Primary Cutaneous CD30+ Type Pleomorphic Immunoblastic Cell Lymphoma
Primary cutaneous large cell lymphoma CD30 + (CD30 + LCL) is a rare subtype of cutaneous T-cell lymphoma (CTCL) that often regresses spontaneously. The large-cell pleomorphic immunoblastic histological subtype does not adversely affect prognosis. It is important to distinguish CD30 + primary cutaneous large cell lymphoma from lymph node primary CD30 + lymphoma with secondary skin involvement, because in the latter case the prognosis is worse. The Authors report the case of a patient who presented an irregularly ovoid, figured and ulcerated plaque at the level of the left flank with contiguous ulcerated papules / nodules of smaller dimensions.
Introduction
Primary cutaneous large cell lymphoma CD30 + (CD30 + LCL) is a rare subtype of cutaneous T-cell lymphoma (CTCL) that tends to regress spontaneously. It can present in many ways but most commonly appears as a single or multiple lump that is occasionally ulcerated and localized to the trunk or limbs [1, 2, 3, 4]. A European multicenter study of 47 patients, however, demonstrated that the histological subtype of CLL (anaplastic or non-anaplastic, immunoblastic and large-cell pleomorphic) did not influence prognosis. Based on this study, the authors recommend that the term “anaplastic” be omitted from the nomenclature [1, 4]. It is essential to distinguish CD30 + primary cutaneous large cell lymphoma from primary CD30 + nodal lymphoma with secondary skin involvement, because in the latter case the prognosis is worse and therefore more aggressive treatment is required and there are no differences in clinical presentation. , the course and prognosis between anaplastic and non-anaplastic [4].
The Authors report the case of a patient who presented an irregularly ovoid, figured and ulcerated plaque at the level of the left flank with contiguous ulcerated papules / nodules of smaller dimensions.
Our observation CG male of age 62 for the presence of an irregularly ovoid, figured, asymmetrical plaque, 3.5 cm in diameter along the major axis, of a rosy red color, ulcerated, with irregular polycyclic and raised margins dark red color and lighter, atrophic central area. Adjacent to it there were 5 similar but smaller satellite papules / nodules. On palpation, the lesion was infiltrated mainly at the edges (Figure 1).
This clinical objectivity, localized at the level of the left flank, had appeared about 2-3 months earlier, was associated with intense itching and had undergone gradual centrifugal extension. In the remote pathological history there were tonsillectomy and left varicocele surgeries. Routine blood tests were normal except for an increase in cholesterol and triglycerides.
Equally negative or normal were ESR, CRP, Rheumatoid Factor, Hepatitis B and C markers, b2 microglobulin, pANCA and cANCA, ANA, ENA, Anti DNA and ACE.
A chest x-ray was negative and the ultrasound of the abdomen showed an enlarged liver with steatotic echo structure and gallbladder stones. The ultrasound of the superficial lymph node stations was negative for suspected lymphadenopathies with evidence of reactive lymph nodes with a maximum diameter of 2 cm in the ingunal and submandibular sites bilaterally.
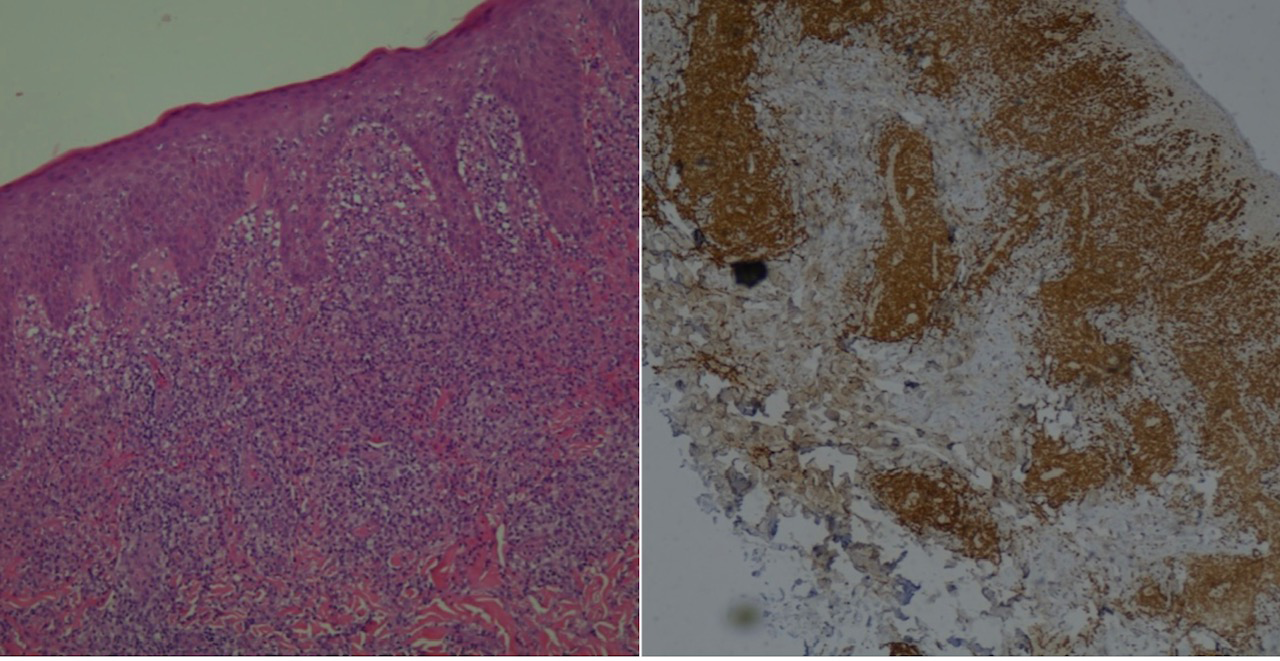
A skin biopsy was therefore carried out, the histological examination of which revealed an infiltration, in the superficial and deep dermis, of aggregates of large, pleomorphic, predominantly immunoblastic (non-anaplastic) lymphoid cells. Associated reactive cell component consisting of small T lymphocytes, histiocytes and rare eosinophilic granulocytes.
Immunohistochemical investigations gave results: CD3 + (diffuse and intense), CD4 + (weak), CD30 + (greater than 75%), Bcl6-. High proliferative activity (Ki67> 50%) (Figure 2).
A diagnosis of CD30 + T lymphoma of the skin, an immunoblastic pleomorphic cell variant was therefore made.
We therefore performed a Total body + skull CT which was negative and we therefore opted for a radiotherapy treatment that the patient performed with external beams at the cumulative dose of 3000 cGy and fractionation 200cGy / day lasting 15 days (Figure 3).


Discussion
Cutaneous T-cell lymphomas (CTCL) include various types of malignancies: mycosis fungoides (MF), Sézary syndrome, lymphomatoid papulosis (LyP), and anaplastic large cell lymphoma (LCL). considered together in order to establish the specific subtype in order to ensure the most appropriate treatment [2, 4]. Primary cutaneous CD30 + lymphoma accounts for approximately 10 percent of all CTCL cases [2]. Diagnosis is based on the following criteria: (a) the predominance (greater than 75%) of large CD30 + immunoblast cells; (b) no clinical evidence of previous or concomitant LyP, MF or other cutaneous lymphoma and (c) absence of extracutaneous lymphoglandular or systemic localization [4].
It most commonly affects men between the ages of 45 and 60 and clinically tends to appear as a solitary lump, often with ulceration, although in 20% of cases it can be multifocal at presentation. Lesions generally grow rapidly and are more frequently localized to the trunk and extremities [1, 2]. A study of 47 patients with CD30 + primary cutaneous lymphoma conducted by Beljaards, et al. showed that all 47 patients had lesions on the trunk, face, arms or legs [4]. Histology typically reveals the presence of clusters of large CD30 + cells, infiltrated by inflammatory cells are often found in the periphery [1, 3].
Of great importance in the diagnosis is to determine the CD30 positivity.
Previous studies have shown that CD30 negative lymphoma has a worse prognosis than CD30+ [4] and must be treated more aggressively. The morphological subtype of LCL (i.e., anaplastic vs non-anaplastic types, between immunoblastic and large pleomorphs) does not affect prognosis. [1, 4]. There is a continuum of CD30 + pictures, from malignant large cell CD30 + lymphoma to benign lymphomatoid papulosis (LyP). The tendency of CD30+ malignant large cell lymphoma to spontaneously regress in about 25% of cases suggests that this condition may be related to LyP, an indolent type of CTCL characterized by recurrent papulonodular lesions that usually regress spontaneously. LyP histopathology reveals numerous inflammatory cells with few CD30 + cells (less than 25%) [2, 3].
Primary CD30 + cutaneous lymphoma is also histologically similar to the anaplastic CD30 + lymph node form, therefore it should be noted if there is lymph node involvement or involvement beyond a regional lymph node [3].
In contrast to primary cutaneous lymphoma which can remain localized to the skin for prolonged periods of time, the systemic / lymph node form is an aggressive disease with rapid spread to other organs, including the skin. There may be different therapeutic options for primary cutaneous CD30 + LCL depending on the extent of the disease. Local radiotherapy and surgical excision are effective with limited disease as in our case, while systemic chemotherapy should be reserved for patients with generalized disease or systemic LCL progression [1, 2]. Patients with solitary or localized lesions may require no treatment as spontaneous regression can occur in up to 42 percent of CD30 + LCL.
References
-
Freitas IC, Vieira R, Afonso A, Pacheco A, Nunes P (2000) Primary cutaneous CD30-positive large cell lymphoma. J Eur Acad Dermatol Venereol 14(1): 51-53.
-
Parlette EC, Tabor CA (2006) CD30+, large T-cell lymphoma: diagnostic distinction and management. Dermatol Online J 12(6): 8.
-
Lan CC, Yu HS, Cheng ST, Chen GS (2003) Relapsing ulcerative papules over bilateral hands and scrotum in an Asian man: an atypical manifestation of primary cutaneous CD30-positive lymphoma. J Dermatol 30(3): 230-235.
-
Beljaards RC, Kaudewitz P, Berti E, Gianotti R, Neumann C, et al. (1993) Primary cutaneous CD30-positive large cell lymphoma: definition of a new type of cutaneous lymphoma with a favorable prognosis. A European Multicenter Study of 47 patients. Cancer 71(6): 2097- 2104.
-
Beljaards RC, Kaudewitz P, Berti E (1993) Primary cutaneous CD30-positive large cell lymphoma: definition of a new type of cutaneous lymphoma with a favorable prognosis: a European multicenter study of 47 patients. Cancer 71(6): 2097-2104.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling