Iga Associated Lymphocytic Vasculopathy: an Underrecognized Entity
Immunoglobulin A (IgA) associated lymphocytic vasculopathy is an uncommonly reported entity in which IgA immune complexes evoke a lymphocytic vascular reaction instead of a neutrophilic vasculopathy. We present the clinical, histopathological and immunofluorescence features of IgA associated lymphocytic vasculopathy in a 25 year old male
Introduction
Immunoglobulin A (IgA) is the most abundant antibody present in mucosal secretions and responsible for defence against multiple microorganisms. Due to being exposed to multiple antigens, IgA antibody may sometimes lead to autoreactive host responses including vascular injury. IgA vasculitis, the most frequent vasculitis in children, is characterized by IgA immune complex deposition and neutrophil mediated inflammation in small vessels of skin, gastrointestinal tract, kidney and joints. Rarely, there may be lymphocytic infiltration which is interesting as IgA antibodies are known to activate neutrophils via IgA specific Fc receptors. We herein report a case of IgA associated lymphocytic vasculopathy that demonstrated perivascular as well as intraepidermal IgA deposits along with lymphocyte predominant infiltration.
A 25-year-old man presented with recurrent episodes of multiple red raised lesions on his legs. There was no precipitating factor or any associated systemic complaints. On examination, multiple discrete palpable as well as non- palpable purpuric lesions were present over dorsa of feet and lower one-third of the legs. Mucosa, hair and nails were normal.
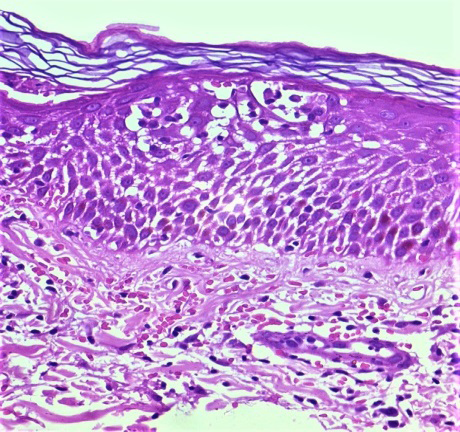
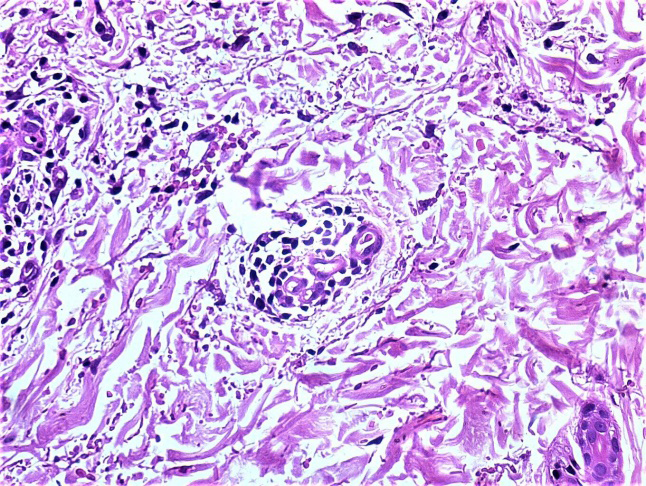
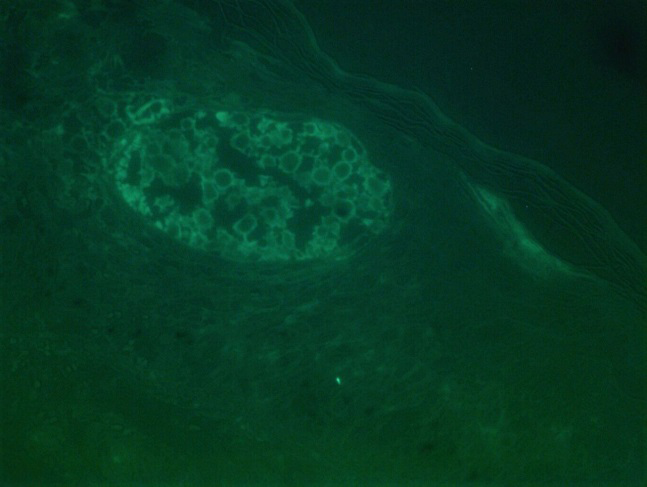
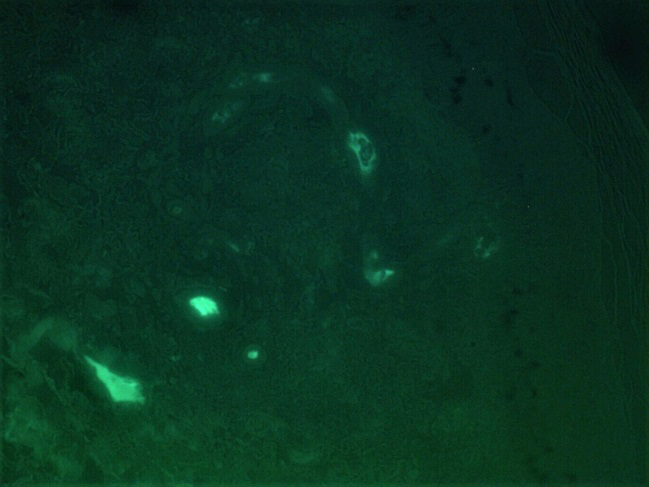
Systemic examination was unremarkable. All investigations including complete blood count, coagulation profile, liver and renal function tests, viral markers, chest radiograph, tuberculin skin test, urine examination for proteinuria and antibody profile did not reveal any abnormality. Differential diagnosis of leukocytoclastic vasculitis and adult onset IgA vasculitis was kept and biopsy from new, active lesions was sent for histopathological and direct immunofluorescence (DIF) examination. On histopathology, there was marked spongiosis throughout the epidermis, with foci of spongiotic vesicles containing lymphocytes. Exocytosis of extravasated red blood cells was present within the spongiotic areas (Figure 1). Superficial and mid-dermis showed perivascular inflammatory infiltrate, comprising predominantly of lymphocytes, red blood cell extravasation and endothelial swelling (Figure 2). On lesional direct immunofluorescence (DIF), IgA was deposited in the entire epidermis, with strong positivity within the spongiotic vesicles (Figure 3), in addition to IgA deposits in the walls of blood vessels (Figure 4). Based on clinical, histological and DIF findings, a diagnosis of IgA associated lymphocytic vasculopathy was made. Patient was given short course of steroids which led to resolution of lesions.
IgA associated lymphocytic vasculopathy was first described by Crowson, et al. in 2002 as a distinct subtype of small vessel vascular injury syndromes. It is mainly a histopathological diagnosis. Proposed pathogenesis is that IgA immune complexes through interaction with complement and/or Fc receptors on T and B lymphocytes, can induce a lymphocyte-dominant non-necrotizing vascular reaction [1]. Associations reported include viral infection, undifferentiated connective tissue disease and Berger’s disease. Our patient did not have any systemic disease or illness [1]. Clinically, both palpable and non-palpable purpuric lesions can occur on lower limbs and sometimes, on upper limbs as well. On histopathology, a superficial perivascular lymphocytic infiltrate with prominent erythrocyte extravasation and on DIF, prominent and predominant IgA deposits within cutaneous vasculature are noted. Hallmark features of neutrophilic inflammation fibrinoid necrosis and fragmented neutrohilic nuclei (leucocytoclasia) are absent. Our patient had prominent epidermal spongiosis histologically and perivascular as well as intraepidermal IgA deposition on DIF. This immunopathological finding may be the result of migration of lymphocytes from the dermal vessels into the epidermis, suggesting that the pathogenic process in IgA associated lymphocytic vasculopathy is not only confined to the dermal vessels, but may even involve the epidermis. There is no standard prescribed treatment, our patient responded to steroids.
Schamberg’s disease is a close differential diagnosis; erythrocyte extravasation, lymphocytic infiltrate and DIF positivity with IgM, fibrinogen or C3 is seen in Schamberg’s disease but IgA deposition does not occur [2]. IgA vasculitis was excluded based on lack of neutrophilic infiltration of the vessel walls, leukocytoclasia and fibrinoid necrosis.
To conclude, IgA associated lymphocytic vasculopathy is a rarely described cutaneous IgA vascular injury syndrome.
Further studies are needed to unfold the pathogenesis of IgA associated lymphocytic vasculopathy, correlate the histopathological and immunofluorescence findings and determine their clinical and prognostic significance.
References
-
Crowson AN, Magro CM, Usmani A, McNutt NS (2002) Immunoglobulin A-associated lymphocytic vasculopathy: a clinicopathologic study of eight patients. J Cutan Pathol 29(10): 596-601.
-
Ratnam KV, Su WP, Peters MS (1991) Purpura simplex (inflammatory purpura without vasculitis): a clinicopathologic study of 174 cases. J Am Acad Dermatol 25(4): 642-647.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling