Multiple Proliferating Trichilemmal Cysts with Clinical and Microscopic Correlation
Proliferating Trichilemmal Cyst (PTC), also known as pilar cyst, is an uncommon benign intradermal or subcutaneous cystic lesion. It occurs in 5–10% of the population, most commonly on the scalp of elderly women. We present the case of an elderly Moroccan woman with multiple rapidly enlarging proliferating trichilemmal cysts on her scalp, which were surgically excised. Histological analysis revealed localized cystic lesions with trichilemmal keratinization and no signs of malignancy. PTC originates from the isthmic region of hair follicles. It’s typically presents as a slow-growing, subcutaneous cystic nodule that has been present for several years, often following a history of trauma or chronic inflammation. Although several case reports have been published in the literature, those involving multiple PTCs with rapid expansion and progression are rare. Differential diagnoses included epidermoid cysts, pilomatrocomas and squamous cell carcinoma and basal cell carcinoma. PTCs are a rare histopathological entity, as their histological characteristics may not always align with their clinical behavior. A thorough histological examination is crucial to identify any focal areas of malignant transformation. Complete surgical excision with a margin of 1.0 cm to reduce recurrence, is the standard treatment. This case highlights the importance of regular follow-up to monitor for recurrence or rare malignant transformation, as clinical behavior may not align with histological findings.
Abbreviations
PTC: Proliferating Trichilemmal Cyst; TCs: Trichilemmal Cysts; ECs: Epidermoid Cysts.
Introduction
Proliferating Trichilemmal Cyst (PTC), also known as pilar cyst, is an uncommon benign intradermal or subcutaneous cystic lesion [1]. It occurs in 5–10% of the population, most commonly on the scalp of elderly women. PTC typically presents as a slow-growing, subcutaneous cystic nodule that has been present for several years, often following a history of trauma or chronic inflammation [2]. Clinically, trichilemmal cysts (TCs) are similar to epidermoid cysts (ECs), differing primarily in their frequency and distribution. Histologically, TCs are characterized by abrupt keratinization and abundant eosinophilic cytoplasm, without a granular layer, in contrast to ECs [3]. In rare instances, a proliferating trichilemmal cyst may transform into a malignant form [4].
Although several case reports have been published in the literature, those involving multiple PTCs with rapid expansion and progression are rare. We present the case of an elderly woman with multiple rapidly enlarging proliferating trichilemmal cysts (PTCs).
Case Presentation
An 80-year-old woman presented to our outpatient department with multiple soft skin tumors on her scalp,

which had rapidly grown over the past 7 months.
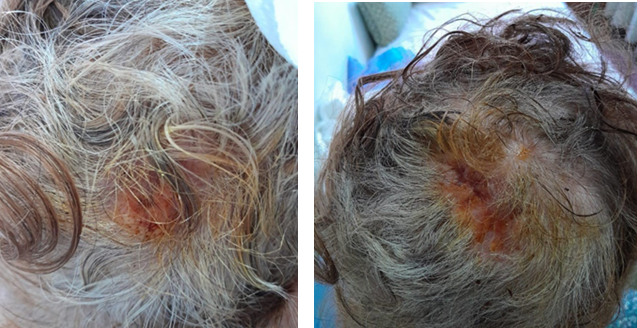
During the clinical examination, the scalp revealed multiple firm, elevated nodular lesions with a smooth surface in the parietal and occipital regions, some of which were multilobulated, ranging from approximately 2 cm to 5 cm in size. The overlying skin exhibited an inflammatory and keratinizing appearance in certain areas (Figure 1).
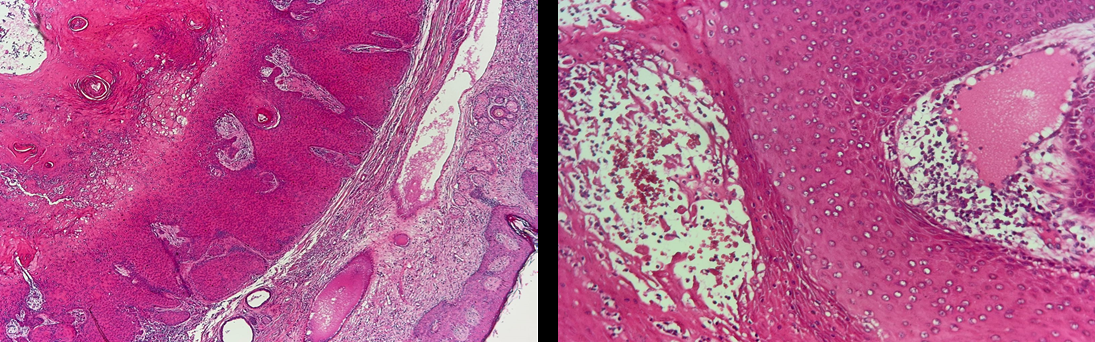
The tumors were surgically excised through radical excision (Figure 2), and histopathological examination revealed localized cystic lesions in the subcutaneous tissue. The cysts showed an acanthotic epidermis with abrupt trichilemmal keratinization. The cyst lumen contained dense eosinophilic material, with no major atypia (Figure 3). The final histopathological diagnosis was proliferating trichilemmal cysts of the scalp.
Discussion
Proliferating pilar cysts were initially described by Wilson-Jones in 1966. These neoplasms originate from the isthmic region of the hair follicle and are histologically distinguished by the presence of trichilemmal keratinization [3].
A typical clinical presentation of proliferating trichilemmal cysts is a slowly growing subcutaneous nodule that eventually develops into a large nodular mass, in contrast to our patient who exhibited rapid progression. Rapid growth of these lesions may suggest malignant transformation into carcinoma.
Histologically, PTC is characterized by a squamous epithelium in the center of the lobules that transitions into trichilemmal keratinization, with an abrupt change to dense keratin without a granular layer, leading to the formation of homogeneous keratin cysts [5]. While PTC is typically regarded as biologically benign, cases of malignant transformation have been reported [1, 5, 6, 7, 8, 9, 10].
The differential diagnosis of TCs includes epidermoid cysts, pilomatricoma, , sebaceoma, keratoacanthoma , sweat gland tumor , cutaneous squamous cell carcinoma, basal cell carcinoma, trichilemmal carcinoma and cutaneous angiosarcoma [11].
Despite the rapid growth of the lesion observed in our case, histological analysis showed no significant cytological atypia or tissue invasion to support a diagnosis of carcinoma [12, 13]. The standard treatment for proliferating trichilemmal cysts is complete local excision, and some studies suggest a margin of 1.0 cm to reduce the risk of recurrence [14, 15].
Conclusion
PTCs are a rare histopathological entity, as their histological characteristics may not always align with their clinical behavior. A thorough histological examination is crucial to identify any focal areas of malignant transformation. Additionally, regular clinical follow-up is essential to monitor for potential recurrence or metastasis.
References
-
Markal N, Kurtay A, Velidedeoglu H, Hucumenoglu S (1998) Malignant transformation of a giant proliferating trichilemmal tumor of the scalp: patient report and literature review. Ann Plast Surg 41: 314-316.
-
Laing V, Knipe RC, Flowers FP, Stoer CB, Caro FA (1991) Proliferating trichilemmal tumor: report of a case and review of the literature. J Dermatol Surg Oncol 17: 295- 298.
-
Ramaswamy AS, Manjunatha HK, Sunilkumar B, Arunkumar SP (2013) Morphological Spectrum of Pilar Cysts. N Am J Med 5: 124-128.
-
Alam K, Gupta K, Maheshwari V, Varshney M, Jain A, et al. (2015) A large proliferating trichilemmal cyst masquerading as squamous cell carcinoma. Indian J Dermatol 60: 104-104.
-
Park BS, Yang SG, Cho KH (1997) Malignant proliferating trichilemmal tumor showing distant metastases. Am J Dermatopathol 19: 536-539.
-
Amaral AL, Nascimento AG, Goellner JR (1984) Proliferating pilar (trichilemmal) cyst; report of two cases, one with carcinomatous transformation and one with distant metastases. Arch Pathol Lab Med 108: 808- 810.
-
Saida T, Oohara K, Hori Y, Tsuchiya S (1983) Development of a malignant proliferating trichilemmal cyst in a patient with multiple trichilemmal cysts. Dermatologica 166: 203-208.
-
Weiss J, Heine M, Grimmel M, Jung EG (1995) Malignant proliferating trichilemmal cyst. J Am Acad Dermatol 32: 870-873.
-
Hyung JK, Tae SK, Kyung HL, Young MK, Chang HS (2001) Proliferating trichilemmal tumors: CT and MR imaging findings in two cases, one with malignant transformation. Am J Neuroradiol 22: 180-183.
-
Sang BB, Kuh KL, Ju SK, Lee H, Lee NS, et al. (2001) A case of malignant proliferating trichilemmoma of the scalp with multiple metastasis. Korean J Intern Med 16: 40- 43.
-
Peryassu MA, Peryassu BC, Peryassu RC, Maceira J, Silva M (2013) Proliferating trichilemmal tumor: a case on the nose of a 70-year-old man. Case Rep Dermatol 5: 248- 253.
-
Gamboa L, Castro M, Cherit J, Memije E (2013) Proliferating trichilemmal cyst: the value of ki67 immunostaining. Int J Trichology 5: 115-117.
-
Valerio E, Parro FHS, Macedo MP, Pinto CAL (2019) Proliferating trichilemmal cyst with clinical, radiological, macroscopic, and microscopic correlation. An Bras Dermatol 94(4): 452-454.
-
Kiel CM, Homoe P (2021) Giant, Bleeding, and Ulcerating Proliferating Trichilemmal Cyst, With Delayed Treatment Due to Coronavirus Outbreak: A Case Report and Review of the Literature. Front Surg 8: 680160.
-
Kawaguchi M, Kato H, Suzui N, Miyazaki T, Tomita H, et al. (2021) Imaging findings of trichilemmal cyst and proliferating trichilemmal tumour. Neuroradiol J 34(6): 615-621.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling