Self-Assessments of the Quality of Own Life during a Viral Pandemic and War
This publication is the result of a study of the dynamics of self-assessment of quality of life indicators by young medical workers (students) against the background of the negative impact of the infodemic due to the chronic stress situation during the covid 19 pandemic, quarantine restrictions and professional communication with various patients, and the full-scale war of complete destruction that began on 24.02.22 all citizens of Ukraine. General clinical methods were used as research methods - to assess the condition of the mucous membranes, skin and somatic organs, as well as psychodiagnostic questionnaire SF36 for anonymous self-determination of the quality of one's life. The analysis of the obtained results of two hundred young medical students during 2021-2022 revealed a number of correlational dependencies from the amount of time during which they are forced to study and work against the background of the mostly negative impact of the infodemic, initially caused only by the situation of the viral pandemic and the need daily contact with various patients, and after 02.24.22 and in conditions real large-scale war and martial law. That is, already in conditions of real danger of being injured or killed during another missile attack in the rear and being infected with another viral strain of coronavirus infection due to forced daily professional contact with various somatic patients. The awareness of the presence of these two factors directly reduces their self-esteem of the quality of their own life and is, in certain situations, a sufficient factor that contributes to the formation of psychosomatic disorders as a manifestation of the initial clinical signs of somatic-emotional professional pathology, which, in particular, manifests itself in the appearance of various rashes on the skin.
Introduction
In today’s realities, the majority of the population of Ukraine is forced to live both in the conditions of somewhat relaxed quarantine restrictions due to the viral pandemic, and in the 9-month period of a large-scale war and martial law in the rear. The real life situation for the civilian population turned out to be frankly threatening and poorly predicted. No person feels sufficiently reliably protected from a very real aerosol viral infection, even as a result of accidental short-term contact (in transport, a store, a coffee shop) with a person already infected with the coronavirus, who is in the incubation period and considers himself healthy. Likewise, in fact, none of the citizens of Ukraine can consider themselves more or less protected from death, disability or significant physical injury as a result of the “liberation and peacekeeping” actions of the “Rashist” forces. In these circumstances, it is the medical workers (doctors, senior medical school students, nurses, laboratory assistants, nurses) who are in daily contact with various somatic and post-traumatic patients, definitely belong to the group of increased professional risk. Because it is this rather specific layer of the civilian population, being at the forefront of the fight against this pandemic, that they risk not only their own health but also their lives to overcome it, and by providing medical aid to wounded and injured civilians and soldiers of the Ukrainian Armed Forces.
In our opinion, it is the doctors, due to their professional education, who mostly more realistically assess the scale of this viral pandemic and war, as well as their various negative consequences for society as a whole and for themselves personally. Perhaps, precisely because of this, both the numerous shortcomings of the existing system of medical care as a whole and especially its distinct inadequacy in wartime conditions became more obvious to them. In fact, the optimistic public awareness of guaranteed medical safety “disappeared” almost instantly. Ukrainian society was forced to realize that first the outbreak of covid19, and then the “military special operation” equalized life chances for everyone, almost regardless of age, gender, economic situation, social status and political preferences. And this awareness, in turn, qualitatively changed Ukrainian society as a whole. So, all of us as citizens of Ukraine are now forced to work, fight, study, love and hate, raise children, often communicate only online, dream, live and die in this new reality.
Being scientists-clinicians and aware of the real situation of the national health care system during this pandemic and war, a distinct infodemic and barely hidden administrative helplessness, it seemed to us the most appropriate and scientifically promising to pay attention to the analysis of self-assessment of the quality of life (QoL) in different groups doctors. In times of war and pandemics, it is the doctors who are forced to risk their own health and lives every day to be at the forefront of the struggle to overcome the negative consequences of both viral pathology and various post- traumatic conditions, and not to “isolate themselves” from these problems, as a large part of the administrative “elite” of the country that fled to fight “heroically” as part of the “Monaco battalion”. In addition, medical workers, having professional education and becoming more aware of the professional risks of their work during the pandemic and war, have been anxiously waiting for the appearance of clinical signs of both viral pathology and the somatic consequences of possible physical injury from missile attacks in recent months. Therefore, it was quite logical to assume that our level of general anxiety was likely to increase and, as a result, the self-assessment of the quality of one’s own life would decrease - this integral indicator, which is formed mostly subconsciously in every human personality from a large number of various components. We were also prompted to make such a choice by the fact that in the world medical scientific literature, since the end of the last 20th century, QoL has been recognized as a mandatory and integral part of a comprehensive analysis of modern objective methods of diagnosis, assessment of treatment effectiveness, and the appropriateness of an early forecast of the real state of providing medical care assistance [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14]. Another important factor in this choice was the technical possibility of an anonymous remote screening test examination (in 10-15 minutes) of medical colleagues in conditions of a sharp reduction in personal contacts during quarantine and the need to provide 24x7 medical assistance to civilians and military personnel during wartime. The analysis of the obtained points of the self-assessment of the quality of life will be able to help, although not to improve it, but to better understand its dynamics and meaning [1, 3, 7]. And this, in turn, will also contribute to a better understanding by doctors of the realities of their own psycho-somatic state in the difficult period of the simultaneous combination of the continuation of the covid19 pandemic and a full-scale war to destroy all citizens of Ukraine.
The purpose of the study is to investigate the dynamics of self-assessment of quality of life indicators among young medical workers against the background of the negative impact of the basic chronic stress situation - the infodemic, quarantine restrictions and months of professional communication with various patients during the covid 19 pandemic and the full-scale war of destruction that began on 24.02.22.
In Order to Implement It
It Was Planned To Perform the Following Tasks: 1. To determine the “basic” level of self-assessment indicators of the quality of life of medical workers of a kind of “control” group - 4th-year students of NMU with minimal (mostly only theoretical) clinical experience. 2. To conduct a comparative analysis of the quality of life indicators of young medical workers of slightly different professional levels: “theoretic” students and students of medical universities-nurses, who combine their theoretical knowledge with professional daily active communication with various patients in conditions of quarantine restrictions and total public concern due to regular missile attacks.
Research Methods
General clinical-for a general assessment of the somatic condition; psycho-diagnostic questionnaire: adapted questionnaire SF-36 to determine the quality of life; biostatistics for the purpose of mathematical processing of the received data [3].
Testing and surveys were conducted on a completely voluntary basis in the spring of 2020 and at the beginning of the summer of 2021 remotely by students of the 4th year of the medical and dental faculties of the National Medical University named after O.O. Bogomolets, who denied the presence of signs of a real somatically understandable pathology. During the previous survey, none of them showed noticeable anxiety about the state of their own health and did not consider it necessary to systematically monitor it. They were mostly psychologically interested in the very procedure of quick anonymous self-testing to determine such, from their point of view, somewhat ephemeral concept as their own self-esteem.
It so happened that in the first 2 weeks after 24.02.2022, while continuing to hold seminar classes on dermatovenerology as scheduled, we also managed to remotely test students of the 4th year of NMU. And this took place already in qualitatively different conditions of the start of a full-scale military aggression and an attempt to seize Kyiv in 3-4 days.
In all 3 above-mentioned time periods of screening testing, in relation to individual data, only the age, gender, place of work of working students, the absence of obvious (significant) somatic pathology in their anamnesis over the last 3-5 years were established.
Ested young medical workers can be considered a kind of control group, which combines physical health, a certain psychological stability and a fairly sober professional perception of both the epidemiological features of the pandemic and the real risk of being infected or receiving physical damage during the performance of their professional duties in wartime. That is, as a result of such a specific combination, they are potentially minimally psychologically vulnerable to the impact on them of the public infodemic of the last two years of the coronavirus pandemic. But regarding the impact of the initial period of the war, it was unclear and unpredictable... For screening psycho-diagnostic testing, we used the automated Medical Outcomes Study Short Form 36 questionnaire (SF-36, version 1), with an adapted Ukrainian translation. SF-36 belongs to general (non-specialized) questionnaire tests and has been widely used for decades in various studies of quality of life in various patients with somatic pathology [3, 12]. Its basic and attractive feature is that it makes it possible to quantitatively (in conditional points) evaluate various qualitative components of QoL. Traditionally, they are divided into 8 separate scales:
- Physical functioning (PF) reflects the degree to which the general physical condition limits the performance of various everyday tasks (self-care, walking, climbing stairs, moving heavy objects, etc.) and the needs of daily existence.
- Role functioning caused by the physical condition (RF) is a measure of the impact of any negative physical manifestations on the ability to perform usual role functions in the family, at work, when communication and other everyday duties.
- Physical (pain) sensations (BP) are present, which in one way or another affect the general well-being of a person and the ability to engage in active daily activities, including everyday housework.
- Self-assessment of the general state of one’s health (GH) at the moment and in the future of life, work and treatment.
- Vitality (vital activity) (VA) reflects the subjective feeling of the fullness of one’s own strength and energy or, on the contrary, weakness, insufficiency, lack of such strength, impotence.
- Social functioning (SF) is a measure of its completeness, sufficiency and adequacy of social activity during communication from the point of view of the tested personality.
- Role functioning determined by the emotional state (RE)- to what extent the internal emotional state affects (positively or negatively) the ability to perform usual and necessary life roles in everyday life (including large expenditures of time, reduction of the volume of work, reduction of its quality).
- Mental health (MH) is a quantitative level of expressiveness of a sufficient or insufficient state of one’s own mental activity for everyday life and usual household or industrial activities.
It characterizes the mood, the presence of depression, anxiety, the general indicator of negative \ positive emotions. The scores obtained after processing the data for each such scale range from 100 (maximum result = complete well-being) to 0 (tsunami). Scientists also combined all these 8 scales fall into two qualitatively different groups: the physical component of health, or physical well-being (PW), and the psychological component of health, or mental well- being (MB\MH).
A long-term and statistically significant analysis of the results of many independent professional studies of quality of life with the help of the SF-36 test in the various groups interviewed shows that there is every reason to believe [2, 3, 4, 13]:
- 30 points or less is traditionally described in the literature as a “stormy” zone, or “You are in a sea of problems and you don’t even have an oar!”. That is, a person is at the beginning of the development of a certain psychoneurological pathology;
- 31-39 points is a zone of clearly negative self-assessment of quality of life - psychologically it is already “storming!” and the person is still trying to somehow fight with it, although it is clearly not very successful;
- 40-49 points is a zone of distinct psychological “risk”, when the self-assessment of the quality of life is clearly underestimated and has a tendency to further deterioration under the influence of very different factors;
- 50-55 points is a zone of only certain “risky instability”, when it is equally likely that some insignificant, mostly dynamic decrease-deterioration, and improvement- increase are possible;
- 56-64 points are the zone of an average acceptable level, or the conditional average statistical norm, when the significance of all scales fluctuates at the level of around 60 points;
- 65-74 points are a zone of unambiguously positive physical and mental health “peace”;
- 75-79 points is a zone of unambiguously positive physical and mental “comfortable peace”;
- 80-90 points means guaranteed and stable mental and physical “well-being”;
- 91-100 points. For a qualitative assessment of this range, the specialized literature uses the aphoristic expression “Buddha has touched you” [13].
The structure of this questionnaire makes it possible to quantitatively determine the point expressiveness of each of these 8 scales and to qualitatively “see the fine points of subsidence” of the self-assessment of QoL. And this is critically important in the preparation of both preventive and complex treatment and communication measures in the complex and very changing conditions of both a viral pandemic and a war that has begun, when we all became forced witnesses to how the myth about the supposed existence of a guaranteed medical security in the 21st century. And we all now in this new harsh reality are forced to live in the world of VUCA - instability, ambiguity, uncertainty and complexity!
Results and Discussion
Interpersonal contacts with fellow clinicians and students of the 4th year of medical and dental faculties, related to remote testing for the period from spring 2020 to March 2022, took place almost exclusively remotely due to quarantine restrictions and mainly on the initiative of the students themselves medical workers who independently learned about the possibility to more objectively assess their psychological state and quality of life (QoL). In our opinion, this testified to their considerable concern due to the ambiguity and uncertainty of their own psycho-somatic situation and the real daily danger of receiving a biological injury-an infectious viral disease. During such sporadic contacts, it was found that most of the clinical colleagues who came to us had problems sleeping, as well as apparently unmotivated emotional disturbances. This became the reason for us to offer such persons to anonymously undergo a remote screening psychological examination. A similar desire was expressed by numerous senior students of NMU, who objectively assessed their own psychological state as ambiguous and unstable. On average, we evaluated and analyzed the results of only 2-3 test subjects per day. This work was made possible mainly due to the use of the automated calculation algorithm (in points) provided by D.Ya. Raigorodskyi in his electronic version of the monograph “Practical Psychology”, and some other algorithms of such analysis [1, 2, 13].
About a hundred medical workers of both sexes, aged from 20 to 73, were gradually examined remotely. After receiving and analyzing the results of only the first ten people, we faced the problem of the lack of a kind of “foundation” or “control group”, that is, people without distinct clinical manifestations of accompanying somatic pathology and corresponding somatic complaints. This forced us to select a separate group of young (21-22 years old) medical students from 78 people who denied having any obvious somatic pathology during the previous two years and who, while studying at NMU, were in more adequate conditions for perceiving informational messages about the СOVID19 pandemic than the main segments of the population. Allocating them into a separate group allowed us to obtain “pure” self-assessments of QoL, which were mainly influenced only by external socio-psychological and informative stressors of the infodemic, partially severed social contacts due to various quarantine restrictions and the difficulties caused by them in the performance of functional professional duties by these persons at his workplace during professional communication with various patients.
What did the results of their self-assessment of their own quality of life demonstrate during the period of the beginning of the quarantine restrictions (spring 2020) and the gradual growth of the pandemic? That is, in conditions of marked activation of biological anxiety’s protective mechanisms, when such self-esteem was primarily influenced by the infodemic’s administrative and informational components, Quantitatively, this was manifested in the following score values of individual scales SF-36: PF-97.6 points; RF-81.7 points; BP-77.1 b; GH-78.2 b; VT-72.6 b; SF- 87.5 b; RE-85.1 b; MH-81.2 b; PH-68.5 b; MH-51.7 b.
From the analysis of these point values, it is obvious that in fact numerous components of the quality of life were in the zones of unambiguously positive physical and mental peace (65-74 points) or guaranteed comfortable peace (75-79 points). The lowest point quantitative self-assessment (51.7 points) fell only on the total scale of mental well-being-MH and quite objectively testified to the risky and pronounced general internal excitement of young medical students against the background of significant public anxieties and fears and mass information infodemic . This was directly confirmed by the high values of virtually all other scales of the SF-36 test, which were either in the zone of guaranteed and stable “well-being” (80-90 points), or were almost touched by the Buddha (97.5 b).
Somewhat different average values of QoL scales were found in young medical students already in the adaptation stage of chronic pandemic stress (at the end of spring 2021), that is, after a year of quarantine restrictions, several lockdowns and online training. Quantitatively, this was manifested in the following average score values of individual scales SF-36: PF-95.3 points; RF-73.1 points; BP-84.3 b; GH- 82.1 b; VT-59.2 b; SF-85.2 b; RE-58.4 b; MH-65.6 b; PH-56.7 b; MH-48.7 b.
For better visualization and understanding of the differences in the self-assessment of the quality of life of young medical students of both “control” groups with a difference of one year (beginning of spring 2020 - end of spring 2021), we arranged their score results on all scales of the SF-36 in the form of a kind of graphic display of point values of separate QoL scales, where the inner, smaller circle around the center shows the 30-point limit of the “storm” zone, and the larger one shows the 60-point limit between the zones of positive “calm” and certain “risk” (Figure 1).
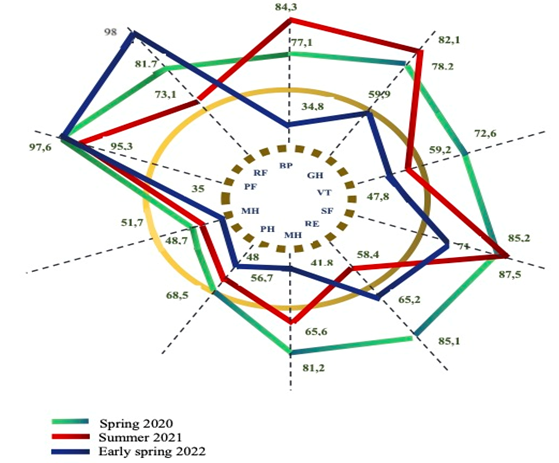
Spring 2020 = dashed line Spring-Summer 2012 = solid line Early spring 2022 = a line of separate dots Figure 1: Graphic display of the dynamics of SF36 score values in different periods of screening testing of young doctors.
Such a score display of the average results of both subgroups indicates the presence of certain discrepancies in their self-assessments of their own quality of life on many scales. You can clearly see a very significant “slump” of self-assessment scores on the scales RE (58.4 points vs. 85.1 points), MN (65.6 points vs. 81.2 points) and VT (59.2 points vs. 72.6 b.) from the zone of guaranteed well-being to the zone of only peace. And this with the simultaneous actual preservation of full physical well-being: PF-95.7 b. against 97.6 b., RF (73.1 b. against 81.7 b.) BP-74.4. And social functioning - SF (85.2 points vs. 87.5 points); That is, such high self-assessment scores of both physical health and social functioning clearly indicate the absence of obvious somatic pathologies in students in the stages of psychological activation and adaptation, which gives reason to consider them as a kind of “control” group. Only the stable “risky instability” of the results of the mental restlessness scales MH (51.7 points vs. 48.7 points) look all the more convincing. That is, students in different stages (phases of anxiety and adaptation) of chronic biological pandemic stress develop significant psycho-emotional discomfort, which lowers their self-esteem of their own quality of life according to the total scale of mental well-being.
As for the results of the testing of young doctors during the early spring of 2022, they found their graphical representation in the form of a line of individual dots in Fig.
As for the results of the testing of young doctors during the early spring of 2022, they found their graphical representation in the form of a line of individual dots in Fig. 1. When analyzing these point results, obtained during the first 2 weeks after the beginning of the military aggression of Moscow on 24.02.22, the following rather distinct differences on individual scales attract attention: • In reality, the total level of mental well-being of MH “fell” catastrophically - to only 35 points. That is, from the zone of somewhat risky instability (51.7 - 48.7 points) during the pandemic to the edge of the actual zone of internal psychological “storm” as a result of the frankly psychotraumatic impact of the start of a full-scale war. • Self-esteem also “fell” by more than 20 points (from 78.2-82.1 to 59.9) the general state of one’s own health (GH) at the moment and in the future of life and work. Although it remained within the conditionally average statistical norm. Similarly and no less significantly (from 74.1 - 84.3 to 54.8 points) the scale of actual body sensations (BP), which in one way or another affect the general well-being of a person and his ability to engage in active everyday life, also fell activity. • And this despite the fact that the indicators of purely physical (PF) functioning remained as high as possible (97.6 points), the role functioning determined by the physical condition (RF) even noticeably increased from 73.1 to 81.3 to a maximum in 98 points. However, the total physical well-being (PW) also deteriorated to 48 points and ended up in the zone of distinct psychological “risk”. • As expected, self-assessment of one’s own mental health (MH) changed most significantly (actually doubled from 81.2 to 41.8 points). This quantitative indicator of the level of expressiveness of a sufficient or insufficient state of one’s own mental activity for everyday life and usual household or industrial activities unequivocally testified to the dominance of anxiety and negative emotions, and therefore to a clear psychological “risk”, when the self- assessment of the quality of life is clearly underestimated and has a tendency to further deterioration. • Role functioning due to the emotional state (RE) turned out to be somewhat better (65.2 points) than in the summer of 2021 (58.4 points), but worse than at the very beginning of the viral (85.1 points) pandemic in the spring of 2020. That is, the beginning of military aggression expectedly and substantially (by 20 points) negatively affected the internal emotional state and the ability to perform usual and necessary life roles in everyday life. However, this type of role functioning still remained in the zone of unambiguously positive physical and mental “peace”; • Such an indicator as vital activity (VT) began to reflect the subjective feeling of weakness (47.8 points), and not the fullness of one’s own strength (72.6 -59.2 points) as it was before in the times of only viral pandemic; • To a somewhat lesser extent (from 85.2 - 87.5 points to 71 points) the self-assessment of the degree, completeness, sufficiency and adequacy of social activity (SF) decreased, remaining within the zone of unambiguously positive physical and mental “peace”.
In general, the dynamic picture of changes in the self- assessment of the quality of life of young doctors over the past 2 years indicates a clearly generally negative impact of both a biological stressor - a viral pandemic - and such a catastrophic social and psychological stressor as war. And at the same time, information related to the beginning of the war clearly had a more pronounced impact on medical students, and this despite the fact that both of these external stressors are characterized by their distinct uncertainty, obvious unpredictability and public infodemic.
Conclusion
- Any somatic, and especially such an infectious pathology as СOVID 19, is a biological stress-trauma, which almost always causes a certain bio-psychological trauma in the majority of the civilian population and is clearly more adequately perceived by medical workers - students studying dermatology.
- In the period of social infodemic, quantitative indicators of self-assessment of the quality of life of medical students without real somatically understandable dermatological pathology should be considered as a conditional standard of adequate psychological self- assessment and psychosomatic adaptation to training and clinical work in conditions of unpredictability, instability, ambiguity and uncertainty.
- The first weeks after the start of the war for the destruction of Ukraine and all its citizens led to catastrophic results of emotional self-assessments of the quality of their own lives by young doctors and the short-term appearance of skin rashes and itching in some of them.
References
-
Yu IF, Yu MM, Yu VB (2002) The Procedure of Adaptation of the International Questionnaire for Assessing the Quality of Life MOSSF-36 in Ukraine: Experience of Use in Patients with Bronchial Asthma. Ukr Pulmonol Magazine 3: 9-11.
-
Novyk AA (2007) Guide to the Study of Quality of Life in Medicine. 2nd (Edn.), M: ZAO OLMA Media Group pp: 320.
-
Ware JE, Kosinski M, Keller SD (1994) SF-36 Physical and Mental Health Summary Scales: A User’s Manual. Health Institute, New England Medical Center, Boston.
-
Amirdzhanova VN, Goryachev DV, Korshunov NY (2008) Population Indicators of Quality of Life According to the SF36 Questionnaire. (Results of the Mirage multicenter study of quality of life). J Scientific and Practical Rheumatology 1: 36-48.
-
Tulaeva EA, Ryazantsev VE, Cherapkin AV (2013) Evaluation of the Lifestyle of a Urological Patient from the Standpoint of Evidentiary Statistics. Bulletin of the Mordovian University 1-2: 194-197.
-
Rychkova SV (2009) Influence of Rehabilitation on Quality of Life Indicators in Children with Chronic Gastroduodenal Pathology. Questions of Spa Treatment. Physiotherapy and Therapeutic Physical Culture 1: 20- 22.
-
Sadykova DI (2009) Quality of Life in Adolescents with Essential Arterial Hypertension. Russian Journal of Perinatology and Pediatrics 1: 12-17.
-
Morales LS, Edwards TC, Flores Y, Barr L, Patrick DL (2011) Measurement properties of a multicultural weight-specific quality-of-life instrument for children and adolescents. Qual Life Res 20(2): 215-224.
-
Yu AE, Govorin AV, Tsvinger SM (2009) Quality of Life in Patients with Osteoarthritis. Bulletin SO RAMS 6(140): 15-18.
-
Mupagova MV, Barskova VG, Eliseeva MS () Quality of Life of Men with Gout: Are There Differences from the Population? (Results of comparative studies). J Original Studies pp: 299-303.
-
Mostak NA, Klymenko AA (2017) Use of the SF36 Questionnaire in Assessing the Quality of Life in Patients with Chronic Thromboembolic Pulmonary Hypertension. W Clinician 11: 44-49.
-
Chernega NV, Denisova MF (2011) Determination of the Quality of Life of Children with Chronic Viral Hepatitis B and Liver Cirrhosis. Perinatology and Pediatrics 2: 56- 58.
-
Ya RD (2011) Practical Psychodiagnosis. M: Bachrach-M.
-
Nasrallah HA (2021) During a Viral Pandemic Anxiety is Endemic: The Psychiatric Aspects of COVID-19. Cur Psychiatry 19(4): 3-5.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling