Clinical Pathological Correlations of VEGF Protein Expression in Gastric Cancer at a Tertiary Facility in Uganda
Background: Gastric cancer ranks as the 5th most common cancer worldwide and is the 3rd leading cause of cancer deaths, responsible for approximately 783,000 deaths annually. In Uganda, its incidence has risen from 0.8 per 100,000 people in 1960 to 9 per 100,000 in 2014. Although vascular endothelial growth factor (VEGF) protein expression is critical for gastric cancer management, its prevalence in Ugandan patients is unknown. Objective: This study aimed to determine the prevalence of VEGF protein expression in gastric cancer and investigate related clinicopathological features at the Makerere University Pathology Department. Methods: A cross-sectional study was performed using conveniently sampled archived tissue blocks from patients diagnosed with gastric adenocarcinoma. These samples underwent Hematoxylin and Eosin (H&E) and immunohistochemistry (IHC) staining. Results: The study analyzed 100 specimens with a male to female ratio of 1.56:1 and an average age of 59.4 years. VEGF expression was positive in 57.0% of cases. The intestinal Lauren subtype constituted 79% of cases, while the diffuse subtype made up 21%. The predominant histological subtype was tubular adenocarcinoma (52.0%). Most cases were poorly differentiated (42.0%), well-differentiated (31.0%), and moderately differentiated (27.0%). Higher VEGF expression was observed in lower tumor grades (71.0%) (p=0.059). Tubular adenocarcinomas exhibited the highest VEGF expression (p=0.099). Male patients showed higher VEGF expression (P=0.610). Mucinous adenocarcinoma had the lowest VEGF expression (p=0.004), and poorly differentiated adenocarcinomas also had very low VEGF expression (p=0.049). Conclusion: The study revealed significant overexpression of VEGF in gastric adenocarcinoma tissues, with varying associations to different clinicopathological variables.
Abbreviations
ADB: African Development Bank; COVID: Coronavirus Disease; H&E: Hematoxylin and Eosin; IHC: Immunohistochemistry; P-Value: probability value; UCI: Uganda Cancer Institute; VEGF: Vascular Endothelial Growth Factor; WHO: World Health Organization.
Introduction
Gastric carcinoma is the fifth most common cancer globally, with 1,033,701 new cases reported in 2018, equating to 11.35 cases per 100,000 people [1]. According to Globocan 2018 data, it is the third leading cause of cancer-related deaths, accounting for approximately 783,000 deaths in the same year [2, 3]. There is significant geographical variation in the incidence and mortality rates of gastric cancer, with higher rates in Japan, China, Central and Southern America, and lower rates in North America, West Africa, and Southern Central Asia [3].
In Uganda, the incidence of gastric cancer has increased more than elevenfold, from 0.8 per 100,000 people in the 1960s to 9 per 100,000 in 2014 [4]. Unfortunately, in many countries, gastric cancer is often detected at advanced stages, making curative surgery infeasible [5, 6, 7]. Despite improvements in survival rates over recent decades, the prognosis remains poor due to late-stage diagnoses, rendering many cases inoperable [8].
Gastric carcinoma, like other solid tumors, shows varying levels of vascular endothelial growth factor (VEGF) protein expression, ranging from 26.7% to 89.9% [9]. VEGF expression also varies by age and gender, with higher expression seen in males and older individuals [10, 11, 12]. However, in Uganda, the prevalence of VEGF protein expression in gastric cancer and its impact on treatment and prognosis are largely unknown. This cross-sectional study aims to determine the frequency of VEGF expression in Ugandan patients and describe their characteristics.
Methods and Materials
Study Design
This study was a laboratory-based cross-sectional study.
Study Setting
This study was conducted in the Department of Pathology at Makerere University, College of Health Sciences, in Kampala, Uganda. This department plays a crucial role in teaching, research, and providing diagnostic biopsy and autopsy services for the entire country. The department receives and processes an average of 4,000 to 8,000 tissue biopsies per year and archives an average of 10 tissue blocks with gastric cancer annually.
Study Duration
This study was conducted over a period of approximately four months, from March 2021 to June 2021.
Study Population
The study consisted of archived formalin-fixed paraffin- embedded (FFPE) tissue blocks of patients diagnosed with gastric cancer in the Department of Pathology at Makerere University from January 2009 to December 2020.
Selection Criteria
Inclusion Criteria: Archived formalin-fixed and paraffin- embedded (FFPE) tissue blocks of patients diagnosed histologically with invasive gastric cancer at the Department of Pathology, Makerere University, from January 2009 to December 2020.
Exclusion Criteria: Tissue blocks that were poorly fixed/ processed, extensively damaged, poorly kept, with extensive necrosis, or from patients with a history of preoperative chemotherapy or radiotherapy were excluded from the study.
Sampling Method and Sample Size Estimation
Cases that met the above inclusion criteria were selected using a convenience sampling method starting from December 2020, moving backwards until the required sample size was achieved. The identified archived tissue block numbers were retrieved from the department archive using the laboratory accession number, demographics, and clinical ethical data on the request forms. The sample size was determined using the Kish Leslie formula (Kish, 1965) as follows:
( ) 2
2 * 1 Z P P N E
− = Where: N= Sample size Z = Standard normal deviation at a 95% confidence interval, corresponding to 1.96 P = Prevalence of VEGF protein expression; since this is unknown for Uganda, a prevalence rate of 68.7% from a study conducted at Cairo University, Egypt, was applied [13] E = Standard error between the estimated and true population prevalence, accepted as 5% for this study ( ) 2
2 1.96 *0.687 1 0.687
0.05 N − = N=331 The number of tissue blocks (Population size) with the diagnosis of gastric carcinoma was estimated to be around 120.
Therefore, using finite population correction, the actual sample required was calculated as follows: N= Calculated sample size* Population size/Calculated sample size + Population size-1 Calculatedsamplesize*Populationsize Calculatedsamplesize+Populationsize-1 N =
331*120 331 120 1 N = + −
N = 88.26 Therefore, the minimum sample size required for the study was 89. A sample size of 100 was consequently considered for this study.
Study Variables
Independent Variables: These included age, sex, histological subtypes, and grade. Dependent Variable: The dependent variable was VEGF immunoreactivity.
Precautions Taken During the COVID-19 Pandemic
The following precautions were taken to protect investigators during the COVID-19 pandemic:
- Personal protective equipment (PPE) such as face shields, gloves, and face masks were routinely used during laboratory work.
- Social distancing with colleagues in the laboratory was always observed.
- Hand sanitizing before and after laboratory work was routinely practiced.
Tissue Preparation, Staining, and Classification
Tissue processing and HE Staining: Sections of 4-micron thickness were cut from formalin-fixed and paraffin- embedded (FFPE) tissue blocks using a microtome machine. Care was taken to handle sections delicately to avoid damage. Sections were floated on water maintained below the melting point of wax to remove wrinkles and then mounted on labeled, saline-coated glass slides for proper identification. The slides were heated in an oven at 55-65°C for 30–60 minutes to melt the wax and ensure tissue adhesion to the glass.
Subsequently, sections were dewaxed in xylene for approximately 5 minutes to remove paraffin wax. They were then dehydrated in a series of graded alcohols (100%, 90%, 70%) for 1–3 minutes each to remove water from the tissue. After dehydration, sections were rinsed in distilled water for at least 30 seconds to remove residual alcohol.
Hematoxylin and Eosin (H&E) staining followed standard procedures: sections were immersed in hematoxylin solution to stain nuclei blue, followed by washing in acid alcohol to remove excess hematoxylin and enhance contrast. Counterstaining with eosin imparted a pink coloration to cytoplasm and extracellular matrix. Stained slides were examined under a light microscope by the principal investigator and supervising pathologists to visualize cellular morphology and tissue architecture.
Tumor Classification & Grading: Tumors were classified based on histological typing according to the Lauren and WHO classification systems. This classification system helped categorize tumors into different subtypes based on their morphological features. Additionally, tumor grading was performed to evaluate the degree of differentiation and aggressiveness of the tumor cells. The grading system played a crucial role in predicting prognosis and guiding treatment decisions.
Immunohistochemistry (IHC) Scoring: Tissue sections underwent immunohistochemical staining to evaluate VEGF expression in tumor cells. The expression of VEGF was assessed by the principal investigator and corroborated by supervising pathologists. VEGF immunoreactivity was detected in the cytoplasm of the tumor cells. The IHC score was calculated by multiplying the percentage of positive cells by the staining intensity. Percentage of positive cells: Scored as 0 if less than 5% of tumor cells stained, 1 if 5%-25% stained, 2 if 26%-50% stained, and 3 if >50% stained. Staining intensity: Scored as 0 for negative immunoreaction, 1 for weak intensity, 2 for moderate intensity, and 3 for strong intensity. The product of these two parameters ranged between 0 and 9. Cases with scores equal to or higher than 1 were considered positive for VEGF expression. Discrepancies in scoring were resolved by soliciting a third opinion from another pathologist.
Data Collection Procedures
Clinical and demographic data were retrieved from request forms. Histological typing and grading were performed by the principal investigator and confirmed by supervising pathologists. VEGF immunoreactivity was assessed and scored by the principal investigator and confirmed by supervising pathologists. Results were recorded in data collection forms.
Statistical Analysis
Data were entered into an Excel sheet, summarized using descriptive statistics, and presented in tables and graphs. Chi-square test and t-test were used to compare variables with the expression of VEGF protein. Bivariate analysis using logistic regression was conducted to obtain crude odds ratios (OR). Multivariate logistic regression was performed to determine independent factors associated with VEGF protein expression, adjusting for variables with a p-value <0.2 at the bivariate level and those known to affect VEGF expression from literature. Confounding and interaction were assessed, and a parsimonious model with significant adjusted R^2 and a non-significant Pearson’s chi-square test was considered. The significance level was set at a 95% confidence interval and a p-value ≤ 0.05.
Results
Social Demographic Characteristics
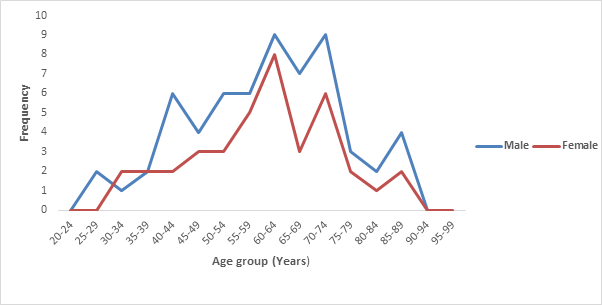
The study included a total of 100 specimens. The gender distribution was 61% males and 39% females, indicating a male predominance. The mean age of the participants was 59.4 years, with a standard deviation of 14.5 years. The age range was 44.5 to 73.9 years. While the mean age was calculated for the overall sample, further analysis by gender revealed similar mean ages for males (59.44 years) and females (59.21 years). These findings were summarized in Figure 1.
Histopathological Findings
The majority of cases were tubular adenocarcinoma (52%), followed by papillary adenocarcinoma (18%), poorly cohesive carcinoma (17%), mucinous adenocarcinoma (9%), and signet ring cell carcinoma (4%). Most cases (79%) belonged to the intestinal type according to the Lauren classification, while 21% were of the diffuse type. These findings are summarized in Table 1. The study categorized tumor grades into low (grade I) and high grades (grades II and III). There were 31 cases of grade I gastric adenocarcinoma, 22 cases of grade II, and 47 cases of grade III, as shown in Table 2.
| Tumor Classification & Grading | Frequency(%) |
|---|---|
| WHO histological type | |
| Tubular adenocarcinoma | 52(52.0) |
| Papillary adenocarcinoma | 18(18.0) |
| Poorly cohesive carcinoma | 17(17.0) |
| Mucinous adenocarcinoma | 9(9.0) |
| Signet ring cell carcinoma | 4(4.0) |
| Lauren classification | |
| Intestinal type | 79(79.0) |
| Diffuse type | 21(21.0) |
| Histological grade | |
| Poorly differentiated | 42(42.0) |
| Well differentiated | 31(31.0) |
| Moderately differentiated | 21(27.0) |
Table 1: Proportions of WHO Histologic Types, Lauren Classification, Histological Grades.
| Tumor Grades | ||
|---|---|---|
| VEGF immunoreactivity | Low grade | High grade |
| Positive VEGF | 22(71.0%) | 35(50.7%) |
| Negative VEGF | 9(29.0%) | 34(49.3%) |
| Chi=3.5762, p=0.059 |
Table 2: Proportions of VEGF Immunoreactivity in Low and High Tumor Grades.
VEGF Expression and Immunoreactivity
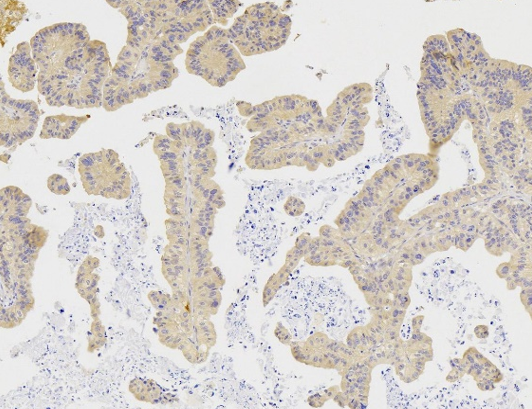
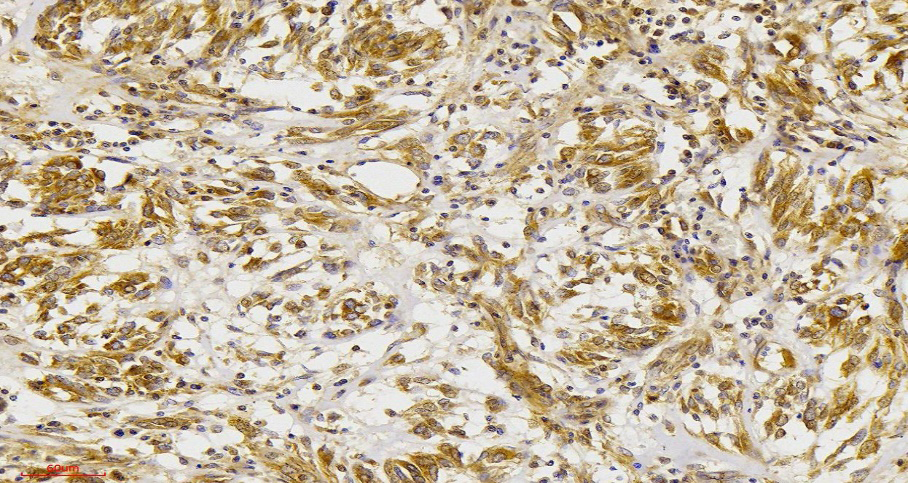
The prevalence of positive VEGF expression was found to be 57% among the total cases, as shown in Table 3. VEGF protein expression was more common in specimens from males (63.2%) compared to females, as shown in Table 3. The tubular type adenocarcinoma had the highest VEGF immunoreactivity (47.4% of positive cases), followed by papillary (26.3%), poorly cohesive carcinoma (17.5%), mucinous (5.4%), and signet ring carcinoma (3.5%). Differences in VEGF immunoreactivity were also shown in Figure 2 & Figure 3 respectively. However, there was no statistically significant difference in VEGF immunoreactivity according to histological subtypes, as shown in Table 4.
| Sex | ||
|---|---|---|
| VEGF immune-reactivity | Male | Female |
| Positive VEGF | 36(63.2%) | 21(36.8%) |
| Negative VEGF | 25(58.1%) | 18(41.9%) |
| Chi= 0.2596, p= 0.610 |
Table 3: VEGF Immunoreactivity According to sex.
| VEGF Immuno-Reactivity | |||
|---|---|---|---|
| Histological types | Positive VEGF | Negative VEGF | |
| Papillary | 15(26.3%) | 3(7.0) | |
| Tubular | 27(47.4%) | 25(58.1) | |
| Mucinous | 3(5.4%) | 6(14.0%) | |
| Signet ring cell | 2(3.5%) | 2(4.7%) | |
| Poorly cohesive | 10(17.5%) | 7(16.3%) | |
| Chi= 7.7992, p 0.099 | |||
| Clinical Pathological Factors | Positive n (%) | Negative n (%) | P-value |
| Age | 0.621 | ||
| ≤59 years | 25 (54.4) | 21 (45.6) | |
| >59 years | 32 (59.3) | 22 (40.7) | |
| Sex | 0.61 | ||
| Male | 36(63.2) | 25 (58.1) | |
| Female | 21 (36.8) | 18 (41.9) | |
| Tumor Location | 0.656 | ||
| Cardia | 6 (66.7) | 3(33.3) | |
| Non-cardia | 24 (52.2) | 22 (47.8) | |
| Not specified | 26 (59.1) | 18 (40.9) | |
| Histological Subtype (WHO) | 0.099 | ||
| Papillary | 15 (26.3) | 3(7.0) | |
| Tubular | 27 (47.4) | 25(58.1) | |
| Mucinous | 3 (5.4) | 6 (14.0) | |
| Poorly cohesive signet ring | 2 (3.5) | 2 (4.7) | |
| Poorly cohesive non-signet ring | 10(17.5) | 7 (16.3) | |
| Histological Subtype (Lauren) | 0.63 | ||
| Intestinal | 46 (58.2) | 33 (41.8) | |
| Diffuse/Mixed | 11(52.4) | 10 (47.6) | |
| Tumor Grade | |||
| Well-differentiated (Grade I) | 22(38.6) | 9 (20.9) | |
| Moderately-differentiated (Grade II) | 15(26.3) | 12 (27.9) | 0.077 |
| Poorly differentiated (Grade III) | 20 (35.1) | 22 (51.2) | 0.029 |
Table 4: Proportions of VEGF Reactivity According to WHO Histological Types.
Relationship of VEGF with Histological Findings, Social Demographics, and Clinicopathological Factors
Increasing age was associated with higher VEGF protein expression, although this association was not statistically significant (p=0.131, CI: 0.99-1.06). VEGF expression showed a decreasing trend among females compared to males, but this difference was not statistically significant (p=0.214, CI: 0.22-1.41). While VEGF expression was higher in tubular adenocarcinomas compared to other subtypes, this difference was not statistically significant. However, mucinous adenocarcinomas exhibited significantly lower VEGF expression compared to papillary adenocarcinomas (p=0.015, CI: 0.02-0.64).
Lower grades (grade I) had higher VEGF expression compared to higher grades (grades II and III), indicating a negative correlation between tumor grade and VEGF expression. This difference was statistically significant. Additionally, mucinous type gastric adenocarcinoma was associated with lower VEGF immunopositivity compared to papillary type adenocarcinoma, which was also statistically significant (p=0.004, CI: 0.01-0.36). These findings are summarized in Table 5.
Discussion
The main objective of this study was to determine the prevalence of VEGF protein expression and associated clinicopathological features in gastric cancer. One hundred conveniently sampled formalin-fixed and paraffin-embedded tissue blocks were included in the study. The prevalence of VEGF and other clinicopathological patient characteristics were determined and analyzed. The prevalence of VEGF protein expression among the patients with gastric cancer was 57.0%.
Ma, et al. [13] found a 55.92% VEGF positive rate in gastric carcinoma, which is similar to the current study’s findings. Ma’s study used a sample size of 118 participants, with the number of males being twice that of females, and the mean age of the participants was 59.2 years. Similarly, the current study had a sample size of 100, a mean age of 59.4 years, and a male-to-female ratio of 1.56 to 1. The similarities in patient demographics between the two studies likely contribute to the observed similarities in VEGF expression levels.
However, the prevalence in this study was higher than that reported in some other studies and lower compared to others. Hafez, et al. [10] from Cairo University found a 66.7% VEGF expression rate in a study of 83 patients, which was higher than the current study’s findings. The difference could be due to the staining protocols and methods used, as Tahoun and Hafez used an automated slide stainer, while manual staining methods were used in this study.
Using a ready-to-use antibody, Song, et al. [14] found a 76.09% VEGF expression rate in 46 cases. The geographical variation and differences in the preparation of the anti- VEGF antibodies could account for the variation in VEGF expression between Song’s study and the current study. In this study, increasing histological grade was associated with reduced VEGF immunopositivity. Hafez NH, et al. [10] reported that VEGF protein expression increased with tumor grade, which may be due to different immunohistochemistry scoring methods and sample sizes.
However, the findings of the current study align with those of Badescu A, et al. [15] from Craiova University, Romania, who found higher VEGF expression in lower grades (G1-G2) compared to grade III (G3). Both studies used a similar antibody clone, VG1. Maeda K, et al. [16] also reported higher VEGF expression (54%) in well-differentiated gastric adenocarcinomas versus 36.7% in poorly differentiated cases, with similar mean ages of patients.
The reduction in VEGF immunopositivity across increasing histological grades may be due to neoangiogenesis, where new blood vessels emerge from existing ones, as evidenced across different histological grades of gastric cancer. This suggests that VEGF protein is differentially expressed across all tumor grades of gastric cancer, with higher expression in lower grades. VEGF plays an important role in gastric cancer development and can be used as an index for diagnosis and prognosis.
Significantly, VEGF immunopositivity was markedly lower in mucinous gastric adenocarcinomas compared to papillary type. Although no specific literature was found on this, Hafez NH, et al. [10] reported differential VEGF expression among WHO histological subtypes of gastric cancer, although their findings were not statistically significant. The different sample sizes used in the studies could account for the variation in results.
Despite the lack of statistical significance, VEGF protein expression increased with patient age in this study. Similar results were found by Hafez NH, et al. [10] & Wang, et al. [17], suggesting that age is an independent prognostic factor for gastric cancer. VEGF immunopositivity among females was lower compared to males, although this difference was not statistically significant. This finding is consistent with other studies by Hafez NH, et al. [10], and Tsujitani S, et al, [18] who also found higher VEGF expression in males.
Xiayi Li, et al. [19] in China found similar results despite using a sample size of 255, which was more than twice the size of the current study. Therefore, the current study’s findings are consistent with several previous studies, indicating a higher VEGF protein expression in males compared to females. Since VEGF is an independent marker of prognosis, males are more likely to have a poor prognosis.
However, this study was limited by factors such as improperly filled laboratory request forms and poorly stored tissue blocks, which might have affected the results. Nonetheless, the study shows that a significant number of patients with gastric cancer in Uganda express VEGF protein, with significantly lower expression in mucinous type gastric adenocarcinoma and markedly lower expression in grade 3 cancers.
Limitations of the Study
Inappropriate tissue fixation affected immunohistochemistry results due to problematic antigen retrieval during the process. Incompletely filled and poorly filled histology request forms made the process of data collection difficult as some of the information to use in the study was missing. Poor storage of the tissue blocks affected the overall quality of the study results
Conclusion and Recommendation
The study demonstrated significant overexpression of VEGF in gastric adenocarcinoma tissues, and this expression correlated differently with various independent variables examined in this study. Therefore, VEGF could serve as a valuable biomarker for assessing the biological behavior of tumors in patients with gastric adenocarcinoma.
To enhance research results, generalizability, and impact, similar multi-center research studies in the “stomach cancer belt” involving large sample sizes are highly encouraged. Given the role of VEGF in patient stratification and prognostication, VEGF antibody testing should be included in routine workup and management of gastric cancer patients. Additionally, anti-VEGF antibodies should be made accessible to researchers to enable impactful health research for better patient care.
Data Availability
Data is available in hard copies and can be accessed on request.
Ethical Approval
Permission to conduct the study was obtained from both the School of Biomedical Sciences Research and Ethics Committee (SBSREC) and the Uganda National Council of Science and Technology. The SBSREC also granted a waiver of consent for the study. To maintain confidentiality, patient names and biopsy numbers were replaced with unique identification numbers assigned to each specimen.
Consent
Informed consent was obtained from all the participants before they were involved in the study.
Conflicts of Interest
The authors affirm that they have no conflicts of interest.
Authors Contributions
M.A. designed the study, collected and managed the data, analyzed it, and participated in manuscript development and revision. K.S., W.H., M.O., R.K., and G.O. contributed to concept development, study design, data collection, and data analysis and revision. M.B. was responsible for manuscript development and reading. W.A., N.V., N.Y., and T.O. were responsible for manuscript revision and analysis. D.L.N. conducted the H&E and IHC staining. All authors have read and approved the final manuscript.
Acknowledgements
Authors acknowledge the African Development Bank and the Uganda Cancer Institute for the financial support rendered in the conducting of this research.
References
-
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68(6): 394- 424.
-
Rawla P, Barsouk A (2019) Epidemiology of gastric cancer: global trends, risk factors and prevention. Przegla̜d Gastroenterol 14(1): 26-38.
-
Tarupi W, De Vries E, Cueva P, Yépez J (2013) Stagnation in decreasing gastric cancer incidence and mortality in Quito: Time trend analysis, 1985-2013. J Cancer Epidemiol.
-
Asombang AW, Rahman R, Ibdah JA (2014) Gastric cancer in africa: Current management and outcomes. World J Gastroenterol 20(14): 3875-3879.
-
Ibingira CBR (2001) Management of cancer of the stomach in Mulago hospital Kampala, Uganda. East Afr Med J 78(5): 233-237.
-
Mabula JB, Mchembe MD, Koy M, Chalya PL, Massaga F, et al. (2012) Gastric cancer at a university teaching hospital in northwestern Tanzania: a retrospective review of 232 cases. World J Surg Oncol 10: 257.
-
Zhu Z, Sun X, Wang J, Sun Z, Wang Z, et al. Histopathology- based prognostic score is independent prognostic factor of gastric carcinoma. BMC Cancer 14: 663.
-
Uprak TK, Attaallah W, Celikel CA, Ayranci G, Yegen C (2015) HER-2 incidence in gastric cancer, its association with prognosis and clinicopathological parameters. Turk J Surg 31(4): 207-213.
-
Park DJ, Thomas NJ, Yoon C, Yoon SS (2015) Vascular endothelial growth factor a inhibition in gastric cancer. Gastric Cancer 18(1): 33-42.
-
Hafez NH, Tahoun NS (2016) Expression of cyclooxygenase 2 and vascular endothelial growth factor in gastric carcinoma: Relationship with clinicopathological parameters. J Egypt Natl Cancer Inst 28(3): 149-156.
-
Lazar D, Taban S, Raica M, Sporea I, Cornianu M, et al. (2008) Immunohistochemical evaluation of the tumor neoangiogenesis as a prognostic factor for gastric cancers. Rom J Morphol Embryol 49(2): 137-148.
-
Wei B, Tai Y, Tong H, Wen S-L, Tang S-H, et al. (2017) Correlations between VEGF-A expression and prognosis in patients with gastric adenocarcinoma. Int J Clin Exp Pathol 10(8): 8461-8469.
-
Ma J, Zhang L, Ru G-Q, Zhao Z-S, Xu W-J (2007) Upregulation of hypoxia inducible factor 1α mRNA is associated with elevated vascular endothelial growth factor expression and excessive angiogenesis and predicts a poor prognosis in gastric carcinoma. World J Gastroenterol 13(11): 1680-1686.
-
Song Z-J, Gong P, Wu Y-E (2002) Relationship between the expression of iNOS,VEGF,tumor angiogenesis and gastric cancer. World J Gastroenterol 8(4): 591-595.
-
Bădescu A, Georgescu CV, Vere CC, Crăiţoiu S, Grigore D (2012) Correlations between Her2 oncoprotein, VEGF expression, MVD and clinicopathological parameters in gastric cancer. Romanian J Morphol Embryol Rev Roum Morphol Embryol 53(4): 997-1005.
-
Maeda K, Chung YS, Ogawa Y, Takatsuka S, Kang SM, et al. (1996) Prognostic value of vascular endothelial growth factor expression in gastric carcinoma. Cancer 77(5): 858-863.
-
Wang L, Yang M, Shan L, Qi L, Chai C, et al. (2012) The role of SPARC protein expression in the progress of gastric cancer. Pathol Oncol Res 8(3): 697-702.
-
Tsujitani S, Saito H, Maeta Y, Yamaguchi K, Tatebe S, et al. (2004) Neoangiogenesis in patients with gastric carcinoma in relation to the expression of vascular endothelial growth factor and thymidine phosphorylase. Anticancer Res 24(3b): 1853-1859.
-
Li X, Zhu X, Wang Y, Wang R, Wang L, et al. (2019) Prognostic value and association of Lauren classification with VEGF and VEGFR‑2 expression in gastric cancer. Oncol Lett 18(5): 4891-4899.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet