nevus. On the skin of the left axillary region, an asymmetric melanocytic spot of 7 mm in diameter, with asymmetric distribution of black, dark brown and light brown colours, with elements of an atypical pigment network, atypical black spots and signs of white - blue veil is observed. Dermoscopic index – 6.1. Suspitio melanoma. Dermoscopic diagnosis was formulated as follows: Multiple melanocytic nevi of the head, neck, trunk, upper and lower extremities. Syndrome of dysplastic nevi. Suspitio melanoma and Spitz-nevus.

As a result of a comprehensive examination the following diagnosis was formed: Multiple melanocytic nevi of the head, neck, trunk, upper and lower extremities. Syndrome of dysplastic nevi. Suspicion of melanoma degeneration of a nevus?
Since the examination also revealed the formation of the skin with suspected melanoma degeneration - the ugly duckling sign, there was a direct need for further diagnostics. We performed the removal of this neoplasm with subsequent histological examination.
| Skin phototype | ІІ-ІІІ | ||
|---|---|---|---|
| A number of nevi | 148 | ||
| up to 0.6 cm | 128 | ||
| up to 1.0 | 17 | ||
| More than 1 cm | 3 | ||
| More than 2 mm on the arms (out of the total) | 38 | ||
| Criterion | Description | Points | Value |
| Asymmetry | On the vertical axis | 1 | |
| On the horizontal axis | 1 | 2.6 | |
| Borders | 12:30-13:30 | 0 | |
| 13:30-15:00 | |||
| 15:00-16:30 | |||
| 16:30-18:00 | |||
| 18:00-19:30 | |||
| 19:30-21:00 | |||
| 21:00-22:30 | |||
| 22:30-00:00 | |||
| Colour | White | 1,5 | |
| Red | |||
| Light brown (beige) | 1 | ||
| Brown (dark brown) | 1 | ||
| Blue grey | |||
| Black | 1 | ||
| Dermascopic structures | Pigment net | 1 | 2 |
| Unstructured zone | 1 | ||
| Stripes | |||
| Globules, granules | 1 | ||
| Black and brown spots | 1 | ||
| General dermatological index | 6,1 |
Table 1: Dermascopic diagnostic conclusion of the patient G.
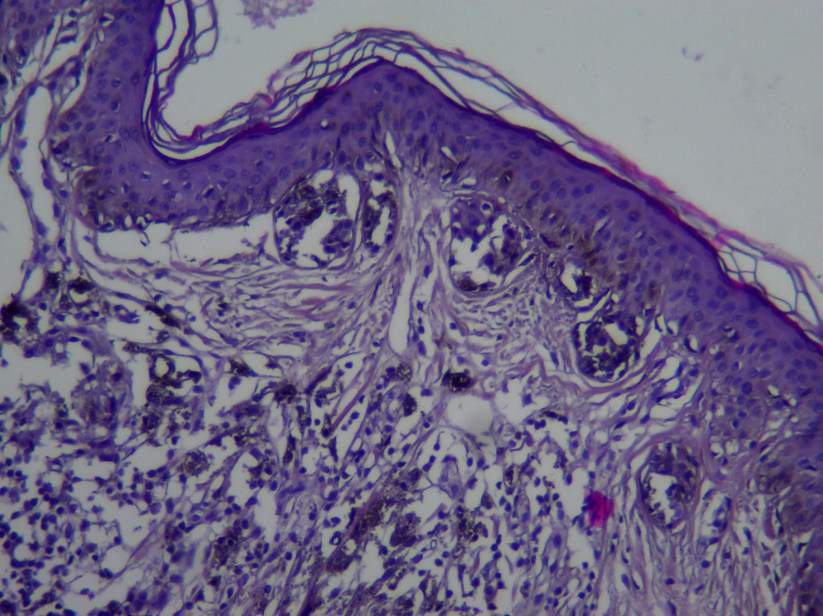
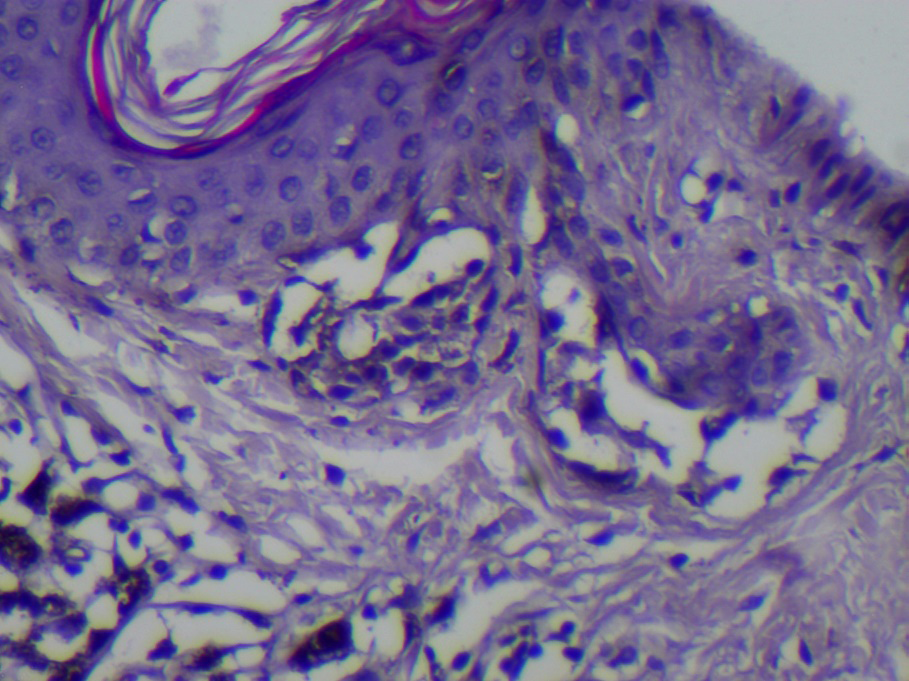
The result of a histological examination (22.02.2021): a fragment of the skin with the presence of a melanocytic dysplastic nevus with mild cytological atypia represented by an accumulation of nevoid cells with oval nuclei (Figure 8), an optically empty corolla of the cytoplasm, as well as groups of nevus cells with small rounded or oval nuclei and a rim of eosinophilic cytoplasm located predominantly in the dermis and intraepithelially. The size of the nuclei of the nevus cells does not exceed the size of keratinocytes and is with moderate hyperchromasia. Visible nucleoli are not observed.
Mitotic activity is unexpressed, atypical mitoses are absent. Intraepithelial complexes of tumor cells are located closer to the epidermal junction, single cells in the spinous layer of the epidermis predominantly with light cytoplasm. A diffuse insignificant mononuclear infiltration is noted in the place of a large accumulation of nevus cells, which were located in the dermis and contain in the cytoplasm brown colored pigment grains of various sizes. The acanthotic processes of the epidermis contain round or oval-shaped clusters of nevus cells with a light cytoplasm of the type reminding a swallow nest. In the superficial layers of the dermis, tumor cells are located in most alveolar groups from 4 to tens of cells (Figure 9). The fibers of the connective tissue of the dermis are parallel to each other and go around groups of nevus cells. In the area of the tumor location, a developed network of small-caliber blood vessels is observed with the preservation of the endothelial lining.
The obtained results of histological examination allowed us to confirm the diagnosis of multiple nevi and exclude the presence of a melanoma neoplasm. Since in this case an examination of a serviceman was carried out, further recommendations were given as follows. The patient was not fit to continue military service. To rule out subsequent malignant transformation, it is recommended to see a dermatologist oncologist for a dermoscopy examination once a year, avoid sun exposure and use sunscreen with SPF factor, which is a generally accepted recommendation in such cases [5].
The case presented by us is an example of the importance of timely diagnosis of multiple nevus syndrome with subsequent medical examination of the patient, taking into account the characteristics and risks of this condition, employment opportunities and military service. To do this, it is necessary to form clear diagnostic criteria based on reproducible research methods available under standard conditions. Dermoscopy in this case is the main diagnostic method and biopsy is especially important to clarify the nature of the process.
References
-
Damsky WE, Bosenberg M (2017) Melanocytic nevi and melanoma: unraveling a complex relationship. Oncogene 36(42): 5771-5792.
-
Cengiz FP. Emiroglu N, Bahali AG, Ozlem Su, Onsun N (2017) Malignant melanoma arising in congenital melanocytic nevi: clinical and dermoscopic challenges. Our Dermatol Online 8(1): 34-36.
-
Rosendahl CO, Grant-Kels JM, Que SKT (2015) Dysplastic nevus: fact and fiction. Journal of the American Academy of Dermatology 73(3): 507-512.
-
Wall N, De’Ambrosis B, Muir J (2017) The management of dysplastic naevi: a survey of Australian dermatologists. Australas J Dermatol 58(4): 304-307.
-
Tschandl P (2018) Sequential digital dermatoscopic imaging of patients with multiple atypical nevi. Dermatol Pract Concept 8(3): 231-237.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling