Observation on the Effect of Dermoscopy for Long-pulsed 1064nm Nd: YAG Laser in the Treatment of Onychomycosis
Purpose: To explore the effect of dermoscopy using a long-pulsed 1064-nm Nd: YAG laser in the treatment of onychomycosis. Methods: Eight patients with onychomycosis (a total of 55 diseased nails) were enrolled in the study and treated every week for a total of 12-16 sessions using a long pulsed 1064-nm Nd: YAG laser. In each session, diseased nails were irradiated for three times, with a 1 minute pause between each passage. Dermoscopic images were obtained using a special lens. Results: Thirteen of the diseased nails were cured. Twenty-four and 14 diseased nails showed excellent and good results, respectively with a significant reduction in white longitudinal stripes, jagged proximal edge, onycholysis, and opacity. However, the treatment was ineffective in four diseased nails. Conclusions: Long-pulsed 1064-nm Nd: YAG laser may be an alternative option for the treatment of mild onychomycosis. Dermoscopy is of great significance in improving the clinical diagnosis and evaluation of onychomycosis.
Introduction
Onychomycosis is the most common nail disease, accounting for approximately 20% of all fingernail and toenail diseases [1]. The diagnosis of onychomycosis mainly relies on clinical manifestations, potassium hydroxide (KOH) examination, and mycotic culture of specimens. Nonetheless, due to their low sensitivity, mycological examinations depend on fungal laboratory equipment and experienced mycological examination experts. Histopathology has disadvantages, such as trauma, pain, time consumption, and high cost, which limit their clinical application. Recently, dermatoscopy has been gradually applied in clinical treatment of onychomycosis, which has important value in improving its clinical diagnosis and evaluation. Specific dermoscopic patterns suggestive of onychomycosis have been identified, including chromonychia, onycholysis, opacity, longitudinal striae, and jagged edge with spikes [2, 3, 4].
Topical antifungal agents have difficulty penetrating the nail plate and exerting a bactericidal effect. Additionally, oral antifungal agents are not suitable for certain populations, such as patients with liver disease and the elderly. Therefore, a variety of non-pharmacological treatments have been attempted using an electric nail grinder, photodynamic therapy, or several laser devices [5, 6]. Among these, the use of a long-pulsed 1064-nm Nd: YAG laser has demonstrated promising results and has been approved by the Food and Drug Administration [7]. However, Hollmig, et al. suggested that a long-pulsed 1064 nm Nd: YAG laser may be ineffective for the treatment of onychomycosis [8]. Herein, we evaluated the safety and efficacy of the 1064 nm long-pulsed Nd: YAG laser in the treatment of onychomycosis.
Materials and Methods
Study Patients
Between March 2019 and July 2019, eight patients were consecutively recruited from our institution. Among the eight patients, four were female and four were male with a mean age of 45.5 years (range, 25 – 56 years). This study excluded patients with concomitant nail disorders (psoriasis, atopic dermatitis, lichen planus, etc.) and those who used oral or topical antifungal agents for 6 months. The diagnosis of each patient was based on clinical findings, dermoscopic images, KOH test results, and fungal cultures.
Treatment Methods
The Elite laser treatment instrument (Cynosure, USA) had a wavelength of 1064 nm, and the technical parameters were as follows: pulse width 30 – 40 ms, fluence 50 J/cm2, spot size 3 mm, frequency 1.5 Hz. Onychomycosis was treated using the aforementioned laser equipment and parameters. The spot was approximately 1 cm away from the diseased nail, and the diseased nail was irradiated vertically and uniformly. The treatment range was determined by dermoscopic inspection of the nail infection area. The laser irradiation exceeded the border of the nail infection area by approximately 3 mm (1 spot) and at least three consecutive irradiations each time, with the patient’s mild pain as the degree. Each diseased nail can be irradiated five to six times with an interval of approximately 5 – 10 seconds, according to the patient’s pain tolerance, to achieve a therapeutic effect.
Air cooling was not permitted, to avoid a local temperature drop during treatment. Treatment was conducted once a week, four times as a course of treatment, three consecutive courses of nail treatment, totaling 12 times; four consecutive courses of toenail treatment, totaling 16 times. In all cases, clinical and dermoscopic images were collected before each treatment and 6 months after completion. Dermoscopy (Nanjing Beining Dermoscopy Workstation, China, Software V1.0) was used to obtain dermoscopic images.
Results
Eight patients (four women and four men; median age: 45.5 years) completed the treatment and follow-up. Among them, 47 cases were distal and lateral onychomycosis (DLSO), four cases were endonychomycosis and four cases were total dystrophic onychomycosis, totaling 55 cases of diseased nails. The overall effective rate was 92.7%, and 13 (23.6%) of the diseased nails were cured. After treatment, opacity and onycholysis were significantly reduced in thirty-six (65.5%) cases, showing excellent results (Figure 1); 15 (27.3%) of the nails obtained good results, with reduced white longitudinal stripes, jagged proximal edge, onycholysis, and opacity. Treatment was ineffective for only four (7.3%) of the diseased nails (Figure 2). After the 6-month follow-up visit, the main complaint was mild pain during treatment, which was tolerable. All eight patients insisted on treatment and did not withdraw because of pain. There was one case of subungual hemorrhage of the thumbnail, which was absorbed by itself. No other obvious adverse reactions were found.

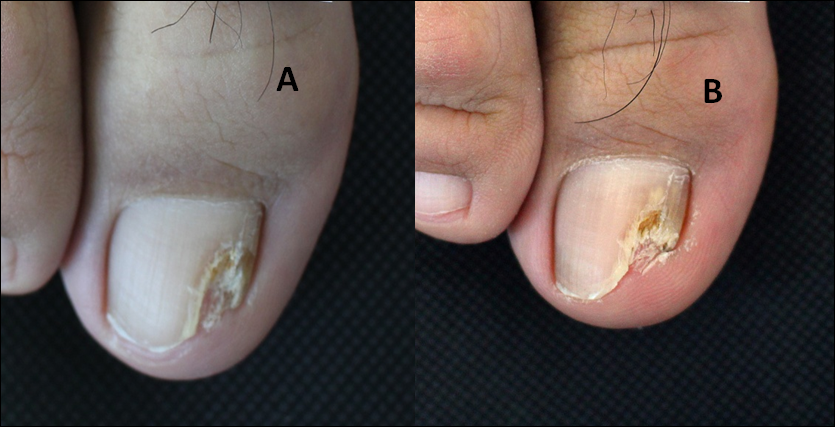

(A) (B) Figure 3: (A) Images captured with an ordinary camera;(B) Images captured using dermoscopy.
Discussion
Onychomycosis is caused by fungus invading the nail plate and subungual tissues. It is a common nail disorder in adults, with an incidence 13% [9]. Current routine treatment for onychomycosis includes systemic and topical antifungal drugs. Systemic antifungal treatments include itraconazole and terbinafine, which are recommended as first-line therapies owing to their high efficacy [10]. However, there are certain adverse reactions or cross-drug reactions with other drugs, which are not conducive to certain populations, such as children and the elderly.
In recent years, researchers have been trying to replace drug therapy with laser treatments to improve the cure rate, reduce the occurrence of adverse reactions, benefit patients with liver and kidney dysfunction, and avoid drug-resistant pathogens [11]. Most professional lasers are long-pulsed Nd: YAG 1064 nm lasers. Many studies have shown that laser treatment of onychomycosis is safe and effective [12]. More statistics are needed regarding the long-term efficacy and safety of this approach given the current study’s conflicting results.
Basic experiments have shown that long-pulsed Nd: YAG lasers can significantly kill Candida albicans and effectively inhibit the formation of Trichophyton rubrum colonies, leading to the destruction of its ultrastructure [13]. The direct thermal killing effect on fungal mycelia can be guaranteed when the treatment temperature exceeds 50°C [14]. In this experiment, to achieve a local high temperature, the laser treatment did not use air coolers to cool down, and experimental observations showed that the long-pulse 1064 nm Nd YAG laser instantly increased the temperature of the infected nail to 43–50°C, resulting in strong localization. The thermal effect can effectively inhibit and slow down the proliferation of fungi. This study found that laser treatment had a better effect on milder onychomycosis; however, the treatment of four of the diseased nails was ineffective. These four nails were thick and severely diseased; thus, treatment failure may be related to the thickness of the diseased nails. The thicker the diseased nails, the less penetration there was, the antibacterial effect was significantly weakened, and the recovery of the diseased nail was poor. It may be necessary to further increase the course of treatment or incorporate other treatment methods, such as local treatment to facilitate laser penetration and external antifungal drugs to reduce the rate of fungal invasion of the nail, and even incorporate with systemic antifungal drugs to improve efficacy.
Recently, dermoscopy has gradually been used in clinical treatment for nail disorders,which is of great value in improving the clinical diagnosis and evaluation of onychomycosis. Kaynak, et al. assessed 97 patients (205 diseased nails) with onychomycosis clinically diagnosed as the research object, of which 56 nails with negative fungal culture and/or histopathology (PAS and HE) results were the control group, and the other 149 patients with positive results were the case group. The results showed statistically significant differences in ruin-like appearance, homogeneous white nails, punctate white nails, and black changes between the two groups [15]. Gagged edges with spikes, longitudinal stripes, and chromonychia are the three most commonly used dermoscopic features in DLSO. The sensitivity/specificity of diagnosis could reach 100%/100%, 82.5%~86.5%/100%, and 95%/83.3%, respectively. Other commonly used features include remote irregular terminals [16] and ruin- like appearance [4]. It has been suggested that mycological examination is not necessary to rule out onychomycosis when the nail process is not seen under dermoscopy [17].
Photographs and dermoscopy were performed before each treatment. Compared with ordinary images, dermoscopy can observe changes that are invisible to the naked eye through high magnification of the local area, thus avoiding missed diagnoses (Figure 3). The false-negative rate of microbiological examination and culture can be reduced by precise localization of the sampling site through dermoscopic features of onychomycosis. Dermoscopy is non-invasive and quick, allowing continuous and dynamic observation of changes in the diseased nails. Continuous observation of the color change of the diseased nail and typical manifestations of onychomycosis through dermoscopy showed that when treating severe nail disease, when the diseased nail grows approximately 3 mm, there are still 2 mm new nails in the post-onychomycosis infection. The discoloration state indicated that the fungi of the diseased nails still had a faster multiplication rate, but the growth rate of the new nails was faster than the infection rate. Despite the advantages of dermoscopy, microbiological tests are still needed to make an accurate and reliable diagnosis.
Conclusion
This study confirmed that the long-pulse width 1064 nm Nd: YAG laser is more effective in treating milder onychomycosis, and no obvious adverse reactions were found in patients with normal liver and kidney function. It is a treatment plan worth promoting, owing to simple post- treatment care and high patient compliance. Dermoscopy is an easy, inexpensive, rapid, and simple technique for improving clinical diagnosis and evaluation of onychomycosis. In addition to microbiological testing, Dermoscopy can also be used as the first step in the diagnosis and evaluation of onychomycosis.
Fund program: (Z191100006619053) and (19QNP027)
Approval Opinions
The ethics committee discussed the relevant content of the program, “clinical application of long pulse laser in the treatment of onychomycosis”, and agreed that the research methods involving human ethics are in line with the Declaration of Helsinki and the World Health Organization’s Biomedical Research involving Humans International Code of Ethics. The research can be carried out.
References
-
Gupta AK,Uro M, Cooper EA (2010) Onychomycosis therapy: past, present, future. J Drugs Dermatol 9(9): 1109-1113.
-
Nakamura RC, Costa MC (2012) Dermatoscopic findings in the most frequent onychopathies: descriptive analysis of 500 cases. Int J Dermatol 51: 483-485.
-
Nada EEA, EI Taieb MA, EI-Feky MA, Ibrahim HM, Hegazy EM, et al. (2020) Diagnosis of onychomycosis clinically by nail dermoscopy versus microbiological diagnosis. Arch Dermatol Res 312(3): 207-212.
-
Ramos Pinheiro R, Dias Domingues T, Sousa V, Sousa V, Galhardas C, et al. (2019) A comparative study of onychomycosis and traumatic toenail onychodystrophy dermoscopic patterns. J Eur Acad Dermatol Venereol 33(4): 786-792.
-
Kim YJ, K im BJ, K im MN (2008) The efficacy of electric nail grinding with nail lacquer in the treatment of onychomycosis. Korean J Dermatol 46(1): 77-82.
-
Aspiroz C, F ortuñ o Cebamanos B, Rezusta A, Paz- Cristóbal P, Domínguez-Luzón F, et al. (2011) Photodynamic therapy for onychomycosis. case report and review of the literature. Rev Iberoam Micol 28(4): 191-193.
-
Moon SH, Hur H, Oh YJ, Choi KH, Kim JE, et al. (2014) Treatment of onychomycosis with a 1064-nm long- pulsed Nd:YAG laser. J Cosmet Laser Ther 16(4): 165- 170.
-
Hollmig ST, Rahman Z, Henderson MT, Rotatori RM, Gladstone H, et al. (2014) Lack of efficacy with 1064nm neodymium:yttriumaluminumgarnet laser for the treatment of onychomycosis: A randomized, controlled trial. J Am Acad Dermatol 70: 911-917.
-
Amichai B, Davidovici B, Trau H, Lyakhovitsky A, Grunwald MH, et al. (2011) A rationale for systemic treatment in onychomycosis with negrative results on fungal examination. Clinical and experiment dermatology 36: 724-727.
-
Lipner SR, Scher RK (2019) Onychomycosis: Treatment and prevention of recurrence. J Am Acad Dermatol 80(4): 853-867.
-
Gupta AK, Paquet M (2015) Management of onychomycosis in Canada in 2014. J Cutan Med Surg 19(3): 260-273.
-
Helou J, Maatouk I, Hajjar MA (2016) Evaluation of Nd:YAG laser device efficacy on onychomycosis: A case series of 30 patients. Mycoses 59(1): 7-11.
-
Xu ZL,Xu J,Zhuo FL,Wang L, Xu W, et al. (2012) Effects of laser irradiation on Trichophyton rubrum growth and ultrastructure. Chin Med J 125(20): 3697- 3700.
-
Paasch U, Mock A, Grunewald S, Bodendorf MO, Kendler M, et al. (2013) Antifungal efficacy of lasers against dermatophytes and yeasts in vitro. Int J Hyperthermia 29(6): 544-550.
-
Kaynak E, Goktay F, Gunes P, Sayman E, Turan D, et al. (2018) The role of dermoscopy in the diagnosis of distal lateral subungual onychomycosis. Arch Dermatol Res 310(1): 57-69.
-
El-Hoshy KH, Abdel Hay RM, El-Sherif RH, Salah Eldin M, Moussa MF (2015) Nail dermoscopy is a helpful tool in the diagnosis of onychomycosis: A case control study. Eur J Dermatol 25(5): 494-495.
-
Jesus-Silva MA, Fernandez-Martinez R, Roldan-Marin R, Arenas R (2015) Dermoscopic patterns in patients with a clinical diagnosis of onychomycosis-results of a prospective study including data of potassium hydroxide (KOH) and culture examination. Dermatol Pract Concept 5(2): 39-44.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling