Vegetative Pemphigus - Challenge for Diagnosis and Treatment
Pemphigus is a group of potentially life-threatening autoimmune diseases characterized by the formation of skin and / or mucous membranes. Among the many types of pemphigus, the most rare clinical option is vegetative. It is often difficult to diagnose and clinically recognize this pathology because of the variety of expressions and the presence of verrucous formations. Therefore, the purpose of this work is to highlight the issues of the clinic, diagnosis and treatment of vegetative pemphigus (PV). The literature review and analysis of the results of clinical examination of a patient with PV were performed.The vegetative pemphigus accounts for 1 to 2% of all cases of pemphigus disease, and worldwide the incidence of vegetative vesicle is approximately 0.7 per 100,000. In most patients, the initial manifestations are stomatitis. From several weeks to months after the onset of mucous membranes, skin pustules and / or flaccid bullae are formed on unmodified skin, usually affecting the torso, arms, legs, and flexion areas. The skin formations are destroyed, eroded, form vegetations, covering with vegetative plaques the eroded surface characterized by abnormal growth of keratinocytes. These hyperkeratotic lesions are typically present in the intertriginous areas - including the groin / inguinal folds, armpits, hips, and flexion. The pathological process is based on the formation of IgG autoantibodies against desmoglins, one of the major cell adhesion proteins of the desmosome, causing loss of cell adhesion. This loss of adhesion leads to acantholysis. Histopathologically early lesions of pemphigus vulgaris and pemphigus vegetans demonstrate transbasal acantholysis. Pemphigus vegetans also exhibits epidermal hyperplasia, papillomatosis and intraepidermal eosinophilic abscesses according to the duration of the lesion. The diagnosis of a vegetative vesicle is made on the basis of clinical features, histological examination and detection of autoantibodies. The most widely used methods of detecting pemphigus autoantibodies include direct and indirect immunofluorescence, immunoprecipitation, immunoblotting, and enzyme-linked immunosorbent assay (ELISA). Treatment recommended by European and Japanese guides includes topical internal focal therapy, systemic therapy, wound care, and oral treatment features. This article presents a clinical case of a patient diagnosed with Vegetative Pemphigus. The severity and course of the disease is variable, but before the onset of steroids, most patients died. Treatment with systemic steroids reduced mortality rates. Morbidity and mortality are associated with the degree of disease, the maximum dose of prednisolone required to induce remission, and the presence of other diseases. The prognosis is worse for elderly patients and patients with comorbidities.
Introduction
The vegetative pemphigus accounts for 1 to 2% of all cases of pemphigus disease, and worldwide the incidence of vegetative vesicle is approximately 0.7 per 100,000. Given the limited number of cases, the epidemiology is thought to be similar to that of pemphigus vulgaris, which is more common in women, with the female to male ratio is 1.3 to 2.3 to 1. Age at diagnosis is typically 50 to 70 years in the US and European countries and 30 to 50 years in other countries [1]. Pemphigus (pemphigus) is a group of potentially life-threatening autoimmune diseases characterized by the formation of blisters on the skin and/ or mucous membranes. The word “pemphigus” comes from the Greek word “pemphix”, which translates as a blister, and describes a group of chronic bullous diseases, first named by Wichmann in 1791. The term pemphigus once included most bullous skin eruptions, but diagnostic tests have improved and bullous diseases have been reclassified. On the basis of clinical and histopathological characteristics, as well as on specific antigens against which autoantibodies are produced, different types of pemphigus were determined. They can be classified into the following forms: vulgar, foliar, vegetative and seborrheic. In recent decades, non-classical forms of pemphigus have also been described: paraneoplastic pemphigus and IgA pemphigus, herpetiform pemphigus, Brazilian type [2]. The most common type of pemphigus is vulgar pemphigus, characterized by mucocutaneous bullae. Among the many types of pemphigus, the rarest clinical variant is vegetative. It is very often difficult to diagnose and clinically recognize this pathology due to the variety of manifestations and the presence of verrucous formations. Therefore, the purpose of this work is to highlight the issues of the clinic, diagnosis and treatment of pemphigus vulgaris [3, 4, 5, 6].
Clinic
In most patients, the initial manifestations are represented by stomatitis. From several weeks to months after the appearance of mucous blisters, skin pustules and/ or flaccid bullae develop on intact skin, usually affecting the body, arms, legs, and flexor areas. Blisters are placed on the skin that is not changed externally, filled with serosus, transparent(clear) contents. They quickly open, turning into painful bright red erosions. Skin formations are destroyed, eroded, form vegetations, covering the eroded surface with vegetative plaques characterized by abnormal growth of keratinocytes. These hyperkeratotic lesions are characteristically present in the intertriginous regions - including the groin/inguinal folds, armpits, thighs, and flexor surface. Less commonly affected areas include the scalp, soles of the feet, and areas of skin grafts. There are also reports of damage to the nose, vagina and conjunctiva. In the oral cavity, hyperkeratotic plaques appear on the tongue, having a brain-like shape. Although most patients have an adequate physical examination, it is important to take a detailed medical history, including family and personal history of autoimmune diseases and skin problems. Other relevant details include stressors, history of radiation therapy, recent illness, medication changes, or if there is pain associated with activities such as eating, swallowing, sexual activity, or if clinical symptoms flare with menstruation [2, 7, 8, 9, 10].
Clinical Types
• Neumann’s type (Neumann) is more severe and resistant to treatment. It has characteristic large vesiculobullous, erosive lesions, flaccid blisters on intertriginous areas where vegetations develop. The mucous membrane of the oral cavity is often involved in the pathological process. This subtype is more common, with a clinical course parallel to pemphigus vulgaris. Patients require higher doses of systemic corticosteroids, have relapses and remissions.
• The Hallopeau type has a more benign course and typically exhibits initial pustular lesions that heal as vegetative plaques. The mucous membrane of the oral cavity is often not affected, has a more sluggish course. It can be repeated spontaneously. Patients require lower doses of systemic corticosteroids and usually have a prolonged remission [4].
Pathogenesis
The basis of the pathological process is the formation of IgG autoantibodies against desmogleins, one of the leading proteins of cell adhesion to desmosomes, which cause the loss of cell adhesion. This loss of adhesion leads to acantholysis (Acantholysis; Akanto- + Greek Lysis destruction, dissolution - a degenerative change in the spinоsus layer of the epidermis, which is manifested by the destruction of intercellular bridges, loss of cells, mostly cytoplasm and morphological changes in the nuclei; leads to the formation of blisters). As the epidermis grows the blisters burst, which leads to the formation of erosions on the skin and mucosa. Desmoglein-1 (Dsg-1) is present in all layers of the epidermis with higher concentrations in the more superficial layers, whereas desmoglein-3 (Dsg-3) is expressed in the parabasal and basal layers. In the mucosa, Dsg-1 and Dsg-3 are expressed in all layers of the epidermis, but the mucosa has lower concentrations of Dsg-1. Patients with mucocutaneous pemphigus have autoantibodies directed against Dsg-1 and Dsg-3, whereas patients with mucocutaneous pemphigus have antibodies directed only at Dsg-3. The cause of the trigger that leads to the formation of antibodies is unknown [9, 11, 12].
Histology
Histopathological examination helps to reveal the level of blistering in order to diagnose pemphigus and differentiate it from other subepidermal bullous lesions, since acantholytic keratinocytes can be observed in several vesiculobullous diseases (Haley-Haley disease, as Grover and Haley-Haley, others). For biopsy, it is recommended that a recent blister (less than 24 hours of appearance) placed inside a 4-mm punch or small excision be selected, as blisters are usually easily ruptured. If this is not possible, a biopsy of the area around the formation should be performed so that the blister cover adheres to the adjacent skin and does not peel off during histological processing. The biopsy should be fixed in 10% formalin (buffered formalin is better for preserving the surface antigen). Histopathological examination indicates the level of epidermal cleavage (suprabasal or intramalpygian). Histopathologically, early lesions of pemphigus vulgaris and pemphigus vegetative show suprabasal acantholysis. Pemphigus vegetative also reveals epidermal hyperplasia, papillomatosis, and intraepidermal eosinophilic abscesses according to the duration of the lesion. Histopathological changes in vegetative pemphigus are also different from the vulgar type by the eosinophilic reaction, the formation of microabscesses, and the degree of vesiculation. Acantholysis can affect the epithelia of the adjunct apparates (usually follicular epithelium), which facilitates the differential diagnosis with Hailey-Hailey disease [6, 13].
Diagnostics
Vegetative pemphigus is diagnosed on the basis of clinical features, histological examination and detection of autoantibodies. There are several methods of evaluation and identification of autoantibodies. The most widely used methods for detecting pemphigus autoantibodies include direct and indirect immunofluorescence, immunoprecipitation, immunoblotting, and enzyme-linked immunosorbent assay (ELISA) [14].
1. Characteristic clinical picture
2. Nikolsky’s symptom: On externally unchanged skin. When lightly rubbing healthy-looking skin with a finger near the blisters, and sometimes at a distance from them, peeling of the surface layers of the epithelium occurs with the formation of erosions.
3. Nikolsky’s marginal symptom: When pulling with tweezers for scraps of the blister cover, the epithelium peels off far beyond the erosion.
4. Asbe-Hansen’s symptom: When pressed, the blister causes an increase in its area. These 3 symptoms clinically represent acantholysis or loss of cell adhesion and are not specific for VP; they can be present in other forms of pemphigus and in toxic epidermal necrolysis.
5. Cytological method: (Ttsanka smear) is useful for the rapid demonstration of acantholytic keratinocytes of the spinosus layer (abundant eosinophilic cytoplasm and a rounded central nucleus), stained mainly with hematoxylin and eosin [15].
6. Histological examination • Immunoblotting or serum ELISA: Blood tests can identify patients with serum desmoglein 3 autoantibodies with a specificity and sensitivity of 98 to 100%, so almost all pemphigus patients will have desmoglein 3 reactivity.
• Direct immunofluorescence (DIF): Similar to pemphigus vulgaris, direct immunofluorescence in pemphigus vegetative demonstrates intercellular deposition of IgG and C3 in the intraepidermal space and on the surface of keratinocytes. IgG4 and IgG1 are the predominant IgG types. This deposit creates a characteristic “fish net” pattern.
• Indirect immunofluorescence (NIF) is a semi- quantitative method of identifying autoantibodies to the proteins of desmosome elements [3, 5, 16].
Additional evaluation methods • General blood test: may show peripheral eosinophilia.
• Serum immunoglobulins: IgG and IgA titers often correlate with disease activity and can be used to monitor therapeutic response.
• Electron microscopy: keratinocytes show a decrease in tonofilaments. Desmosomes are rarely found. The basement membrane is often damaged due to an inflammatory infiltrate [9].
Clinical Case
A patient, a 45-year-old man, came for an appointment with complaints of rashes on the skin of the axillar region. He did not treat himself and did not ask any medical help. General clinical and instrumental research within normal limits. He denies the family history of skin diseases. He has been sick for about 2 years. After a thorough history, clinical and histological examination, a diagnosis of pemphigus vegetative was made (Figures 1A-1D).

Differential Diagnosis
It is differentianed with vegetative lesions in other bullous autoimmune skin diseases, such as bullous pemphigoid or immunoglobulin A (IgA) pemphigus, chronic inflammatory plaques of Hailey-Hailey disease and especially vegetative pyoderma. Differentiating pemphigus vegetans from pyodermatitis pyostomatitis vegetans is the most difficult. Both diseases show similar clinical and histopathological findings, but immunofluorescence results are characteristically negative in pyostomatitis vegetans. Very rarely, solitary vegetative masses mimicking pemphigus vegetative may be the cutaneous manifestations of paraneoplastic pemphigus in this setting associated with malignancy. Also, this pathology should be distinguished from other pseudoepitheliomatous processes, for example, infection (for example, blastomycosis) or iododerma (for example, bromoderma) [14].
Treatment
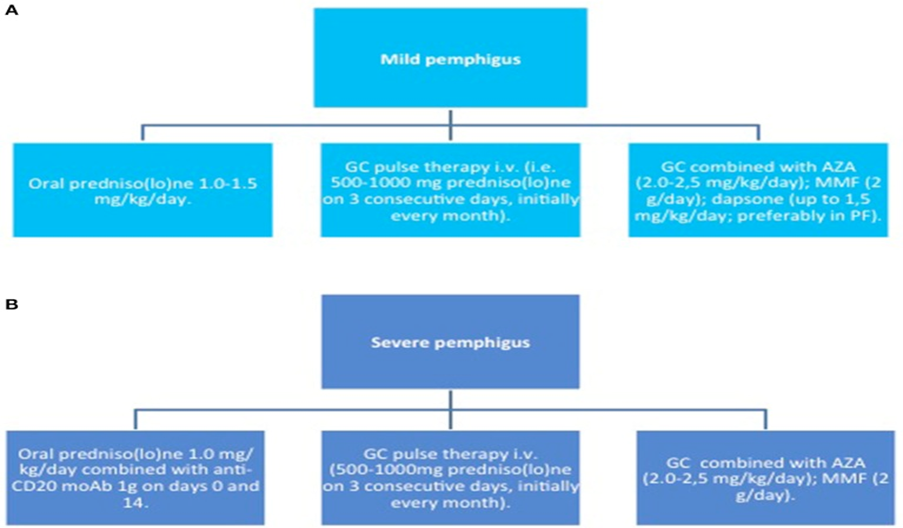
Due to the rarity of this form of the disease, the published guidelines for its management mainly rely on expert consensus (Figure 2). The goal of pemphigus treatment is to maintain a complete remission, defined as the absence of new or progression of existing lesions. Ideally, all systemic therapy should be discontinued; however, remission achieved with minimal therapy, prednisone (≤10 mg/day), or minimal adjuvant therapy (or a combination thereof) may be a more realistic goal in the treatment of pemphigus. The recommendation is to maintain remission for 1 year, and then slowly reduce the therapy for another year, taking into account the individual data of the patient and their co- morbidities.
Treatment recommended by European and Japanese guidelines: Wound care: Daily cleaning and dressings. Medical gauze and chemical coagulation.
Surgical options: Surgical excision of vegetative lesions.
Treatment in the area of the oral cavity: Mouth rinse, including liquid dexamethasone 2 times a day or clobetasol ointment.
Topical therapy:
- Class I steroids used twice a day
- Local tacrolimus in case of damage to the face area or if the patient is not sensitive to chronic steroid therapy
- Minocycline/nicotinamide at onset and relapse is used with success and avoids systemic steroids [17, 18].
Intrafocal Therapy • Triamcinolone is injected directly into the focus of the vegetative lesion Systemic Therapy: The gold standard for treatment is systemic corticosteroids. It is believed that corticosteroids increase the expression of desmoglin in keratinocytes, which leads to a rapid therapeutic effect. Corticosteroids and immunosuppressants are the most effective in the treatment of patients with pemphigus.
- Prednisone: from 0.5 to 2 mg / kg / day for 2 - 4 weeks.
- Azathioprine: 50 mg daily and higher titrate to 2.5 mg/ kg/day.
- Dapsone: 100 to 200 mg daily. Ideal for mucosal damage. Can be combined with mycophenolate or azathioprine [19].
- Mifephenolate mofetil: from 30 to 40 mg / kg / day. Risk of side effects, lymphoma and SC virus.
- Methotrexate: 15 mg/week. A safe and useful steroid- gentle remedy.
- Cyclophosphamide: works well on the oral mucosa, but has a wide side effect profile.
Combined therapies of the first line: Corticosteroid plus one of the following drugs: rituximab, mycophenolate mofetil, azathioprine, methotrexate, cyclophosphamide.
If standard steroids and immunosuppressants are insufficient, second-line treatments include: Rituximab, a CD20 monoclonal antibody, dosed at 2 mg/kg for 3 to 5 days every 4 weeks. Rituximab has been shown to induce short- term remission in 95% to 100% of pemphigus patients and correlates with a decrease in anti-DSG3 titers.
Pulse therapy: Intermittent high-dose IV corticosteroids and immunosuppressive agents to achieve faster results and minimize the side effects of long-term steroid therapy. Less common treatment options include plasmapheresis, immunoadsorption, and hematopoietic stem cell transplantation.
New therapy methods: The goal is to offer longer-lasting therapy with fewer side effects and less immunosuppression.
- B-cell activating factor (BAFF): B-cell activating factor co-stimulates the B-cell response. BAFF levels are often elevated in patients with HIV-cell autoimmune diseases, making it a novel therapeutic target [14].
- Inhibitors of Proliferation Inhibitors of Ligand (APRIL): Proliferation-inducing ligand is a key biomarker in the regulation of B cells, humoral immunity, and autoimmune disease pathogenesis. Inhibitors are a therapeutic option [18].
- Anti-cytokine therapy, anti-interleukin (IL)-4 and anti- interleukin (IL)-6): Interleukins, especially IL-4 and IL-6, have been implicated in pemphigus by enhancing Th2 overstimulation and isotype switching to IgG1 and IgG4, which have been shown to play a role in the loss of desmoglein. Direct inhibition of IL-4 and IL-6 is a potential treatment for pemphigus patients [19].
- Costimulators and co-inhibitors - manipulators and inhibitors of pathogenic signaling pathways (p38MAPK, c-Myc and EGFR) are currently being studied and may be targets for new therapies [20, 21].
Conclusion
The severity and course of the disease is variable, but before the advent of steroids, most patients with pemphigus died. Treatment with systemic steroids dramatically reduced the mortality rate. Untreated pemphigus, particularly pemphigus vulgaris, is often fatal due to susceptibility to infection and fluid and electrolyte disturbances. Morbidity and mortality are related to the extent of the disease, the maximum dose of prednisolone required to induce remission, and the presence of other diseases. The prognosis is worse in elderly patients and in patients with concomitant diseases. The prognosis is usually better in childhood than in adulthood.
References
-
Langan SM, Smeeth L, Hubbard R, Fleming KM, Smith CJ, et al. (2008) Bullous pemphigoid and pemphigus vulgaris--incidence and mortality in the UK: population based cohort study. BMJ 337: a180.
-
Jain VK, Dixit VB, Mohan H (1989) Pemphigus vegetans in an unusual site. Int J Dermatol 28(5): 352-353.
-
Basu K, Chatterjee M, De A, Sengupta M, Datta C, et al. (2019) A Clinicopathological and Immunofluorescence Study of Intraepidermal Immunobullous Diseases. Indian J Dermatol 64(2): 101-105.
-
Cozzani E, Christana K, Mastrogiacomo A, Rampini P, Drosera M, et al. (2007) Pemphigus vegetans Neumann type with anti-desmoglein and anti-periplakin autoantibodies. Eur J Dermatol 17: 530-553.
-
Gerhars M, Stadler R (1987) Pemphigus vegetans type Hallopeau. Detection of antibodies to pemphigus with direct and indirect immunofluorescence. Hautarzt 38 (6): 371-374.
-
Huang YH, Wang SH, Kuo TT, Chi CC (2005) Pemphigus vegetans occurring in a split-thickness skin graft. Dermatol Surg 31(2): 240-243.
-
Jain V, Jindal N, Imchen S (2014) Localized Pemphigus Vegetans without Mucosal Involvement. Indian J Dermatol 59(2): 210.
-
Mergler R, Kerstan A, Schmidt E, Goebeler M, Benoit S (2017) Atypical Clinical and Serological Manifestation of Pemphigus Vegetans: A Case Report and Review of the Literature. Case Rep Dermatol 9(1): 121-130.
-
Amagai M, Tsunoda K, Zillikens D, Nagai T, Nishikawa T (1999) The clinical phenotype of pemphigus is defined by the anti-desmoglein autoantibody profile. J Am Acad Dermatol 40:167–170.
-
Ruocco V, Ruocco E, Caccavale S, Gambardella A, Lo Schiavo A (2015) Pemphigus vegetans of folits (intertriginous areas). Wedge. Dermatol 33(4): 471-476.
-
Min MS, Damstetter E, Chen AYY (2018) Autoimmune blistering disorders in the setting of human immunodeficiency virus infection. Int J Womens Dermatol 4(3): 159-165.
-
Shirakata Y, Amagai M, Hanakawa Y, Nishikawa T, Hashimoto K (1998) Lack of mucosal involvement in pemphigus foliaceus may be due to low expression of desmoglein 1. J Invest Dermatol 110(1): 76-78.
-
Hietanen J (1982) Acantholytic cells in pemphigus. A scanning and transmission electron microscopic study. Acta Odontol Scand 40(5): 257-73.
-
Van Beek N, Zillikens D, Schmidt E (2018) Diagnosis of autoimmune bullous diseases. J Dtsch Dermatol Ges 16: 1077-1091.
-
Yaeen A, Ahmad QM, Farhana A, Shah P, et al. (2015) Diagnostic value of Tzanck smear in various erosive, vesicular, and bullous skin lesions. Indian Dermatol Online J 6(6): 381-386.
-
Aoki V, Sousa JX Jr, Fukumori LM, Périgo AM, Freitas EL, et al. (2010) Direct and indirect immunofluorescence. An Bras Dermatol 85: 490–500.
-
Sawai T, Kitazawa K, Danno K, Sugie N, Machizuki T, et al. (1995) Pemphigus vegetans with esophageal involvement: successful treatment with minocycline and nicotinamide. No. J Dermatol 132(4): 668-670.
-
Von Köckritz A, Ständer S, Zeidler C, Metze D, Luger T, et al. (2017) Successful monotherapy of pemphigus vegetans with minocycline and nicotinamide. J Eur Acad Dermatol Venereol 31(1): 85-88.
-
Xing YM, Kang HK, Yun JH, Roh JY, Lee JR (2011) Unexpected type of vegetarians treated with a combination of dapsone and steroid. Anne Dermatol.
-
Tavakolpour S (2017) Current and future treatment options for pemphigus: is it time to move towards more effective treatment? Int. Immunopharmacol 53: 133- 142.
-
Karpati S, Amagai M, Prussick R (1993) Pemphigus vulgaris antigen, a desmoglein type of cadherin, is located within keratinocyte desmosomes. J Cell Biol 122: 409-415.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling